











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkAnother autumn was coming on a Thursday morning when Mexico was browsing the newspaper and rushing the coffee before going to work.
It was September the 19th of 1985 at 7 am, and news included the recent episode of the icy battle between Ronald Reagan and Mikhail Gorbachev about the Star Wars project, the presidential tour of Miguel de la Madrid and the eternal delays of the stadiums preparation for the XIII Soccer World Cup, that would take place eight months later. However, there was no information about the proximity of that earthquake, greater than 8 MW strong, that would occur a couple of minutes later. That day, many people died as a result of huge landslides and other more because of an acute myocardial infarction due to panic. In medical literature, several authors have described the way how an earthquake is related with an increased incidence of myocardial infarction, however this association appears to be stronger than we thought.1
Occasionally and without any warning, our planet suddenly sneezes and causes a cataclysm of colossal dimensions, like the Krakatoa’s volcano eruption, the earthquake of almost 200 gigatons in Valdivia or the Tsunami in Indonesia. Our human body, as a faithful representative of Nature, may also experience cataclysms that severely alter us, but this time transformed into a vascular catastrophe, secondary to a thrombus formation which generates a chain reaction within the affected territory, usually the myocardium or encephalon. A first similarity between major earthquakes and acute atherothrombosis is that both events have a very low occurrence rate, and their consequences are immediate and catastrophic.
Therefore, geologists and physicians’ concern focuses on predicting these types of events, because when they have already occurred, it is usually too late. Chávez-Domínguez and colleagues demonstrated in 2003 that 92% of patients who died due to a heart attack in Mexico did not received any attention from health services because they died at home, at work or on the street.2
Science of seismology studies the continuous movement of the earth’s crust and records it, minute by minute, in the different centers located throughout our planet. Earth-quakes occur daily, and when scientists plot their apparition over the years (time domain), it is very difficult to determine some dynamic pattern. However, if we change our perspective to a frequency-domain point of view, using the Fourier transform, we can observe that earthquakes faithfully obey the Power Law, which is date independent. This distribution shows us roughly, that there will be an enormous amount of small quakes and a very low occurrence of great ones, see Fig. 1. Now the problem is, despite having collected and analyzed trillions of terabytes of information about it, large earthquakes continue to appear unpredictably, especially over time.3
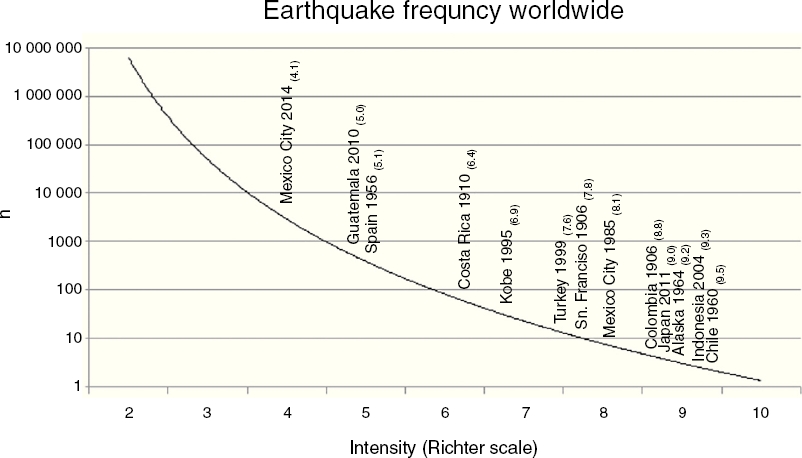
Figure 1 Atherothrombosis and earthquakes follow the power law. This plot shows earthquakes occurrence according to their magnitude, lower intensity, higher frequency and vice versa.
In other order of ideas, atherothrombosis has been extensively studied since the first descriptions by von Rokintansky and Virschow, concepts that later were taken up by Ross and that currently constitute the basis of vascular syndromes’ treatment and prevention. Atherosclerotic lesions accompany human beings since childhood, and they can remain harmless for years, as we see in subjects with multiple atheroma who never had a thrombotic event and who eventually died because of a non-cardiovascular etiology. However, some of these plaques are under a great metabolic and inflammatory stress that one day they can no longer resist, suffering an intimal rupture and generating an imbalance between the pro- and antithrombotic mechanisms of the endothelium. This process can produce a complete arterial occlusion and a wave of ischemia through the tissue at risk.4 Atherothrombosis also follows the power law, as far as many microscopic thrombi can initially appear, but finally they will be destroyed. In contrast, sometimes one or two large thrombi get stable and can cause acute and severe ischemia by occluding the artery that irrigates an important territory. Although this cascade of events has been extensively studied by experts for decades and despite the in-depth analysis of all this information, no method has been able to accurately predict the timing and location of a heart attack. How many times has a patient suffered an acute myocardial infarction under the surprised eyes of his physician?5
Ironically, large earthquakes are also caused by a structural rupture, but of a tectonic plate, which usually have their origin in pre-existing faults located in the earth’s crust. These quakes occur when the stress of a couple of tectonic plates, which has gradually increased for years, suddenly causes a huge plate-movement and the subduction of one plate under the other. Thus, that rupture in a small nucleation zone, displaces the plates and radiates megatons of energy as seismic waves along the surface of the fault.6
Therefore, both earthquakes and heart attacks are the result of a continuous process of stress that under certain circumstances, is liberated in an unpredictable, irrepressible and irreversible way.
The main shake of an earthquake causes the greatest structural damage, especially if it is prolonged. At the end of an earthquake several complications appear, worsening situation: landslides, tsunami, gas leaks, fires, blackouts, loss of communication lines, fractures in the streets and an imminent sanitary contingency. Immediately, emergency services take part, particularly civil protection units that react by rescuing injured, reducing collateral damage and housing the population, by delivering humanitarian and financial support. Finally, everything ends when the affected area is rebuilt, a task that partially lies on people’s resilience that means how quickly a community can recover from earth-quake damage.
Similarly, coronary atherothrombosis damages the heart structure in several ways: inflammation and cellular necrosis, loss of heart rhythm, conduction system blockage or the rupture of valvular and ventricular components. If patient reaches hospital, emergency services would be triggered to relieve ischemia, limit damage and injured tissue will be finally repair with a scar.
In both cases, events could not be precisely predicted and interventions were only reactive to catastrophe. Although an earthquake cannot be avoided, too many lives could be saved by evacuating the area well in advance, only if we can predict it. Unlike earthquake, it is thought that heart attack could be avoided.
A group of seismological scientists are focused in earthquake prediction, based on two methodology types: analysis of diagnostic precursors, widely studied because of its potential utility in the forecast of short-term earthquakes (<1 year). Second type are trend methods, useful for intermediate (1–10 years) or long-time prediction (10–100 years). Earthquake occurrence is an independent and probabilistic phenomenon that means it has no memory. The International Commission on Earthquake Forecasting for Civil Protection (ICEF) published a very heterogeneous list of methods to analyze earthquake precursors, including: changes in deformation rates, fluctuations in groundwater levels, changes in radon concentrations (soil, groundwater and air), electromagnetic variations of the Earth’s surface, thermal anomalies, seismic waves patterns and abnormal animal behavior associated their perception of seismic P waves. Trending methods study the statistical recurrence of quakes, supported by the study of seismographic, historical and paleontological records. Temporal accuracy of this approach ranges from 500 to 2000 years. Some faults on earth’s crust present multiple modes of periodicity. Our main problem is that earthquakes cannot be predicted with a time accuracy shorter than decades, and therefore medium-and short-term forecasts, have always a low probability to confer benefits in terms of civil protection.
Physicians have developed several coronary risk calculators, based on statistical associations obtained from cohort studies (Framingham, etc.), models that promise to be a useful tool to predict cardiovascular adverse outcomes at medium and long-term follow-up (10 years). Predictive variables are usually considered as demographic, nosological and biochemical risk factors, according to atherosclerosis and atherothrombosis pathophysiology.7 Similar to telluric movements, predictions about acute myocardial infarction can be more reliable for long periods of time (decades), but when clinicians try to use it as a short term forecast, these mathematical models lose accuracy.
Outcome prediction in cardiology and seismology accepts the epistemic basis that atherothrombosis and earthquake are a linear, deterministic, reductionist and probabilistic phenomena.
Predicting location of these kinds of events could be more accurate than forecasting time. If adequate seismic and geological data are available, particularly for those areas with a well delineated cortex faults pattern, it is relatively easy to predict where the epicenter will take place. Talking about ischemic heart disease, CT-scan coronary calcium-score allows physicians to identify those arterial territories that are more likely to have an occlusive atherothrombotic event and a heart attack. Other methods for establishing patient’s prognosis include nuclear medicine, stress echocardiography and coronary angiography.
Within time domain, earthquakes tend to occur very closely one to another, grouped in shaking sequences that gradually increase their magnitude (foreshocks) until the most intense earthquake occurs (main shock), followed by a series of aftershocks. Seismology experts also assume that the clusters of foreshocks and aftershocks have a Poisson distribution. When a rate of seismicity is high but without a clear main shock, the sequence is called an earthquake swarm. Geologists think that a better seismographic patterns understanding would improve the short-term quakes predictability, particularly the study of foreshocks behavior. However, these ground waves are practically indistinguishable from the background seismicity of Earth’s crust. Researching teams are currently generating earthquake forecasting-models, like Epidemic-Type After-shock Sequence (ETAS), a combined tool that integrates three seismic scales: Utsu, Omori and Gutenberg-Richter. Historically, only a couple of earthquakes have been well predicted, and the most famous case of an imminent prediction was the Haicheng earthquake (China) on February 4th 1975, where a large population was safely evacuated several hours before the main shake of the earthquake. Nevertheless, this forecasting has been widely questioned and similar schemes of prediction have been unable to succeed.
Today, when science is unable to predict earthquake’s location, timing or intensity; all we have are specialized systems looking for a rapid and effective response to a cataclysm. Alarm casting procedures should be standardized to take better decisions at different levels of government and among the public. One strategy is called Seismic Alert and it has been designed to reduce potential complications due to massive structural destruction, by timely evacuation of the population at risk. Since 1986, the Center for Instrumentation and Seismic Record (CIRES) has implemented this alert system based on the detection of large earthquakes, using sensors located in the already recognized epicenters, particularly at the Mexican southern coasts. CIRES equipment sends a coded signal that is captured by the Personalized Seismic Alert System (SASPER) and it is subsequently re-transmitted to the population at risk using massive electronic information media. Cities with this Anti-Seismic Accelerometer Network are mainly located in the Valley of Mexico, Guerrero and Oaxaca. This electronic warning provides Mexico City about 40 s for people evacuation to safety areas, before the main shock arrives.
Something similar happens with acute coronary syndromes, which initially emit their clinical alert (angina, syncope, etc.) that is repeated through emergency systems activation. The newest form of this action is known as Myocardial Infarction Code that has been structured using smartphone platform and social networks. This biological alarm has been triggered when atherothrombotic process is irreversible, and from then, all attempts will be directed to relieve ischemia, reduce collateral damage and treat complications.
Furthermore, there is another reactive strategy to prevent or to treat life-threatening arrhythmias, tightly associated with myocardial infarction, a program called cardio-protected areas. Electrical therapy for ventricular fibrillation or tachycardia has reduced dramatically short-term mortality due to malignant arrhythmias; this effect has been reinforced with standardization of cardiopulmonary resuscitation maneuvers (ACLS). Those ancient defibrillators evolved into modern semiautomatic devices, that have left intensive care units and came out into out-of-hospital setting. Defibrillation is one of the most effective therapies when is applied rapidly and appropriately. Now, the question is: how to provide the required number of devices to assure that people at risk? The main trouble is that population’s distribution also obeys power law. Thus, there are very few places where a lot of people are together, often only for short time (football stadium, airports, etc.), while almost all individuals are not concentrated, but dispersed over several square kilometers (houses, cars, etc.). Recently, a new strategy came out, based on coupling small defibrillators with an unmanned aerial vehicle (UAV), commonly known as a drone. This hybrid device could arrive very quickly into a cardiac-arrest site, almost wherever the patient is. All these new technologies could resolve some troubles around myocardial infarction, but in a very limited way.
Scientists have developed several theories and statistical tools to predict earthquakes or heart attacks. Although these models seem to have plausible arguments to forecast, in practice they have been unable to fulfill their task. Geophysics believes that earthquake prediction is possible, based on non-seismic physical precursors. On the other hand, cardiologists also think that a myocardial infarction could be even avoidable, if we identify and reduce patient’s risk factors. Nevertheless, other colleagues are pessimistic about these considerations and they think that these predictions are intrinsically erroneous.
This discrepancy led researchers to look for new manners of data interpretation and to postulate more realistic theories. Several decades ago, scientists have described how nature does not have a linear, deterministic, reductionist or closed behavior. Natural phenomena follow an intricate path, composed of innumerable interactions, trending lines that sometimes go together and some other they diverge in an apparently capricious way, but finally they weave a dense tissue of probabilities, facts and conjectures. Edgar Morin calls this type of interactions complexity, from Latin: complexus (interlaced).
One of the most accepted theories for earthquake onset describes how continental-drift dynamics presents several types of fluctuations in tectonic plates load, which generate self-organization and resonance phenomena. This mechanical behavior can result in emergent properties, such as an earthquake. Seismic pattern has a clearly complex and non-linear behavior, which needs to be studied with appropriate methods and new mathematics.8 Earthquake-prediction experts note that, if we use forecasting models in a incorrectly way, they can introduce epistemic uncertainty.
Analogously, there are cardiology study-groups interested in non-linear dynamics, and they are researching topics like: atherosclerotic plaque formation, circulation patterns of blood elements and life-threatening arrhythmias genesis.9 Earthquakes and atherothrombosis are irreversible phenomena and this fact suggests that both could present, thermodynamically, high levels of entropy.
The lack of accurate forecasting-models forces us to take a more realistic approach. Thus, the most accurate and effective way to deal with this problem, whether it be an earthquake or a heart attack, is to implement a specific and fast intervention, once the event just happened. Engineers are already designing seismic-resistant buildings, based on their complex and non-linear behavior during an earthquake. Physicians have by now, emergency systems like Myocardial Infarction Code or cardio-protected areas. However, these interventions are only symptomatic and palliative: we cannot yet establish any relevant measure to prevent a natural disaster.10
In summary, earthquakes and atherothrombosis are more similar than we thought, because they are unpredictable, irrepressible and irreversible. We need a new approach, like complexity sciences, for studying these problems in a trans-disciplinary teamwork that could bring us a brightly light in this dark scenario. Just imagine what could happen if physicists and physicians join their efforts in an interactive research to accurately predict a natural cataclysm, whether it be an earthquake or a heart attack. . .

