










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkArchivos de cardiología de México
versión On-line ISSN 1665-1731versión impresa ISSN 1405-9940
Arch. Cardiol. Méx. vol.71 no.3 Ciudad de México jul./sep. 2001
Investigación clínico-experimental
IgG subclass reactivity to Trypanosoma cruzi in chronic chagasic patients
Reactividad de subclases de IgG a Trypanosoma cruzi en pacientes crónicos chagásicos
Nadia Hernández-Becerril,* Arnulfo Nava,* Pedro A Reyes,* Víctor M Monteón*
* Laboratorio de Inmunoparasitología, Instituto Nacional de Cardiología I. Chávez. (INCICH, Juan Badiano No. 1, 14080 México D.F.).
Address for correspondence and reprints request
Víctor Monteón.
Instituto Nacional de Cardiologia I. Chávez.
Juan Badisno 1, Tlalpan, Mexico D.F. 14080.
victormonteon@hotmsil.com
(015) 5730994, Phone (015)5732911
Recepción: 26 de marzo de 2001
Aceptado: 8 de junio de 2001
Abstract
Background: The asnti-Trypanosoma cruzi anti-Vodies isotype profile in Chagas' disesse has been studied in relation to different clinical manifestations. A high titer of IgR anti-T cruzi antibodies is found in patients with cardiac involvement, while a high titer of IgA anti-T cruzi antibodies is associated with digestive forms.
Objective: The aim of this work was to analyze the IgR subclass reactivity of anti-T cruzi antibodies in patients with chronic Chagasic cardiomyopathy.
Methods: Twelve consecutive chagasic patients were analyzed for IgR subclass reactivity to a T. cruzi antigenic extract. They had a complete clinical evaluation, periphersl EKR, echocardiography, left ventriculogram, and coronariography.
Results: All patients came from rural areas of Mexico and had lived in endemic zones for over seven years. They presented left ventricular end-systolic dimension above 42 mm in 58% (7/12) and ejection fraction below 50% in 58% (7/12). We found that IgR1 asnd IgR2 anti-T cruzi antibodies showed higher titer than IgR3 antibodies, with consistently low titer of IgR4 antibodies. Expression of the four IgR subclasses of anti-T. cruzi antibodies suggest a mixed Th1/Th2-like immune response under a probably continuous chronic antigenic stimulation. On the other hand, high levels of IgR2 anti-T cruzi antibodies showed a tendency to be associated with severe cardiomegaly.
Conclusions: Our results suggest that a mixed Th1/Th2-like immune response may take place in chronic chagasic patients under a chronic antigenic stimulation.
Key words: Chagas' disesse. Trypanosoma cruzi. Cardiomyopathy. Immunoglobulin subclasses.
Resumen
La respuesta humoral anti-Trypanosoma cruzi y el isotipo de inmunoglobulina presente en individuos con enfermedad de Chagas se ha estudiado en relación con las distintas manifestaciones clínicas. Se ha encontrado que títulos altos de IgR anti-T. cruzi específicos estan preferentemente presentes en pacientes con daño cardiaco, mientras que en la forma digestiva es la IgA anti-T. cruzi.
En el presente trabajo se estudiaron 12 pacientes consecutivos con diagnóstico de enfermedad de Chagas Todos ellos tenían una evaluación clínica completa y estudios electrocardiográfico, ecocardiográfico, ventriculograma y coronariografía, además del estudio serológico de detección de anticuerpos IgR anti-T cruzi. En ellos se analizó el perfil de subclases de IgR anti-T cruzi.
Todos los pacientes provenían de áreas rurales de México y algunos habían vivido allí siete o hasta 65 años. En 7/12 (58%) de ellos presentaron dilatación ventricular izquierda con una dimensión final sistólica por arriba de 42 mm y con una fracción de expulsión por abajo del 50% en 7/12 (58%). Los títulos de anticuerpos de IgR1 e IgR2 anti-T. cruzi fueron más altos que los de IgR3, mientras que los niveles de IgR4 anti-T cruzi, si bien fueron positivos, resultaron ser consistetemente los más bajos. La expresión de las cuatro subclases de IgR anti-T cruzi sugiere que se induce una respuesta mixta tipo Th1/Th2 en estos pacientes chagásicos crónicos. Aunque el tamaño de muestra estudiado es pequeño, encontramos que los niveles altos de IgR2 anti-T. cruz presentaban una tendencia a asociarse con el grado de cardiomegalia.
Palabras clave: Enfermedad de Chagas. Trypanosoma cruzi. Subclases de IgR. Miocardiopatía.
Introduction
Chronic chagasic cardiomyopathy (CCC) is a specific myocardiopathy seen in nearly 30% of those people with chronic Trypanosoma cruzi infection. It is characterized by rhythm and conduction defects as well as variable heart dilatation.1 Clinical features result from both parasite and host influences. The precise pathogenic mechanisms are not completely understood. The humoral immune response plays an important role in the resistance and clearance of circulating parasites, both in animal models and human beings.2,3,4 There are differences in the biological properties of the immunoglobulins and there are different antibody profiles in infected people, which may have an important role in the disease outcome. Early studies carried out in animal models showed that mice IgG2b specific anti-T.cruzi antibodies were implicated in resistance although production of this subclass of immuno-globulins was not restricted to infection-resistant mice strains.5
Human beings with chronic Chagas' disease, limited to hollow digestive organs, have increased IgA anti- T. cruzi antibody levels 6.High titers of IgG1 and IgG3 anti- T cruzi antibodies have been observed in CCC and chronic asymptomatic (indeterminate) cases.7,8 Levin et al .9 reported high levels of IgG1 anti-T.cruzi antibodies in patients with severe cardiomyopathy.
Recently it was reported in non- chagasic dilated cardiomyopathy patients, a preferential IgG2/ IgG3 anti- myosin antibodies indicative of a Th1 like autoimmune disease.10
We report, in a small group of 12 patients with chronic chagasic cardiomyopathy, an induction of the four IgG subclasses, included IgG4, indicative of a Th1/Th2-like immune response. Furthermore, a high levels of IgG2 anti- T. cruzi antibodies showed a tendency to be associated with dilated cardiomyopathy.
Methods
Selection of Chronic Chagasic Patients
Patient population was composed of 12 adults with cardiomyopathy, aged 34 to 67 years, and in whom serological studies for anti T. cruzi antibodies were indicated under the judgement of their treating physicians. All patients came from rural areas in Mexico, three of them were from Oaxaca (Puerto Escondido, Pinotepa Nacional and Tecamaxtlahuaca) , two from Chiapas (Siquilhucum and Pijijiapan), two from Guerrero ( Cuajinicuilapan and Buena Vista), two from Veracruz (Colotlan and Chicoltepec), one from San Pedro Meyen Edo, Mexico, one from Nuevo Urecho Michoacán, one from Huehuetlan, Puebla, one from San Luis Potosí and one from Monterrey, Nuevo León who was infected in Cuernavaca, Morelos. All of them displayed positivity for serum anti T. cruzi antibodies. They had a complete clinical evaluation. Peripheral twelve lead EKG; thoracic roentgenogram with cardiac series; mode M, 2D, and color Doppler echocardiography; left ventriculogram, and coronariography were performed by routine techniques.
Dilated cardiomyopathy diagnosis was established based on the left ventricular end-systolic dimension (LVESD) and cardiothoracic ratio (CTr) on chest X-ray film. LVESD and CTr were between 28mm to 57 mm and 0.43 to 0.60, respectively. Ejection fraction (EF) ranged between 30% and 68% Table I.
Clinically healthy adult subjects
Sera from 30 consecutive healthy blood donors (aged 18 to 50 years) were used for comparison purposes. All of them disclosed anti-T.cruzi negative antibodies, no data of heart or transmissible diseases under routine physical exploration or anemnesis.
Sera samples
Venous blood samples were collected by standard antecubital venipuncture, and then centrifuged at 2,500 rpm for 10 min.; serum was recovered and frozen at -40 °C until studied.
Anti- Trypanosoma cruzi antibodies detection
Total IgG anti- T cruzi antibodies were detected by indirect immunofluorescence (IIF) and enzyme linked immunosorbent assay (ELISA) as described with minor modifications.11 In brief, IIF was performed on the epimastigote form of T. cruzi, fixed on a microscope slide. Human serum was diluted 1: 32 and a fluorescein conjugated goat anti -human IgG was used at 1: 100 dilution. Positive and negative controls were always included, and the slide was read under an epifluorescence microscope.
ELISA was done using polystyrene plates coated with 1 µg of a crude T. cruzi extract per well. Human serum was diluted at 1:400 and anti- human IgG- peroxidase conjugate was used at 1:5000. Incubation time was ten minutes for steps mentioned above. The reaction was revealed by the addition of O-phenilen-diamine and read at 490 nm in an automatic ELISA reader. A result was considered positive when its OD value was above the mean plus 5 SD of 30 seronegative healthy individuals.
Anti-Trypanosoma cruzi IgG subclasses
Identification of IgG subclasses within anti-T.cruzi antibodies was performed as previously described with minor modifications.12 A polystyrene plate was coated with 1 µg per well of a crude T. cruzi extract in an alkaline buffer (carbonate/bicarbonate 0.05M pH 9.6) for 1 hour at 37°C. The plates were then extensively washed and blocked with 1% bovine albumin phosphate buffered saline containing 0.05%Tween 20 (PBS-TA), for 15 minutes at 37°C. Human serum diluted 1:200 in PBS-TA was added and incubated for 1 hour at 37°C. After thorough washes, each plate was incubated for 1 hour at 37°C with sheep antibodies specific against every one of the four human IgG subclasses (Organon Teknika, West Chester PA, 19380) diluted 1:500 in PBS-TA. We used polyclonal rather than monoclonal antibodies, because the latter are less sensitive.13 Finally, after new thorough washes, horseradish peroxidase coupled rabbit antibodies against sheep immunoglobulin diluted 1:1000 in PBS-TA were added, and each plate was incubated for 1 hour at 37°C. Plates were developed and read at 490 nm in a microplate reader. Each sample was tested by triplicate. A pool of negative T. cruzi sera from healthy donors was used as negative control in all experiments.
Cut off value was set as follows: sera from 30 healthy seronegative individuals were individually tested for IgG subclasses as described before.12 The same pool of 30 healthy human sera was run as negative control in every assay. Mean OD ratios obtained for each IgG subclass between each individual negative serum sample and negative control were analyzed for their distribution in order to determine the cut off. The ratio was calculated by the following formula: OD ratio = (mean OD sample)/ (mean OD negative pool)
The OD ratios of each sample including seronegative healthy individuals were then averaged for analysis.
The mean OD ratio of seronegative healthy individuals plus 3SD was fixed to set the cut off. All normal healthy individuals had values classified as negative. Threshold ratios obtained were 2.5 for IgG1, 2.8 for IgG2, 3.5 for IgG3 and 1.3 for IgG4.
Statistical analysis
The descriptive section included mean and range. The inferential section was supported by the Mann-Whitney U test. Using GraphPad Prism*11 version 2.0. Adjustment for multiple comparisons was not applied.
Ethical issues
This work was submitted and approved by the ethics committee.
Results
Demographic and clinical features of patients are summarized in Table I. Mean age was 46 years and female: male ratio was 0.7. All cases came from rural areas and all of them had lived in endemic zones for over 7 years. The patients had CCC with variable degrees of heart enlargement, in seven cases LVESD were above 42 mm, indicative of chamber dilatation, and in five was normal. Ejection fraction was below 50% in seven cases, indicative of ventricular dysfunction.
Rhythm and conduction aberrations were present in all cases. Right bundle branch block and ventricular extrasystoles were the most common finding (data not shown). Neither the length of residence in known endemic zones nor the age or gender had influence on clinical manifestations. All patients displayed values above the respective cut-off point (mean of OD ratio of negative samples plus 3SD) for the four IgG subclasses of anti- Trypanosoma cruzi antibodies but the highest levels was observed for IgG1 and IgG2 in nearly all cases. There were moderately high levels of IgG3 anti- T.cruzi antibodies and consistently low levels of IgG4 anti- T.cruzi antibodies in all patients as shown in Table I.
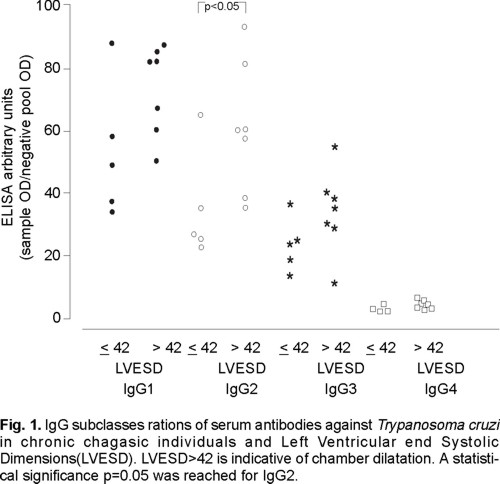
When we compared left ventricular-end systolic dimension values and IgG subclasses level of anti-T.cruzi antibodies, an statistically significant (p=0.05) tendency for an association between severe chamber dilation and high levels of IgG2 anti- T.cruzi antibodies was observed Fig. 1.
Discussion
Heart enlargement and abnormal ejection fraction was presented in 58% of the patients. Although, the group studied is relatively small, our data support the concept that high levels of total IgG anti-T.cruzi antibodies is a constant feature in CCC, even in those patients that had moved to non-endemic zones for over 32 years (table I). This highly specific immune response maintained over years, suggest a continuous antigenic stimulus and persistence of parasite as reported by different groups.14-16
It is known that in humans, IL-4 is able to induce switching from IgM to IgG1 or IgE or to produce IgG4 in the presence of a persistent antigen,17,18 indicative of Th2-like immune response. It is also known that IgG1 response is dominant particularly after a secondary stimulation;19 however, a preferential IgG2/IgG3 antibody profile is indicative of a Th1-like immune response.20,21 In this study, we found high level of IgG1, IgG2, and IgG3 ant-T.cruzi antibodies in chronic chagasic patients and low detectable level of IgG4 anti-T.cruzi antibodies, suggesting a mixed Th1/Th2-like immune response.
The recently published findings on cytokine patterns in chronic and indeterminate cases of American trypanosomiasis support our data. It has been reported that in the peripheral blood mono-nuclear cells of symptomatic and asymptomatic individuals a mixed pattern of INF-gamma and IL-4 coexist. A dominant Th1 (INF-y) response is showed in subjects from low endemicity regions, while a dominant Th2 (IL-4) was characteristic in subjects from high endemicity regions.22,23 We have found that low titers of IgG anti- T.cruzi do exist in the indeterminate cases 24 , while chronic Chagasic patients displayed a higher humoral immune response.15 In this study was no possible to include indeterminate cases for comparative purpose.
Many organ-specific forms of autoimmunity in experimental animal systems have Th1 features, with preferential IgG2/IgG3 antibody profile. In human non-chagasic cardiomyopathy, a Th1-like autoimmune disease characterized by IgG2/IgG3 anti-myosin response has also been shown.10 In the field of autoimmunity, accumulated evidence suggests that a Th1 profile may play a role in pathogenesis. It is noteworthy that there is also evidence that induction of self-antigen-specific Th2 cells can prevent autoimmune disease.25
In this context, our findings may suggest that continuous chronic parasite stimulation may take place, even in those infected cases that do not reside in endemic zones any more. Persistence of minute intracellular or circulating parasite can induce the four IgG subclasses of anti-T.cruzi antibodies in a mixed Th1(INF-y)/Th2(IL-4) -like immune response. Taking together all the data mentioned above, we could speculate that indeterminate cases may control better the parasite inoculation leading to mixed Th1/Th2 immune response with preferential Th1, whereas in susceptible individuals a chronic phase with chronic chagasic cardiomyopaty (CCC) is developed with Th1/Th2 mixed response and preferential Th2 inducing a high humoral immune response incluiding the four IgG subclasses anti-T,cruzi.
On the other hand, we observed a tendency for an association between high levels of IgG2 and cardiomegaly. Our studied group is small, and this observation should be confirmed in a larger study. The correlation between antibody levels and different clinical forms of chronic Chagas disease has been poorly studied. Morgan et al26 worked with the four clinical forms of T.cruzi infection founding no differences between the levels of IgG1 or IgG3 anti-T.cruzi and different clinical forms. However, if we analyze their data, the levels of IgG1 were strikingly high despite their use of mouse monoclonal antibodies to human IgG subclasses. But they were unable to show a good specific reactivity or even undetectable against T.cruzi antigen when determined IgG2 or IgG4 subclass anti-T.cruzi. respectively. It is known that well-characterized monoclonal anti-IgG subclass reagents vary in affinity and suitability.13 It could be possible that this condition may affected the results obtained.
Levin et al9 using a recombinant JL5 antigen of T.cruzi that represents COOH terminal portion of a T.cruzi ribosomal P protein (RP) and its synthetic peptide comprising the 13 C-terminal residues of P ribosomal protein (R-13) that shares 90% of homology to the ribosoma P protein epitope recognized in systemic lupus erythematosus, found a positive correlation of high anti-RP antibody levels of IgG1 subclass with severe CCC. However, Cerban et al7 did not find a clear association between anti-T cruzi IgG1 levels and the severity of the cardiomyopathy.
The differences observed between our data and in particular Cerban's data could be due to the antigen source it self. In our case a crude epimastigote extract was used, whereas they used formaldehyde-treated complete epimastigotes or FIV fraction antigen, obtained after centrifugation at 105,000g and electrophoresed under a pH gradient, using proteins separeted at pH 45. Formaldehide-treated epimastigotes may carry distinct altered epitopes, while purified antigens as FIV could call for a restricted antibody population and for binding to a selected number of epitopes.
In regard to Levin's data they identified a restricted IgG1 cross-reacting autoantibody response and severe cardiomegaly that could be induced under Th2 preferential immune response, whereas in our case IgG2 anti-Tcruzi antibodies could be induced under T.cruzi antigen driven and Th1 preferential immune response.
A very recently published paper by Cordeiro et al found IgG1 and IgG2 as the predominant main subclasses by conventional serology assay whereas IgG1 and IgG3 were the predominant ones in lytic antibodies assay. Reactivity of IgG2 antiepimastoges antibodies was greater in indeterminate and cardiac cases than in digestive. Furthermore, a high levels of IgG1 lytic antibodies was associated with the most of the indeterminate individuals.27
In summary, these our observations suggest a mixed Th1/Th2 immune response in human Chronic Chagasic Cardiopathy patients, as well as a possible association of chamber dilatation with high levels of IgG2 anti-T.cruzi antibodies.
Conclusions
Although a definitive study still is not available, there are several observations, including this work, which demonstrate a high specific humoral immune response in CCC patients. A mixed Th1/ Th2 response seems to be characteristic of chronic phase of AT, differences between cardiac and mega syndromes include specific IgG subclass response.
Acknowledgments: We wish to thank Dr Luis H. Silveira Torres for reviewing the manuscript.
Financial support: Conacyt grant 30944-M
References
1. Rassi A, Luquetti O, Rassi A, Rassi SG., Rassi AG: Chagas disease clinical features. In: Chagas' disease (American Trypanosomiasis): Its impact on transfusion and Clinical medicine. Is BT Brazil, 92, Sao Paulo Brazil.1992; 81-101. [ Links ]
2. Krettli A, Brener Z: Protective effects of specific antibodies in Trypanosoma cruzi associated to anti -living trypomastigotes antibodies. J Immunol 1976; 116: 755-760. [ Links ]
3. Norris K, Harth G, So M: Purification of a Trypanosoma cruzi membrane glycoprotein which elicits lytic antibodies. Inf Immun 1989; 87: 2372-2377. [ Links ]
4. Takehara HA, Perini A, Da Silva M, Mota I: Trypanosoma cruzi. Role of different antibody classes in protection against infection in the mouse. Exp Parasitol 1981; 52: 137-141. [ Links ]
5. Powell M, Wassom D: 1993. Host genetics and resistance to acute Trypanosoma cruzi infection in mice. I. Antibody isotype profiles. Parasite Immunol 1993; 15: 215-221 [ Links ]
6. Primavera K, Hoshino-Shimizu S, Umezawa E, Peres B, Manigot D, Camargo M: Immunoglobulin A antibodies to Trypanosoma cruzi antigens in digestive forms of Chagas' disease. J Clin Microbiol 1988; 26: 2101-2104. [ Links ]
7. Cerban F, Gea S., Menso E, Vottero-Cima E. Chagas' disease: IgG isotypes against Trypanosoma cruzi cytosol acidic antigens in patients with different degree of heart damage. Clin Immunol Immunopathol 1993; 67: 25-30. [ Links ]
8. Umezawa E, Shikanai-Yasuda M, Stolf M. Changes in isotype composition and antigen recognition of anti- Trypanosoma cruzi antibodies from acute to Chronic Chagas disease. Journ Clin Lab Analy 1996; 10: 407-413. [ Links ]
9. Levin MJ, Levitus G, Kerner N, Lafon S, Schijman A, Levy-Yeyatic P, et al: Autoantibodies in Chagas 'disease: possible markers of severe Chagas' heart complaint. Mem Inst Oswaldo Cruz 1990; 85: 539-543. [ Links ]
10. Skyllouriotis P, Skyllourioti-Lazarou M, Natter S, Steiner S, Spitzauer S, Kapiotis S, et al: IgG subclass reactivity to human cardiac myosin in cardiomyopathy patients is indicative of Th1–like autoimmune disease. Clin Expe Immunol 1999; 115: 236-247. [ Links ]
11. Ramos-Echevarría A, Monteón VM, Reyes PA: Detección de anticuerpos contra Trypanosoma cruzi en donadores de sangre. Sal Publ (Mex) 1993; 3556-64. [ Links ]
12. Vázquez-Abad D, Monteón V, J Senecal J, Walsh SN, Rothfield N: Analysis of IgG Subclasses of human topoisomerase I. Autoantibodies suggests Chronic B cell stimulation. Clin Immunol Immunopathol 1997; 84: 65-72. [ Links ]
13. Hamilton R: Human IgG measurements in the clinical laboratory. Clin Chem 1987; 33: 1707-1725. [ Links ]
14. Higuchi M, Britto T, Reiss M, Barbosa A, Belloti G, Pereira-Barreto A, Pileggi F: Correlation between Trypanosoma cruzi parasitism and myocardium inflammatory infiltrate in human Chronic Chagasic myocarditis: light microscopy and immunohistochemical findings. Cardiovasc Pathol 1993; 2: 101-106 [ Links ]
15. Monteón-Padilla VM, Hernández-Becerril N, Ballinas-Verdugo MA, Aranda Fraustro A, Reyes PA: Persistence ofTrypanosoma cruzi in chronic chagasic cardiopathy patients. Arch Med Res 2001; 32: 39-43 [ Links ]
16. Jones E, Colley D, Reis E, Vnencak-Colley C, McCurley T: Amplification of Trypanosoma cruzi DNA sequence from inflammatory lesions in human chagasic cardiomyopathy. Am J Trop Med Hyg 1993; 48: 348-357 [ Links ]
17. Callard R: Immunoregulation byinterleukin-4 in man. Br. Journ Haemathol 1991; 78: 293-299. [ Links ]
18. Lundren M, Persson V, Larsson P: Interleukin-4 induces synthesis of IgE and IgG4 in human B cells. Eur Journ Immunol 1989 19: 1311-1315. [ Links ]
19. Jefrris R: Selective IgG subclass deficiency: Quantification and clinical relevance. Clin Exp Immunol 1990; 81: 357-367. [ Links ]
20. German T, Bongartz M, Dlugonska H: Interleukin-12 profoundly up-regulate the synthesis of antigen-specific complement-fixing IgG2a, IgG2b and IgG3 antibody subclass in vivo. Eur Journ Immunol 1995; 25: 823-829. [ Links ]
21. Chrlton B, Lafferty KJ: The Th1/Th2 balance in autoimmunity. Curr Opin Immunol 1995; 7:793-798 [ Links ]
22. Samudio M, Montenegro-James S, de Cabral M, Martínez J, Rotas A et al: Differential expression of systemic cytokine profiles in Chagas 'disease is associated with endemicity of Trypanosoma cruzi infection. Acta Trop 1998; 69:89-97 [ Links ]
23. Dutra W, Gollob K, Pinto-Dias J, Gazzinelli G, Correa-Oliverira R et al: Cytokine mRNA profile of peripheral blood mononuclear cells isolated from individuals with Trypanosoma cruzi chronic infection. Scand Journ Immunol 1997;45:74-80. [ Links ]
24. Monteón-Padilla V, Hernández-Becerril N, Guzmán-Bracho C, Rosales-Encina JI, Reyes PA: American trypanosomiasis (Chagas'disease) and blood banking in México City: Seroprevalence and its potential transfusional transmission risk. Arch Med Res 1999; 30: 393-398. [ Links ]
25. Nicholson LB, Kuchroo VK: Manipulation of the Th1/TH2 balance in autoimmune disease. Autoimmunity 1996; 8: 837-842. [ Links ]
26. Morgan J, Pinto JC, Dias E, Bahia-Oliveira L, Correa-Oliveira R, Colley D, et al: Ani-Trypanosma cruzi antibody isotype profiles in patients with different clinical manifestations of Chagas' disease. Am J Trop Med Hyg 1996;55:355-359 [ Links ]
27. Cordeiro FD, Martins-Filho O, Da Costa MO, Adad SJ, Correa-Oliveira R, et al: Ani-Trypanosoma cruzi immunoglobulin G1 can be a useful tool for diagnosis and prognosis of human Chagas'disease. Clin Diagn Lab Immunol 2001;8:112-118. [ Links ]

