











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The Mexican Encuesta Nacional de Salud (ENSA, National Health and Nutrition Survey),1 reported a prevalence of arterial hypertension in the adult population of 31.5%, with 47.3% of these hypertensive subjects being unaware of their condition.1 In spite of increasing levels of awareness, an alarming proportion (49.8%) of known hypertensive patients remains uncontrolled.1 To effectively address this public health problem, significant improvements on the diagnosis and management of this condition as well as safe and effective treatment options are needed.
Fimasartan (FMS) is a newly developed angiotensin II receptor antagonist resulting from a bioisosteric replacement of losartan’s imidazole moiety with a pyrimidin-4(3H)-one part that confers this agent with the highest affinity to the AT1 receptor among drugs from this class (IC50 = 0.42 nM; Ki = 6.3E–11 M).2 Results from clinical studies in the Eastern-Asian population have shown that Fimasartan is not inferior and may be superior to losartan and valsartan,3,4 and that its antihypertensive effect is evident after two treatment weeks.5 FMS undergoes minimal hepatic metabolism, mainly by CYP3A4, which is well known for showing a marked genetic variability that may significantly influence drug disposition and therapeutic effect in different ethnic groups.6,7
The safety and efficacy of FMS have only been systematically explored in Eastern-Asian subjects, therefore, the above described potential for differences in drug disposition and the possibility for this agent to show different efficacy and safety profiles in the Mexican population8,9 require further assessment.
The purpose of this study was to evaluate the efficacy and safety of daily doses of 60 mg and 120 mg fimasartan, with or without 12.5 mg hydrochlorothiazide in Mexican subjects with essential hypertension grades 1–2.
Method and patients
Inclusion criteria
Subjects eligible to participate in the study were hypertension treatment naïve consenting adults, 18 years of age or older, with a baseline sitting diastolic blood pressure consistent with the diagnosis of grade 1 or 2 essential hypertension (diastolic blood pressure [DBP] ≥90 ≤109 mmHg). Not adequately controlled subjects already on monotherapy – provided that their treating physician considered them as suitable for a two-week washout period, were also eligible for the study.
Exclusion criteria
Subjects with grade ≥3 hypertension (systolic blood pressure [SBP] ≥180 mmHg and/or DBP ≥110 mmHg); secondary hypertension; uncontrolled type II diabetes mellitus (HbA1c > 9%); morbid obesity (BMI ≥40 kg/m2); renal dysfunction (creatinine ≥1.5 times above the upper limit of the normal range), liver dysfunction (aspartate aminotransferase and/or alanine aminotransferase ≥1.5 times the upper limit of the normal range), gastrointestinal or hematological diseases or conditions with a potential to affect the absorption, distribution, metabolism and excretion of the study drugs; a history of myocardial infarction, severe coronary artery disease or clinically significant congestive heart failure within 6 months prior to the screening visit; auto-immune or connective tissue disease and clinically significant laboratory test abnormalities according to the investigator’s judgment were not considered eligible to participate; additional exclusion criteria were the use of concomitant treatments which could affect blood pressure, known allergies or contraindication to the use of angiotensin II receptor antagonists, pregnant or breastfeeding women or in the case of women with childbearing potential, the rejection to use an effective contraceptive method (in accordance with the investigator’s judgment), a history of alcohol or drug abuse, clinical trial participation within 6 months prior to screening and any other reason which in the investigator’s opinion might contraindicate the participation of a subject in the study.
Method
Eligible patients spontaneously attending to 13 participating sites in Mexico were enrolled to participate in the 24-week study treatment period. Starting on Day 0, and after a two week washout period in the case of subjects already receiving monotherapy, all patients received oral FMS 60 mg once a day (q.d.) during the first 8 weeks of the planned treatment period. Patients with a DBP <90 mmHg at treatment week 8 continued receiving the same dose for up to 24 weeks; those with week 8 DBP ≥ 90 mmHg were then randomized to receive either FMS 120 mg q.d. or a fixed-dose combination tablet of fimasartan + hydrochlorothiazide (FMS/HCTZ) 60 mg/12.5 mg q.d. At week 12, patients randomized at week 8 maintaining a DBP ≥ 90 mmHg were escalated to open treatment with the fixed dose combination tablet of FMS 120 mg/HCTZ 12.5 mg q.d. for the remaining 12 weeks of the study (Fig. 1). At all visits, subjects were instructed to take one tablet of their assigned medication in the morning, with or without food.

Included subjects underwent a medical evaluation including physical exam, vital signs, safety laboratory analyses, assessments of treatment adherence (by means of tablet counting) and assessments of occurrence of adverse events at baseline and at treatment weeks 4, 8, 12, 16, 20 and 24.
Randomization Method. At the end of treatment week 8, subjects not achieving the target (DBP <90 mmHg) were randomized by means of a computer-generated randomization list (simple randomization with a 1:1 allocation ratio), to receive either FMS 120 mg q.d. or FMS/HCTZ 60 mg/12.5 mg q.d. The randomization sequence was administered by an independent third party, so that sponsor’s staff, investigators and enrolled subjects were blinded to the randomization list.
Blood pressure measurement was performed on the same arm at each clinic visit by either the principal investigator or designated medical personnel experienced and trained in the use of identical calibrated sphygmomanometers (Tycos 767, Welch Allyn) provided to each participating site with appropriate cuffs to accommodate the subject’s arm circumference. Subjects had to refrain from performing exercise and/or consume tobacco or coffee for at least 30 min prior to blood pressure measurements. Following 5 min of rest in the sitting position, the average of two consecutive blood pressure measurements (2 min apart from each other) was obtained with the individual and average results recorded on the subject’s charts.
Efficacy endpoints
The primary study endpoint was the change from baseline DBP at treatment week 8 (FMS 60 mg q.d). Secondary efficacy endpoints included week 8 SBP change from baseline, treatment-week 12 blood pressure changes from treatment week 8 (subjects randomized to FMS 120 mg q.d. or FMS + HCTZ 60 mg/12.5 mg q.d.), treatment week 24 blood pressure changes from treatment week 12 (non-responding randomized subjects escalated to daily FMS + HCTZ 120/12.5 mg doses at treatment week 12), blood pressure changes from baseline in subjects receiving 60 mg FMS q.d. during the 24 week treatment period and between randomized groups differences on treatment week blood pressure changes from treatment week 8.
Safety endpoints
Safety endpoints consisted on the incidence of adverse events, including clinically significant treatment emergent changes on vital signs, ECG parameters, and clinical laboratory measurements (complete blood counts, blood chemistry and urine examinations).
Statistical analysis
A sample size of 248 subjects was estimated as sufficient to detect a 1.4 mmHg difference in the change from baseline DBP between FMS and an assumed weighted mean change from baseline DBP of –8.375 mmHg for telmisartan as estimated from previously published results,10–16 assuming a DBP standard deviation of 6 mmHg; with 95% power and a two-tailed 5% significance level, using the sampsi command on Stata-12 (one sample comparison of mean to hypothesized value)17; a final sample size of 270 subjects was determined to account for an estimated 8% drop-out rate assumed based on the dropout rate observed in similar studies.10,11,16 Blood pressure changes from baseline and response rates were analyzed on an intention to treat (ITT) population consisting on all subjects taking at least one dose of study medication and one post-baseline blood pressure measurement using the multivariate normal procedure on NCSS10 (NCSS Statistical Software)18 to impute missing data. Safety analysis was performed on all subjects who received at least one dose of the study medications. To explore the robustness of the primary efficacy analysis, efficacy assessments were also conducted on a per-protocol population consisting on all subjects who completed the planned treatment period with no major protocol deviations (protocol deviations: DBP <90 mmHg at screening: 8 cases, included subjects with grade 3 [SBP >180 mmHg]: 3 cases, subjects assigned to an erroneous treatment at week 8: 6 cases, 1 subject erroneously assigned to treatment with FMS 60 mg + HCTZ 12.5 mg at week 4, 1 subject erroneously assigned to FMS 120 mg + HCTZ 12.5 mg at week 16 and 28 additionally withdrawn subjects). Within-group changes from baseline/reference point in time (i.e., week 8 for randomized subjects and week 12 for subjects escalated to the fixed dose combination of FMS 120 mg + HCTZ 12.5 mg q.d.) were analyzed using paired t tests, whereas differences between randomized treatment groups were analyzed using Student’s t tests in the case of independent means and relative risks in the case of proportions of subjects achieving therapeutic target in both groups. Blood pressure changes from baseline observed in the subset of patients treated with 60 mg FMS once daily over the 24 week treatment period were analyzed by means of repeated measures analysis of variance. We used two tailed tests performed at a 5% significance level.
Ethical considerations. This study was conducted in compliance with the principles established in the Declaration of Helsinki. The protocol was approved by the Commission for Sanitary Approval (CAS) of the Mexican Comisión Federal Para la Protección Contra Riesgos Sanitarios (COFEPRIS). Consent was granted by signing a written patient information and informed consent form, previously reviewed and approved by both relevant local ethics committees and the CAS.
Results
This study was conducted from April 2013 to August 2014.
Study population
Two hundred and seventy two (104 [38.2%] treatment naïve and 168 [61.8%] treatment experienced patients completing the planned washout period), eligible Mexican subjects, started the initial 8 weeks of planned treatment with FMS 60 mg q.d. with 33 subjects being withdrawn before completing the planned 24 week treatment period of the study (lost to follow-up: 17 [6.25%], consent with-drawal: 5 [1.84%], non-serious adverse event: 4 [1.47%], treatment non-compliance: 3 [1.10%], investigator’s decision: 1 [0.37%], conflict of interest: 1 [0.37%], serious adverse event: 1 [0.37%] and DBP <90 mmHg: 1 [0.37]); therefore 239 (87.9%) enrolled subjects completed the trial according to the study protocol (Fig. 2). Only five subjects where withdrawn because of the occurrence of non-serious and serious adverse events.

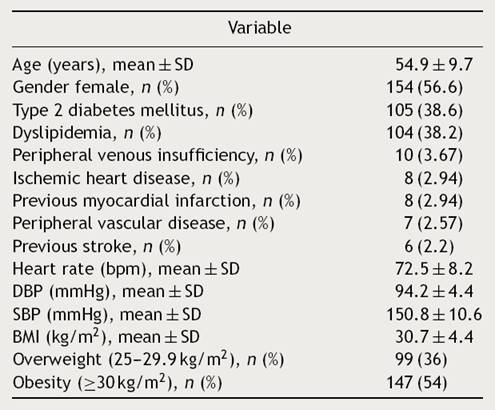
The study population comprised a broad range of patients with essential hypertension, including a significant proportion of subjects with co-morbidities such as obesity (with mean waist–hip ratios of 0.90 ± 0.07 and 0.97 ± 0.05 for female and male subjects, respectively), diabetes, dyslipidemia and coronary heart disease (Table 1). Estimated global assigned treatment adherence rate was 98.6%.
Efficacy
By treatment week 8, FMS 60 mg q.d. reduced both DBP and SBP by 11.3 ± 8.9 mmHg (p < 0.00001) and 16.0 ± 14.1 mmHg (p < 0.00001), respectively; with 75.4% (205/272) of the subjects achieving their treatment target (defined as a SiDBP <90 mmHg). By treatment week 12, 29 and 28 patients randomized to FMS 120 mg q.d. or to the fixed dose combination of FMS + HCTZ 60/12.5 mg q.d. showed significant blood pressure decreases from their week 8 values, with 58.6% (17/29) and 78.6% (22/28) subjects achieving treatment target. At week 12, twelve non-responding randomized subjects (8 from the FMS 120 mg q.d. and 4 from the FMS + HCTZ 60/12.5 mg q.d. groups), received FMS 120 mg/HCTZ 12.5 mg q.d. until the end of the planned treatment period and showed significant DBP and SBP reductions from their week 12 values, with 75% of them achieving treatment target by week 24 (Table 2).

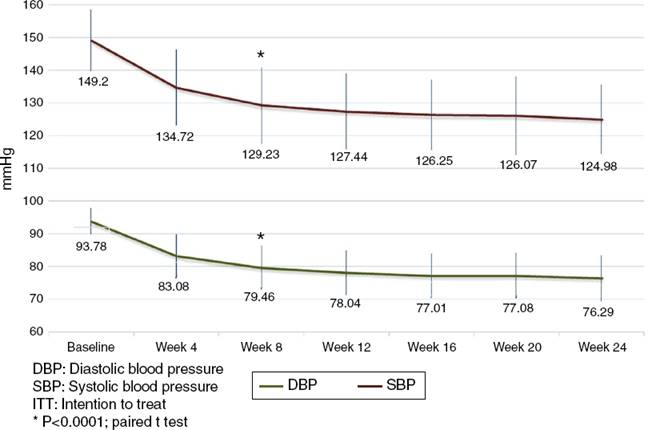
Analysis of the time course of the blood pressure lowering effect in the subgroup of subjects assigned to treatment with 60 mg fimasartan once daily throughout the study showed sustained systolic and diastolic pressure decreases which were statistically significant at all post-baseline assessments (i.e., p < 0.0001 for all pairwise comparisons between weeks 4, 8, 12, 16, 20 and 24 blood pressure decreases and baseline), with a trend to further blood pressure decreases throughout the study (Fig. 3). Of note, the treatment-to-target escalation strategy explored in this study resulted in a high proportion of participating subjects achieving both a DBP <90 mmHg and a SBP <140 mmHg (87.1%) by the end of the planned 24-week treatment period (Fig. 4).

Baseline comparison of subjects randomized at week 8 showed modest, non-significant differences between resulting groups with subjects assigned to FMS/HCTZ 60/12.5 mg being younger (53.1 ± 10.1 mmHg vs. 57.5 ± 8.2 mmHg, p = 0.073) and with a slightly lower baseline SBP (155.5 ± 9.5 mmHg vs. 158.7 ± 14.8 mmHg, p = 0.34) in comparison with subjects randomized to FMS 120 mg q.d. (Table 3). Between-treatment group comparisons showed that patients randomized to FMS/HCTZ 60/12.5 mg q.d. had greater reductions on both SBP and DBP which were not statistically significant (mean difference ± SD [95% confidence interval] of 2.51 ± 7.77 [–1.62, 6.63] and –4.49 ± 12.86 [–2.33, 11.32] for the DBP and SBP, respectively. In comparison with subjects assigned to FMS 120 mg q.d., the proportion of subjects assigned to FMS + HCTZ 60/12.5 mg q.d. who achieved treatment target was higher (12/29, 58.6% vs. 22/28, 78.6%); this difference was, however, not statistically significant (RR = 1.34 [95% confidence interval: 0.94, 2.01], p = 0.11).
Table 3 Subjects randomized at Week 8: baseline clinical characteristics (n = 57).
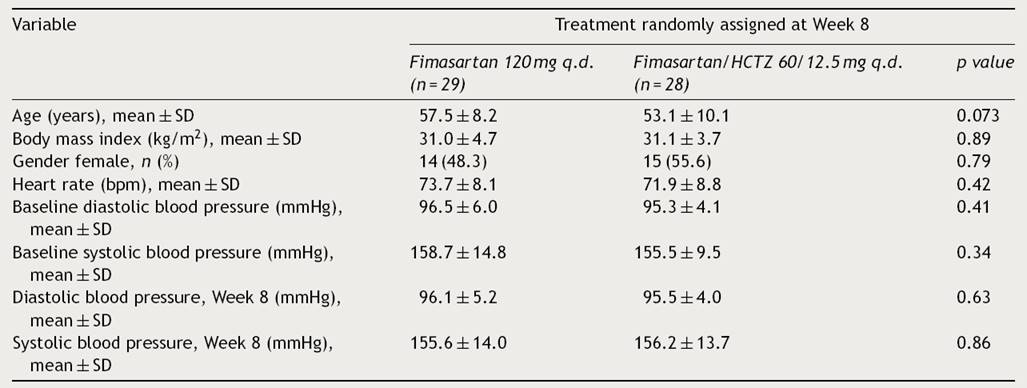
SD, standard deviation.
The exploratory analysis of changes from reference blood pressure values and response rates performed in the per protocol population (n = 225) was consistent with results obtained with the ITT population in terms of the magnitude of effect and statistical significance, thus supporting the robustness of the primary efficacy analyses (Supplementary Data).
Safety
During the whole study period, 64 of 272 subjects (23.5%) experienced 132 adverse events (AEs); most of which were mild to moderate in intensity (125/132 events, 94.7%) (Table 4). Adverse events considered as causally related with the study drugs by the participating investigators were identified in 25/272 (9.19%) subjects. The most frequent related AEs were headache (3.7%), dry mouth (1.1%), non-clinically significant, transient liver enzymes increase (1.1%) and dizziness (0.7%). Two non-serious events (0.7%) of hypotension attributed to FMS were reported, one event was solved with treatment discontinuation and the other resolved spontaneously. Three serious adverse events (one event of narrow angle glaucoma exacerbation and two events of traumatic bone fracture) were observed, all of which resolved with no sequels. None of the serious adverse events were considered by the investigators as related to the study drug. These observations are in accordance with previously reported results.3,4
Table 4 Treatment emergent adverse events.
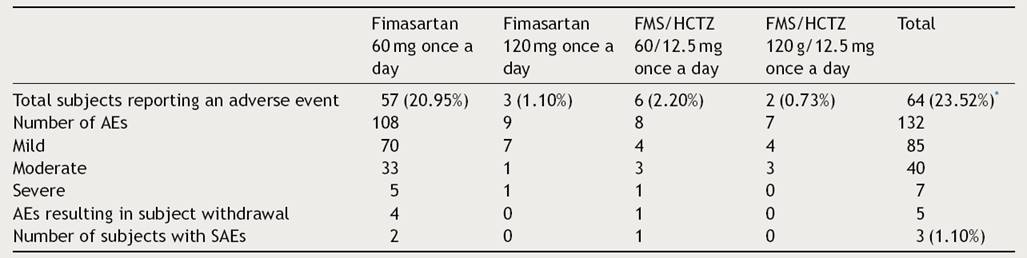
* 4 subjects reported the occurrence of adverse events (AEs) during the initial treatment period with fimasartan 60 mg once a day and during their subsequent treatment with either fimasartan 120 mg once daily, or with fimasartan/HCTZ at doses of 120 mg/12.5 mg once daily.
Non-clinically relevant changes of serum creatinine and potassium (K+) were observed. Serum creatinine change from baseline at week 24 was 0.02 ± 0.1 mg/dL (from a baseline value of 0.83 mg/dL) while serum K+ change from baseline at week 24 was 0.06 ± 0.40 mEq/L (from a baseline value of 4.11 mEq/L). No adverse events related with clinically significant changes of serum Cr and/or K+ values were observed.
Discussion
A series of observational studies and clinical trials indicate that commonly used antihypertensive agents may produce variable blood pressure lowering responses and potentially differing long-term outcomes in different ethnic populations when used as monotherapy.8,19–21 Still, specific information on the safety and efficacy of available antihypertensive medications – both in terms of blood pressure lowering effects and clinically relevant outcomes, in diverse ethnic groups is lacking.22 Data on the efficacy and safety of antihypertensive agents, specially ARBs, among Mexicans remains limited due to the under-representation of this population in clinical trials; with most of the data primarily restricted to retrospective subgroup analyses.23,24 The results of our study represent a contribution toward filling this gap.
In this Mexican experience with grade 1–2 essential hypertension subjects, FMS monotherapy at a dose of 60 mg q.d. resulted in sustained, clinically and statistically significant blood pressure reductions from baseline with 75.4% of subjects achieving the DBP treatment target (DBP <90 mmHg). Interestingly, rather than showing an additive blood pressure lowering effect of subsequent treatment escalation, our treat to goal escalation strategy allowed the identification of subsets of non-responders at weeks 8 and 12 with blood pressure levels very similar to their baseline values and who eventually showed clinically relevant blood pressure value decreases with subsequent treatment escalation, resulting in a high proportion of subjects (87.1%) achieving both a DBP <90 mmHg and a SBP <140 mmHg. We think that this response pattern merits further analysis to determine whether other factors such as renin-angiotensin system-related polymorphisms may influence treatment response in this population.
In conducting this experience, we sought to obtain a reliable estimate of FMSs blood pressure lowering effect in a sample of Mexican subjects by systematically studying a patient cohort based on the same general selection criteria used during the phase III assessment of the efficacy and safety of the drug in the Korean population.3,4,25 The resulting estimates for both DBP and SBP 8 week change from baseline with FMS 60 mg q.d. in our experience were consistent with those published by Lee et al.3 (–11.3 ± 8.9 vs –11.0 ± 7.6 and –16.0 ± 14.1 vs –17.8 ± 12.5, respectively) and similar to those reported by Lee H. and Kim K.S. et al.4 (–11.3 ± 8.9 vs. –14.0 ± 7.2 and –16.0 ± 14.1 vs 18.9 ± 9.0, respectively), thus supporting the notion of a similar efficacy of FMS in both the Korean and Mexican population.
The above results are consistent with our initial assumption of minimal to no effect of intrinsic ethnic factors on the tolerability and efficacy of FMS based on its linear pharmacokinetics, flat efficacy/concentration curve, wide therapeutic dose range (which suggest a low potential for differences in tolerability among differing ethnic groups), its minimal hepatic metabolism and low potential for drug-drug interactions as described on the ICH guidance document E5R1 regarding the acceptance of foreign data,26 and supports the usefulness of this document as a guidance for the regulatory acceptance of foreign clinical data.
Observed differences in terms of the blood pressure lowering effect between subjects randomized to 120 mg FMS q.d. or to 60/12.5 mg FMS/HCTZ q.d., are consistent with existing evidence of a superior effect of combined treatment over monotherapy up-titration,27 but lacked the power needed to reach statistical significance; considered in the context of existing evidence, this result suggests that, in the absence of contraindications to the use of HCTZ, the FMS/HCTZ combination should be the preferred treatment escalation strategy for patients not responding to FMS monotherapy.
The safety and tolerability findings among this cohort of Mexican subjects exposed to FMS alone or in combination with HCTZ were similar to those observed during the initial clinical development of the compound in Korea.
Limitations of this study include its open and non-controlled nature and the fact that sample size estimation was not conducted to provide sufficient power for randomized treatment-group comparisons; the fact that the study was prospectively conducted in a cohort of subjects with a pattern of co-morbidities typically observed among Mexican essential hypertension patients, with a clearly defined ‘‘zero time’’ to determine eligibility and baseline characteristics, and selection criteria and statistical methods (e.g., ITT analysis) similar to those used in controlled clinical trials previously conducted with fimasartan allowed us to obtain estimates of the safety and efficacy of the drug consistent with those observed in Korean subjects.25

