










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkArchivos de cardiología de México
On-line version ISSN 1665-1731Print version ISSN 1405-9940
Arch. Cardiol. Méx. vol.76 n.4 Ciudad de México Oct./Dec. 2006
Comunicaciones breves
Troponin I release at rest and after exercise in patients with hypertrophic cardiomyopathy and the effect of betablockade
Liberación de troponina I en reposo y con ejercicio en sujetos con miocardiopatía hipertrófica. Efecto de betabloqueadores
Gheorghe AM Pop,* Etienne Cramer,* Janneke Timmermans,* Hans Bos,* Freek WA Verheugt*
* Heartcenter, Radboud University Medical Centre, Nijmegen, The Netherlands.
Correspondence to:
Dr Gheorghe AM Pop.
Heartcenter, Radboud University Medical Center Nijmegen.
Geert Grooteplein 8,
6500 HB Nijmegen.
The Netherlands
Telephone: +31 24 3614533 Fax: +31 24 3540537
E–mail address: g.pop@cardio.umcn.nl
Recibido: 8 de mayo de 2006
Aceptado: 21 de septiembre de 2006
Summary
Purpose of the work: In patients with hypertrophic cardiomyopathy ischemia may occur due to massive heart weight, myocyte disarray or small vessel disease. We detected elevated troponin levels in some of these patients and hypothesized that troponin release would rise after exercise and diminish after betablockade.
Methods and results: In 5 of 7 young patients (6 males) with hypertrophic cardiomyopathy and no overt coronary artery disease we found elevated troponin levels after physical exercise; the peak was between 6 and 9 hours and levels returned to pre–exercise values within 24 hours. Troponin release was consistently diminished after use of a betablocker.
Conclusions: Increased troponin release may be present in patients with hypertrophic cardiomyopathy and is temporarily enhanced by exercise and diminishes with betablockade.
Key words: Hypertrophic cardiomyopathy. Troponin. Exercise. Betablocker.
Resumen
Objeto: En sujetos con miocardiopatía hipertrófica puede presentarse isquemia por el aumento de la masa miocárdica o desorganización de los miocitos o alteraciones de los pequeños vasos. Nosotros hemos encontrado niveles elevados de troponina I en algunos de estos enfermos y creemos que la liberación de troponina puede aumentar tras un ejercicio físico y reducirse por acción de betabloqueadores.
Métodos y resultados: En 5 de 7 jóvenes con miocardiopatía hipertrófica y arterias coronarias epicárdi–cas normales hemos encontrado niveles elevados de troponina I tras un ejercicio físico. El nivel máximo se alcanzó entre 6 y 9 horas y los niveles de base se restablecieron dentro de 24 horas. La liberación de troponina se redujo consistentemente con la administración de betabloqueadores.
Conclusiones: Una liberación elevada de troponina I puede presentarse en pacientes con miocardiopatía hipertrófica y acentuarse transitoriamente con el ejercicio, reduciéndose por efecto de betabloqueadores.
Palabras clave: Miocardiopatía hipertrófica. Troponina. Ejercicio. Betabloqueadores.
Introduction
Troponin measurements have shown to be of paramount importance for the diagnosis and risk stratification of patients with (suspected) cardiac disease, especially ischemic heart disease.1 In patients without evidence of active myocardial ischemia or other known causes of troponin elevation a correlation was found between an increased troponin level and left ventricular mass index.2 The same correlation has been demonstrated in an animal model of cats with hypertrophic cardiomyopathy.3
In patients with hypertrophic cardiomyopathy ischemia may occur due to massive heart weight, myocyte disarray or small vessel disease.4–6 We found elevated troponin levels in several patients with hypertrophic cardiomyopathy. If myocardial ischemia would be the explanation of the presence of elevated troponin levels, we hypothesized that troponin release in these patients should increase during exercise and betablockade should reduce this release.
Material and methods
Seven young patients (6 males, 1 female; mean age 34 years) with echocardiographically diagnosed obstructive (n = 4) and non–obstructive (n = 3) hypertrophic cardiomyopathy gave informed consent to participate in this pilot study. In 4 of 7 patients cardiac catheterization has been performed and revealed normal epicardial coronary arteries. In the other 3 patients no catheterization was done, but no risk factors for IHD nor symptoms or ECG signs that would suggest ischemic heart disease were present.
Patients underwent blood sampling for determination of baseline levels of cardiac troponin I (Immulite 2000; Diagnostic Products Corporation Breda, The Netherlands) and cardiac troponin T (Roche Diagnostics, Almere, The Netherlands). In addition CK and CK–MB were assessed.
According to our protocol all patients were to undergo a bicycle exercise tests between 70% and up to 120% of their predicted workload (in Watts) without the use of any betablocker therapy. After each exercise test repeat measurements of cardiac biomarkers in peripheral venous blood were determined at 3, 6, 9 and 24 hours. If a rise and fall of troponin was detected after exercise, a second test was done under medication of either metoprolol 200 mg (4 patients) or atenolol 100 mg (3 patients) on a daily basis. It was planned, that a similar workload (in Watts) was performed with and without betablocker medication. Tests were interspaced by at least 5 days and always done in the morning.
Results
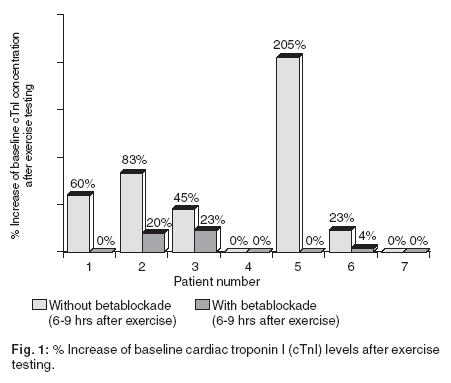
Exercise test and biomarker results are shown in Table I. In patients 4 and 7 no rise of troponin I occurred during exercise without betablocker; the other 5 patients performed a similar workload (in Watts) without and with betablocker therapy. While on betablocker therapy these patients reached at least 20% less rate–pressure product at peak exercise for the same workload (in Watts) as without medication. Patients 2, 3 and 6 had already elevated troponin I levels at rest. Strikingly, without betablockade 5 of 7 patients showed an early increase (< 3 or 6 hours) in troponin I levels after exercise. In contrast, after pre–treatment with a betablocker troponin I release was reduced in all patients, who had troponin elevation at rest and/or after exercise. In two patients (1 and 5) troponin I concentrations became undetectable. Surprisingly, cTnT as well as CK–MB were only elevated in patient 2, who had the highest troponin I levels. CK–MB and cTnT release decreased after betablockade in this patient.
In Figure 1 troponin I levels are depicted as relative increases with respect to baseline concentrations after exercise testing both without and with betablockade. The peak levels were between 6 and 9 hours and returned to pre–exercise values within 24 hours.
Discussion
To our knowledge, this study demonstrates for the first time that troponin release above normal values may be present in young patients with hypertrophic cardiomyopathy without overt coronary heart disease. In 3 patients baseline levels were already elevated and further increased after exercise. In 2 other patients without a measurable troponin I level at baseline, moderate physical exercise induced an early and temporary rise of troponin I. Interestingly, whereas troponin I release occurred in 5 of 7 patients, troponin T release occurred in only one.
Previous studies have shown that coronary microvascular dysfunction, massive heart weight and myocyte disarray are associated with an unfavourable outcome in patients with hypertrophic cardiomyopathy.4–6 Interestingly, these factors seem to have one common denominator: they are determinants of mismatch between oxygen demand and supply, which seems an obvious explanation of troponin release in our patients with hypertrophic cardiomyopathy.
Ischemia however being the cause of a positive troponin in patients with hypertrophic cardiomyopathy is different from that of a positive troponin occurring in the setting of coronary artery disease, where ischemia occurs primarily due to thrombo–occlusive events. This different etiology of ischemia may explain, why troponin release in patients with hypertrophic cardiomyopathy during exercise is early (< 3 or 6 hours), lasts for approximately 24 hours and is not characterized by the more gradual washout seen in patients with vessel occlusion. Our finding of temporary rise of troponin level in young patients with hypertrophic cardiomyopathy also puts in doubt, whether rise of troponin is always a marker of myocardial necrosis. The rise of troponin in these patients might be due to continuous gradual loss of myocardial cells,7 being one explanation why most patients with hypertrophic cardiomyopathy end up in heart dilatation. However, Wu et al have shown that myocardial ischemia may also cause temporary release of troponin from the intracellular cytosol due to cell membrane leakage.8 In ischemic heart disease troponin release has been shown to be an independent predictor for future outcome.1 Whether the same is true for patients with hypertrophic cardiomyopathy should be subject in further investigation.
In ischemic heart disease the rate–pressure product is a reliable index of myocardial oxygen consumption9 and betablockers decrease the mismatch between oxygen demand and supply. Assuming that troponin release in patients with hypertrophic cardiomyopathy is based on the mechanism of myocardial oxygen mismatch, it is not surprising that our study demonstrated a reduction of troponin release after betablocker medication. Furthermore, in heart failure betablockers have shown to slow progression to congestive failure.10,11 Exercise studies in dogs with hypertrophic left ventricle demonstrated a better transmural myocardial blood flow at lower heart rates.12 Loss of contractile force in patients with hypertrophic cardiomyopathy, as expressed by continuous or intermittent troponin release, might be prevented by continuous betablockade, which should also be subject to further clinical research.
Finally, stress testing has shown to be safe in patients with hypertrophic cardiomyopathy. Our findings of rising troponin levels after exercise seem in concordance with the newest guidelines for patients with hypertrophic cardiomyopathy to avoid competitive sport. Maybe measurement of troponin levels after exercise may provide a guide in the amount of physical exercise that will be permitted in these patients.
Conclusions
Increased troponin release may be present in patients with hypertrophic cardiomyopathy. If present, we detected an early and temporarily rise after exercise in all of them. The elevation of troponin I at rest in some patients and the rise of troponin I after exercise could be diminished in all patients after pretreatment with betablockade. Further clinical studies are warranted to demonstrate that elevation of troponin at rest and/or exercise in patients with hypertrophic cardiomyopathy is a marker of worse clinical outcome. Betablockers may improve clinical outcome, especially if such troponin positive HCM patients are at highest risk.
References
1. Hamm CW, Ravkilde J, Gerhardt W, Jorgensen P, Peheim E, Ljungdahl L, Goldmann B, Katus HA: The prognostic value of serum troponin Tin unstable angina. N Engl J Med 1992; 327: 146–150. [ Links ]
2. Hamwi SM, Sharma AK, Weissman NJ, Apple S, Canos DA, Pinnow EE, Lindsay J: Troponin–I elevation in patients with increased left ventricular mass. Am J Cardiol 2003; 92: 88–90. [ Links ]
3. Connolly DJ, Cannata J, Boswood A, Archer J, Groves EA, Neiger R: Cardiac troponin I in cats with hypertrophic cardiomyopathy. J Feline Med Surg 2003;5: 209–216. [ Links ]
4. Cecchi F, Olivotto I, Gistri R, Lorenzoni R, Chiriatti G, Girolami F, Torricelli F, Camici PG: Coronary microvascular dysfunction and prognosis in hypertrophic cardiomyopathy. N Engl J Med 2003; 349: 1027–1035. [ Links ]
5. Spirito P, Bellone P, Harris KM, Bernabo P, Bruzzi P, Maron B J: Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyopathy. N Engl J Med 2000; 342: 1778–1785. [ Links ]
6. Varnava AM, Elliott PM, Mahon N, Davies MJ, McKenna WJ: Relation between myocyte disarray and outcome in hypertrophic cardiomyopathy. Am J Cardiol 2001; 88: 275–9. [ Links ]
7. Van der Laarse A: Hypothesis: troponin degradation is one of the factors responsible for deterioration of left ventricular function in heart failure. Cardiovasc Res 2002; 56: 8–14. [ Links ]
8. Wu AH, Ford L: Release of cardiac troponin in acute coronary syndromes: ischemia or necrosis? Review. Clin Chim Acta 1999; 284(2): 161–74. [ Links ]
9. Gobel FL, Norstrom LA, Nelson RR, Jorgensen CR, Wang Y: The rate–pressure product as an index of myocardial oxygen consumption during exercise in patients with angina pectoris. Circulation 1978; 57: 549–556. [ Links ]
10. CIBIS–II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS–II): a randomized trial. Lancet 1999; 353: 9–13. [ Links ]
11. MERIT–HF Study Group. Effect ofmetoprolol CR/ XL in chronic heart failure: metoprolol CR/XL randomized intervention trial in congestive heart failure (MERIT–HF). Lancet 1999; 353: 2001–2007. [ Links ]
12. Traverse JH, Altman JD, Kinn J, Duncker DJ, Bache RJ: Effect of beta–adrenergic receptor blockade on blood flow to collateral–dependent myocardium during exercise. Circulation 1995; 91: 1560–7. [ Links ]

