










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkArchivos de cardiología de México
On-line version ISSN 1665-1731Print version ISSN 1405-9940
Arch. Cardiol. Méx. vol.71 n.3 Ciudad de México Jul./Sep. 2001
Comunicaciones breves
Bystander coronary sinus diverticulum and left anterolateral accessory pathway
Abdel J Fuenmayor,* Abdel M Fuenmayor,* Lissette Aranguibel*
* Electrophysiology Section. Cardiovascular Research Center "Abdel M Fuenmayor P". University of The Andes. Mérida, Venezuela.
Correspondence
Abdel J Fuenmayor.
Apartado Postal 154, Mérida, 5101, Venezuela.
Phone and Fax number: Intern +58-74-447717.
E-mail: farocha@ing.ula.ve
Recepción: 26 de febrero de 2001.
Aceptado: 1 de junio de 2001.
Abstract
Left posteroseptal accessory pathways have been described inside coronary sinus diverticula. We here describe the case of a patient who was suffering from recurrent episodes of paroxysmal supraventricular tachycardia and had a concealed accessory pathway located in the left anterolateral margin of the mitral annulus and a left posterior coronary sinus diverticulum associated with an aneurysmal coronary sinus vein. In the electrophysiological study, an orthodromic supraventricular tachycardia was induced and reproduced. We performed a successful radiofrequency ablation of the pathway. Our case provides evidence of the coexistence of concealed accessory pathways capable of sustaining orthodromic tachycardia coexisting with a bystander posterior coronary sinus diverticulum and aneurysmal coronary sinus vein.
Key words: Bystander coronary sinus diverticulum. Concealed accessory pathway. Paroxysmal supraventricular tachycardia.
Resumen
Se han descrito fascículos accesorios postero-septales ubicados dentro de divertículos del seno coronario. Aquí describimos el caso de un paciente que sufría episodios recurrentes de taquicardia supraventricular paroxística causada por un fascículo accesorio oculto localizado en la región anterolateral del anillo mitral. En el paciente también había un divertículo del seno coronario asociado con una vena coronaria aneurismática. En el estudio electrofisiológico, se indujo una taquicardia supraventricular ortodrómica que utilizaba el fascículo accesorio descrito, por lo que se realizó una ablación exitosa del fascículo y la paciente se hizo asintomática. Nuestro caso da prueba de la coexistencia de fascículos accesorios ocultos (ubicados en sitios distantes) y de un divertículo del seno coronario y una vena coronaria aneurismática.
Palabras clave: Divertículo del seno coronario. Fascículo accesorio oculto. Taquicardia supraventricular paroxística.
Introduction
Left posterior accessory pathways have been reported to be associated with coronary sinus diverticula and/or middle cardiac vein anomalies.1 When this association is present, the accessory pathway was found in close proximity or within the coronary sinus diverticulum or the coronary vein branches.1-6 To our knowledge, there are no previous reports of the existence of a concealed left anterolateral pathway with a coronary sinus diverticulum and vein anomalies acting as bystanders. We report here the case of a patient with drug refractory supraventricular tachycardia due to a concealed left anterolateral accessory pathway in association with a coronary sinus diverticulum and an aneurysmal coronary sinus vein.
Case report: S.O. is a thirty eight year-old woman who came to our clinic because she was suffering from recurrent episodes (an average of 3 per week) of paroxysmal supraventricular tachycardia (Fig. 1) refractory to treatment with beta-blockers, verapamil and amiodarone. The patient accepted to be submitted to an electrophysiological study for diagnostic and, if indicated, therapeutic purposes (radiofrequency ablation). The physical examination and X-ray did not reveal abnormalities. The ECG did not display pre-excitation, and was within normal limits.

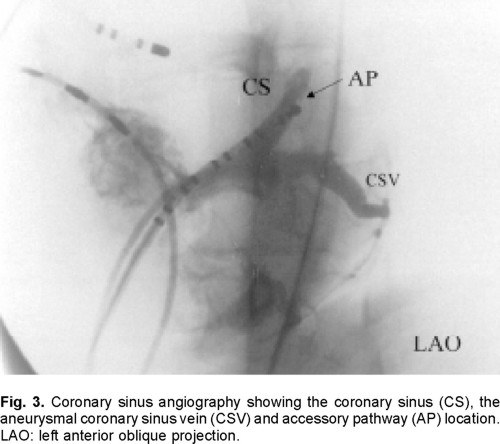
Electrophysiological study: During the programmed atrial stimulation, a reentrant tachycardia was induced (Fig. 2) with an eccentric (left-sided) ventriculo-atrial activation. During the tachycardia the mapping procedure evidenced the shortest V-A interval at the distal pair of electrodes of the coronary sinus catheter that was placed on the left border of the cardiac silhouette as displayed in the left anterior oblique projection. The shortest ventriculo-atrial time recorded in that position was 110 milliseconds. As it was difficult to advance the coronary sinus catheter beyond this point, we decided to perform a coronary sinus angiography that evidenced that the catheter was positioned in an aneurysmal coronary sinus vein (Fig. 3). After pulling back the angiographic, catheter, a second injection was performed and a coronary sinus diverticulum became evident (Fig. 4).


The electrophysiology mapping was carefully repeated making particular emphasis upon the coronary sinus diverticulum and the coronary sinus vein. The shortest V-A interval was found to be located in the anterolateral portion of the mitral ring (70 milliseconds) (Fig. 4).
Radiofrequency catheter ablation: The radiofrequency ablation was, performed with an Atakr RF generator system (Medtronic Inc., Minneapolis) and a Mariner ablation catheter (Medtronic Inc., Minneapolis). The supraventricular tachycardia was induced, and 1 second after the RF initiation the tachycardia stopped and could not be induced thereafter (Fig. 5). Under ventricular stimulation the ventriculo-atrial conduction became normal. The mapping procedure was repeated and no evidence of remaining accessory pathways was found. The programmed stimulation was then repeated after the patient was given a continuous intravenous infusion of adrenaline (50 ηg/kg/minute), but no tachycardia was inducible. The patient was discharged without complications, and six months later she still remains free of arrhythmia without receiving antiarrhythmic therapy.

Comment: Coronary sinus diverticula have consistently been reported in patients with the Wolff-Parkinson-White syndrome in whom the electrocardiographic pattern consists in deep negative delta waves in the inferior leads and an r/S pattern in VR, V5 and V6.7 Our patient's ECG was normal during the sinus rhythm, and the electrophysiological study did not reveal anterograde conduction through the accessory pathway; it could thus be inferred that the accessory pathway was of the concealed type.
The existence of an aneurysmal coronary vein misled the coronary sinus catheter away from the anterolateral portion of the left A-V ring, and made it difficult for us to obtain proper electrograms and intervals for guiding the ablation. We thus took the decision to perform a coronary sinus angiography that disclosed the coronary vein anomaly and the diverticulum that could have been missed otherwise.
Transesophageal echocardiography has been shown to be an alternative means of coronary sinus diverticula's diagnosis,8 but we did not perform it in our patient. Moreover, since we do not systematically perform coronary sinus angiography in all the patients who are submitted to radiofrequency ablation, the incidence of coronary sinus diverticulum and coronary vein anomalies is unknown. It is thus likely that the association of these anomalies is more frequent than suspected and that it goes undetected if a coronary sinus angiography or a transesophageal echocardiogram is not performed in patients submitted to electrophysiological studies.
The complications and therapeutic guidelines for the treatment of patients with coronary sinus vein anomalies that are not associated with accessory pathways are not well known, and more research is needed in this area. To our knowledge this is the first time a patient with a supraventricular tachycardia mediated by a concealed accessory pathway located in the left anterolateral portion and associated with coronary sinus vein anomalies is reported in the literature.
Conclusion
Our case provides evidence for the co-existence of a coronary sinus diverticulum and coronary sinus vein anomalies acting as bystanders and associated with concealed accessory pathways located outside the vein anomalies.
Acknowledgment
We are thankful to Françoise Meyer for her review of the manuscript.
This work was supported by grant Nº EQ-ESP-M-29-93 from Consejo de Desarrollo Científico, Humanístico y Tecnológico. University of the Andes.
References
1. Guiraudon GM, Guiraudon CM, Klein GJ, Sharma AD, Yee R: The coronary sinus diverticulum: a pathologic entity associated with the Wolff-Parkinson-White syndrome. Am J Cardiol 1988; 62: 733-35. [ Links ]
2. Shumacher B, Tebbenjohahhs J, Pfeiffer D, Omran H, Jung W, Luderitz B: Prospective study of retrograde coronary venography in patients with postero-septal and left-sided accessory atrioventricular Pathways. Am Heart J 1995; 130: 1031-39. [ Links ]
3. Omran H, Pfeiffer D, Tebbenhohanns J, Shumacher B, Manz M, Lauck G, et al: Echocardiographic imaging of coronary sinus diveticula and middle cardiac veins in patients with preexcitation syndrome: impact on radiofrequency catheter ablation of posteroseptal accessory pathways. Pacing Clin Electrophysiol 1995; 18: 1236-43. [ Links ]
4. Villacastin J, Merino JL, Almendral J, Arenal A, Tercedor L, Alberca T, et al: Radiofrequency ablation of a posteroseptal accessory pathway associated with coronary sinus diverticulum. Rev Esp Cardiol 1995; 48: 638-41. [ Links ]
5. Beukema WP, Van Dessel PF, Van Hemel NM, Kingma JH: Radiofrequency catheter ablation of accessory pathways associated with a coronary sinus diverticulum. Eur Heart J 1994; 15: 1415-18. [ Links ]
6. Lesh MD, Van Hare G, Kao AK, Scheinman MM: Radiofrequency catheter ablation for Wolff-Parkinson-White syndrome associated with a coronary sinus diverticulum. Pacing Clin Electrophysiol 1991; 14: 1479-84. [ Links ]
7. Haissaguerre M, Jais P, Shah DC, Takahashi A, Barold SS, Clémenty J: A conceptual approach to radiofrequency catheter ablation of accessory pathways focusing on electrogram criteria. In Singer I, Barold SS, Camm AJ (Eds.) Nonpharmacological therapy of arrhythmias for the 21st century. Armonk NY. Futura 1998: 57-87. [ Links ]
8. Hamilton K, Castillo M, Arruda M, Jackman W: Echocardiographic demonstration of coronary sinus diverticula in patients with Wolff-Parkinson-White syndrome. J Am soc Echocardiogr 1996; 9: 337-43. [ Links ]

