











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
According to the World Health Organization in 2019, suicide is a serious global public health issue. Globally, 703, 000 people die by suicide every year. Suicide is among the leading causes of death worldwide, with more deaths due to suicide than to malaria, HIV/AIDS, breast cancer, or war and homicide. More than one in every 100 deaths (1.3 per cent) in 2019 were the result of suicide. The global age-standardized suicide rate was 9.0 per 100,000 population for 2019. Rates varied between countries from fewer than two deaths by suicide per 100, 000 to over 80 per 100,000. The global age-standardized suicide rate was higher in males (12.6 per 100,000) than in females (5.4 per 100,000). While for females, the highest rates in countries were above 10 per 100,000, for males they were above 45 per 100,000. Globally, the age-standardized suicide rate was 2.3 times higher in males than in females. Male:female suicide ratios greater than 1 indicate that suicide rates are higher in males than in females. While the ratio was a little over 3 in high-income countries, it was lower in low-and middle-income countries (low-income countries: 2.9; lower-middle-income countries: 1.8; upper-middle-income countries: 2.6). Globally, the majority of deaths by suicide occurred in low-and-middle-income countries (77 per cent), where most of the world’s population live. More than half of global suicides (58 per cent) occurred before the age of 50 years. Most adolescents who died by suicide (88 per cent) were from low-and middle-income countries where nearly 90 per cent of the world’s adolescents live. Suicide was the fourth leading cause of death in young people aged 15-29 years for both sexes, after road injury, tuberculosis and interpersonal violence. For females and males, respectively, suicide was the third and fourth leading cause of death in this age group. Differences in age-standardized suicide rates can be seen across WHO regions. Suicide rates in the African (11.2 per 100,000), European (10.5 per 100,000) and South-East Asia (10.2 per 100,000) regions were higher than the global average (9.0 per 100,000) in 2019. The lowest suicide rate was in the Eastern Mediterranean region (6.4 per 100,000). The South-East Asia region had a much higher female age-standardized suicide rate (8.1 per 100,000) compared to the global female average (5.4 per 100,000). In males, the regions of Africa (18.0 per 100,000), the Americas (14.2 per 100,000) and Europe (17.1 per 100,000) all had suicide rates which were higher than the global male average (12.6 per 100,000) (World Health Organization, 2021).
In 2019, the ten countries with the highest suicide rates per 100,000 habitants were 1. Lesotho 72.4, 2. Guyana 40.3, 3. Eswatini 29.4, 4. South Korea 28.6, 5. Kiribati 28.3, 6. Federated States of Micronesia 28.2, 7. Lithuania 26.1, 8. Suriname 25.4, 9. Russia 25.1, and 10. South Africa 23.5 (Suicide Rate by Country, 2023).
There was an increase in age-adjusted suicide rates in Latin America and the Caribbean during the period from 1990 to 2009 (Mascayano et al., 2015). Suicide is an extremely important public health problem in Latin America; in the years 2005-2009, approximately 65,000 deaths from suicide each year have been identified and an age-adjusted mortality rate of 7.3 per 100,000 population. From the subregional perspective, the non-Hispanic Caribbean and North America experienced the highest rates of suicide in 2005-2009, while the lowest rates were seen in the subregions of South America and Central America, the Hispanic Caribbean and Mexico. The age-adjusted suicide rate for Latin America and the Caribbean was 5.2 per 100,000 population for both sexes. In the subregions of the Americas, the age-adjusted annual suicide rates per 100,000 population for both sexes were as follows: North America, 10.1; Central America, the Hispanic Caribbean and Mexico, 5.3; South America, 5.2; and the non-Hispanic Caribbean, 7.4 (Pan American Health Organization, 2014).
In Mexico, suicide is one of the most worrying problems since it has doubled since 1990 and the most increment is seen in adolescents and young adults. Although self-inflicted death is less frequent in women, it has increased by 95 per cent since 1990, while in men the increase has been 67 per cent (Programa Sectorial de Salud 2013-2018, 2014).
Suicide is unique among causes of death from illness by virtue of the fact that it is a behavioral endpoint. Its causes are complex and multifaceted and include underlying mental illness, stressful life events, and personality factors such as coping styles. It can occur at any point in the lifespan after early childhood (Sinyor, Tse and Pirkis, 2017).
Suicides are preventable. Even so, every 40 seconds a person dies by suicide somewhere in the world and many more attempt suicide. Suicides occur in all regions of the world and throughout the lifespan. Notably, among young people 15-29 years of age, suicide is the second leading cause of death globally. Suicide has an impact on the most vulnerable populations in the world and is highly prevalent in marginalized and discriminated groups of society. It is not just a serious public health problem in developed countries; In fact, most suicides occur in low-and middle-income countries where resources and services, if they do exist, are often scarce and limited for early identification, treatment and support of people in need. These striking facts and the lack of timely interventions make suicide a global public health problem that need to be tackled imperatively (World Health Organisation, 2014). Suicide increases in individuals without schooling or low schooling (Lakshmi, Yadaiah, Srinivas and Mounika, 2023).
In Mexico, there are no studies investigating trends in mortality by suicide in socioeconomic regions, neither the association of the level of schooling with suicide. The results of this study could be useful for actions aimed at the management of suicides in Mexico.
The objective of this study was to determine mortality trends from suicide at the national level, by state and socioeconomic region, as well as to determine the risk of suicide according to the level of schooling and socioeconomic region in the period from 2000 to 2020.
Methods
An ecological study design was used. Mortality records associated to Intentional self-harm for 2000-2020 were obtained from the National Institute of Statistics and Geography (National Institute of Statistics and Geography, 2017). This information is collected from death certificates issued nationwide. All individual records of mortality in which the basic cause of death was intentional self-harm in the period of 2000 to 2020 were included in the study. The codes of the International Classification of Diseases, 10th revision were identified (WHO, 1995). They corresponded to the basic cause of death from Intentional self-harm (X60.0-X84.9).
Raw and age-adjusted suicide rates nationwide per 100,000 inhabitants were obtained, taking the world population as the standard population (Inskip, Beral, Fraser and Haskey, 1983; National Cancer Institute, 2022). Age-adjusted mortality rates per 100,000 inhabitants from each state and from each of the 7 socioeconomic regions (Table 1) established by the National Institute of Statistics and Geography were also obtained (National Institute of Statistics and Geography, 2000). The national population, estimated by the National Population Council for 2015-2030, was used for the rate adjustment (National Population Council, 2019). The relative risk (RR) and 95 per cent confidence interval (CI) were obtained by Poisson regression to determine the strength of association between educational attainment and socioeconomic regions with the suicide.
Table 1 Socioeconomic Regions of Mexico
| Socioeconomic Regions | States |
|---|---|
| 1 | Chiapas, Guerrero, Oaxaca |
| 2 | Campeche, Hidalgo, Puebla, San Luis Potosi, Tabasco, Veracruz |
| 3 | Durango, Guanajuato, Michoacan, Tlaxcala, Zacatecas |
| 4 | Colima, State of Mexico, Morelos, Nayarit, Querétaro, Quintana Roo, Sinaloa, Yucatan |
| 5 | Baja California, Baja California Sur, Chihuahua, Sonora, Tamaulipas |
| 6 | Aguascalientes, Coahuila, Jalisco, Nuevo Leon |
| 7 | Mexico City |
Source: National Institute of Statistics and Geography.
The seven socioeconomic regional categories for Mexico have been defined by the National Institute of Statistics and Geography of in which differences observed in the social and economic conditions of the population throughout México are presented according to the XII General Population and Housing Census. The seven socioeconomic regions comprise the 31 states and Mexico City according to indicators related to well-being such as education, occupation, health, housing and employment. States classified in the same region have similar characteristics on average; that is, they are homogenous, while the regions differ from one another. According to the indicators used, the socioeconomic conditions increase from region 1, least favorable, to region 7 most favorable. The methodology used to establish the regions had the objective of forming strata with minimal variance in an effort to group the elements more alike or closer to each other following a criterion of established similarity, which allows for differentiating one region from another. Among the techniques used are Mahalonobis distances and a combination of factorial analysis and the algorithm of the k-means (National Institute of Statistics and Geography, 2000).
The Poisson regression model was chosen to determine the strength of association between educational level and socioeconomic region with the suicide, because as a dependent variable, the number of suicides has a Poisson distribution that takes positive whole values. Poisson regression is equivalent to a logarithmic regression of mortality rates. The exponential coefficients allow for estimation of the RR of dying (Cameron and Trivedi, 1998).
Registrations were handled by the Access 2013 program. The strength of association between educational level and socioeconomic region with the suicide was obtained by Poisson regression through the Number Cruncher Statistical System program 2001 (Hintze, 2001). The Epidat version 3.1 program was used to determine age-adjusted mortality rates by state, and socioeconomic region (Hervada Vidal et al., 2004)
Results
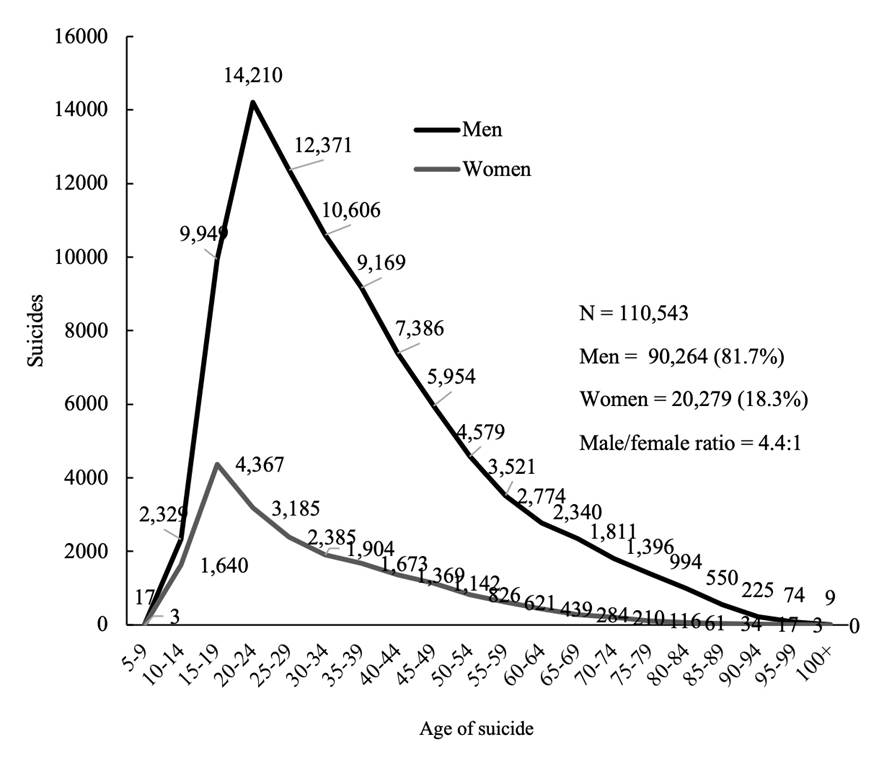
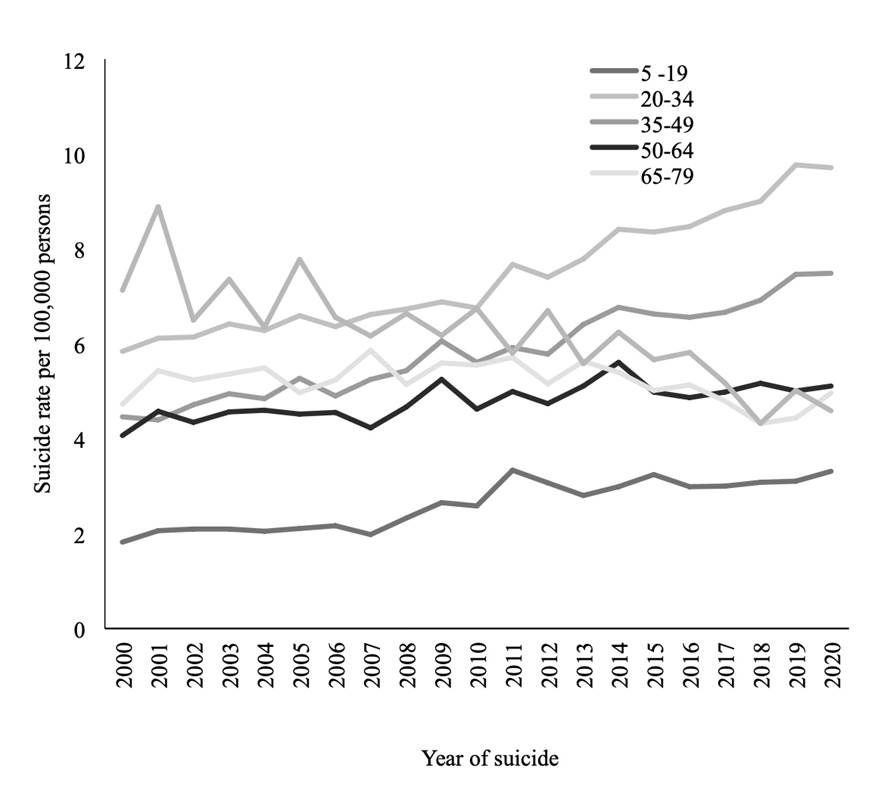
In the study period in Mexico the age-standardized suicide rate increased from 3.7 to 5.7 per 100,000 individuals (Percent change of 35 per cent) (Figure 1). In Mexico in the years 2000 to 2020 there were 110,543 suicides, men with 90,264 (81.7 per cent), and women with 20,279 (18.3 per cent), for a male/female ratio of 4.4:1. The age groups had the highest number of suicides were in the 20-24 years with a total of 17,395 suicides (14,210 [12.9 per cent] men and 3,185 [2.9 per cent] women); followed by age group 25-29 years with a total of 14,756 (12,371 [11.2 per cent] men and 2,385 [2.2 per cent] women), (Figure 2). In the years, 2000 and 2020 there were 3,484 and 7,323 suicides, respectively. In the six age groups, mortality trends increased, except in the age group ≥ 80 years in which the suicide rate decreased from 7.1 to 4.6. The age group 20-34 years had the higher increased of suicide rate from 5.8 to 9.7 (Figure 3).
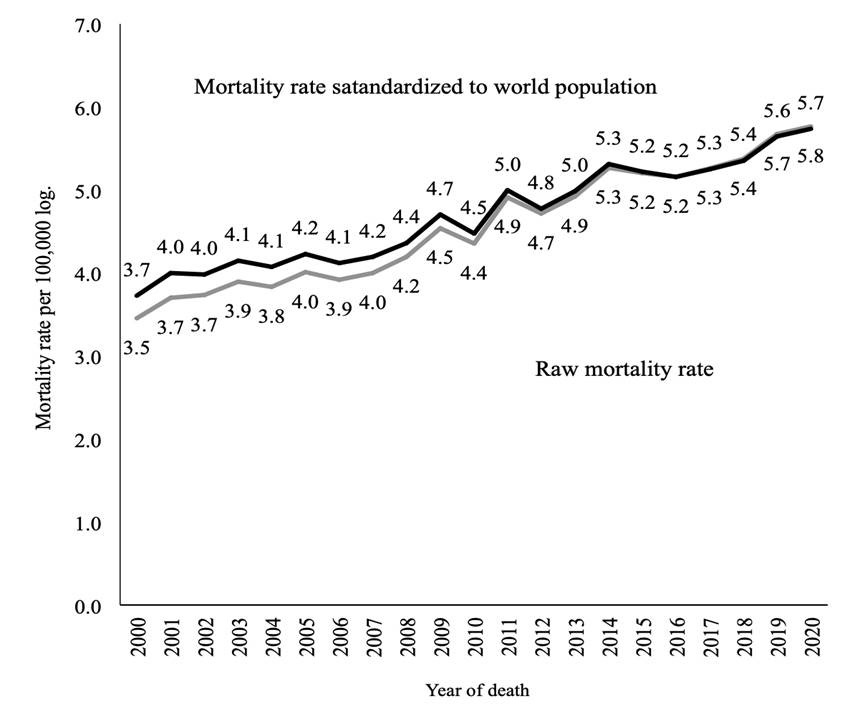
Note: Raw rate of mortality per 100,000 individuals.
Age-adjusted rate by the direct method, standardized with world population per 100,000 individuals.
Source: Analysis by the author of data obtained from the National Institute of Statistics and Geography for the years 2000-2020, and from the National Population Council: population estimates, period 1990-2010 and population projections for the horizon 2015-2030.
Figure 1 Suicide trends. Mexico, 2000-2020
Source: Analysis by the author of the database obtained from the National Institute of Statistics and Geography for the years 2000-2020.
Figure 2 Suicides by age group and gender. Mexico, 2000-2020
Source: Analysis by the author of data obtained from the National Institute of Statistics and Geography for the years 2000-2020, and from the National Population Council: population estimates, period 1990-2010 and population projections for 2015-2030.
Figure 3 Suicide trends by age group. Mexico, 2000-2020
The five main causes of suicide were: 1). Intentional self-harm by hanging, strangulation and suffocation (X70), with 84,876 (76.78 per cent) (Men 70,807 [64 per cent], women 14,069 [12.73 per cent]; 2). Intentional self-harm by other and unspecified firearms discharge (X74), with 11,690 (10.58 per cent) (Men 10,612 [9.60 per cent], women 1,078 [0.98 per cent]); 3) Intentional self-poisoning by and exposure to pesticides (X68), with 4,194 (3.79 per cent) (Men 2,529 [2.29 per cent], women 1,665 [1.51 per cent]; 4) Intentional self-poisoning by and exposure to other and unspecified chemicals (X69), with 3,202 (2.90 per cent) (Men 1,773 [1.60 per cent], women 1,429 [1.29 per cent]); 5) Intentional self-harm by other no specified means (X84), with 1,274 (1.15 per cent) (Men 935 [0.85 per cent], women 339 [0.31 per cent]) (Table 2).
Table 2 Suicide by cause. México, 2000-2020
| ICD 10 | Intentional self-harm | Men 90,264 (81.66%) |
Women 20,279 (18.34%) |
|---|---|---|---|
| X60 | Intentional self-poisoning by and exposure to nonopioid analgesics, antipyretics and antirheumatics | 13 (0.01%) | 21(81.66%) |
| X61 | Intentional self-poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified | 114 (0.10%) | 163 (0.15%) |
| X62 | Intentional self-poisoning by and exposure to narcotics and psychodysleptics [hallucinogens], not elsewhere classified | 33 (0.03%) | 15 (0.01%) |
| X63 | Intentional self-poisoning by and exposure to other drugs acting on the autonomic nervous system | 7 (0.01%) | 12 (0.01%) |
| X64 | Intentional self-poisoning by and exposure to other and unspecified drugs, medicaments and biological substances | 455 (0.41%) | 753 (0.68%) |
| X65 | Intentional self-poisoning by and exposure to alcohol | 24 (0.02%) | 5 (0.005%) |
| X66 | Intentional self-poisoning by and exposure to organic solvents and halogenated hydrocarbons and their vapours | 39 (0.04%) | 11 (0.01%) |
| X67 | Intentional self-poisoning by and exposure to other gases and vapours | 172 (0.16%) | 39 (0.04%) |
| X68 | Intentional self-poisoning by and exposure to pesticides | 2,529 (2.29%) | 1,665 (1.51%) |
| X69 | Intentional self-poisoning by and exposure to other and unspecified chemicals and noxious substances | 1,773 (1.60%) | 1,429 (1.29%) |
| X70 | Intentional self-harm by hanging, strangulation and suffocation | 70,807 (64.05%) | 14,069 (12.73%) |
| X71 | Intentional self-harm by drowning and submersion | 258 (0.23%) | 111 (0.10%) |
| X72 | Intentional self-harm by handgun discharge | 142 (0.13%) | 23 (0.02%) |
| X73 | Intentional self-harm by rifle, shotgun and larger firearm discharge | 294 (0.27%) | 20 (0.02%) |
| X74 | Intentional self-harm by other and unspecified firearm discharge | 10,612 (9.60%) | 1,078 (0.98%) |
| X75 | Intentional self-harm by explosive material | 8 (0.01%) | 0 (0.00%) |
| X76 | Intentional self-harm by smoke, fire and flames | 128 (0.12%) | 50 (0.05%) |
| X77 | Intentional self-harm by steam, hot vapours and hot objects | 4 (0.004%) | 0 (0.00%) |
| X78 | Intentional self-harm by sharp object | 1,112 (1.01%) | 153 (0.14%) |
| X79 | Intentional self-harm by blunt object | 10 (0.01%) | 1 (0.001%) |
| X80 | Intentional self-harm by jumping from a high place | 543 (0.49%) | 225 (0.20%) |
| X81 | Intentional self-harm by jumping or lying before moving object | 141 (0.13%) | 61 (0.06%) |
| X82 | Intentional self-harm by crashing of motor vehicle | 63 (0.06%) | 24 (0.02%) |
| X83 | Intentional self-harm by other specified means | 48 (0.04%) | 12 (0.01%) |
| X84 | Intentional self-harm by other no specified means | 935 (0.85%) | 339 (0.31%) |
Source: Analysis by the author of the data obtained from the National Institute of Statistics and Geography for the years 2000-2020.
Individuals with complete elementary school and high school not finished had higher risk of suicide (RR 3.84, CI95% 3.75-3.93), while those with complete senior in high school had lower risk of suicide (RR 1.42, CI95% 1.38 -1.46) (Table 3).
Table 3 Relative risk of dying from suicides according to educational level, and 95% confidence interval according to Poisson regression. Mexico, 2000-2020
| Education | Relative Risk | 95% confidence Interval |
|---|---|---|
| No school or incomplete elementary school | 2.57 | 2.51-2.64 |
| Complete elementary school and high school not finished | 3.84 | 3.75-3.93 |
| Complete high school and senior in high school not finished | 3.56 | 3.47-3.65 |
| Complete senior in high school | 1.42 | 1.38-1.46 |
| College and postgraduate studies | 1 | N.A |
Note: N/A: Not applicable.
Source: Analysis by the author of the data obtained from the National Institute of Statistics and Geography for the years 2000-2020.
The states with the highest suicide rate were Campeche (2000-2002, 2004, 2014), Yucatán (2003, 2010-2011, 2018), Tabasco (2005-2006), Quinta Roo (2007-2009, 2012), Aguascalientes (2013, 2019) and Chihuahua (2015-2017, 2020). Campeche in the year 2000 and 2014 had a rate of 8.8 and 10.8; Yucatan in 2003 and 2018 with 8.8 and 10.7; Tabasco in 2005 and 2006 with 8.9 and 8.5; Quintana Roo in 2007 and 2012 with 14.6 and 9.7; Aguascalientes in 2013 and 2019 with 9.2 and 12.1, and Chihuahua in 2015 and 2020 with 11.2 and 13.9 (Figure 4).
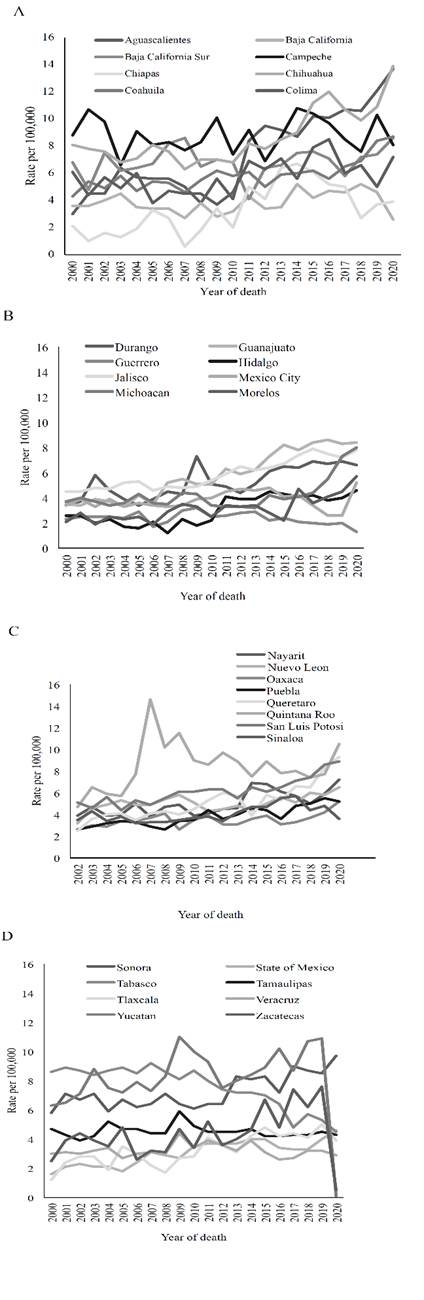
Note: Rate per 100,000 inhabitants adjusted by direct method using national population as standard population.
Source: Analysis by the author of the data obtained from the National Institute of Statistics and Geography for the years 2000-2020.
Figure 4 Age-adjusted suicide rate by state of residence. México, 2000-2020
The states with the lowest suicide rate were Tlaxcala (2000 and 2008), Chiapas (2001-2003, 2007, 2010), Hidalgo (2004-2005, 2009), Guerrero (2006, 2011-2014, 2016-2019), Morelos (2015) and Yucatan (2020). Tlaxcala in 2000 and 2008 had a suicide rate of 1.2 and 1.7; in Chiapas in 2001 and 2010 with a rate 1 and 2; Hidalgo in 2004 and 2009 with1.7 and 1.8; Guerrero in 2006 and 2019 with1.7 and 2, Morelos in 2015 with 2.2 and Yucatan in 2020 with 0.1 (Figure 4).
In the study period, region 5 had the highest suicide rate, except in 2012, 2018 and 2020; in these years region 6 had the highest mortality rate due to suicides. Region 5 in the year 2000 and 2020 had a suicide rate of 5.7 and 7.5 and in region 6 in 2012 and 2020 was 5.9 and 7.9. In the year 2017 region 5 and 6, had the highest mortality rate (7) (Figure 5).
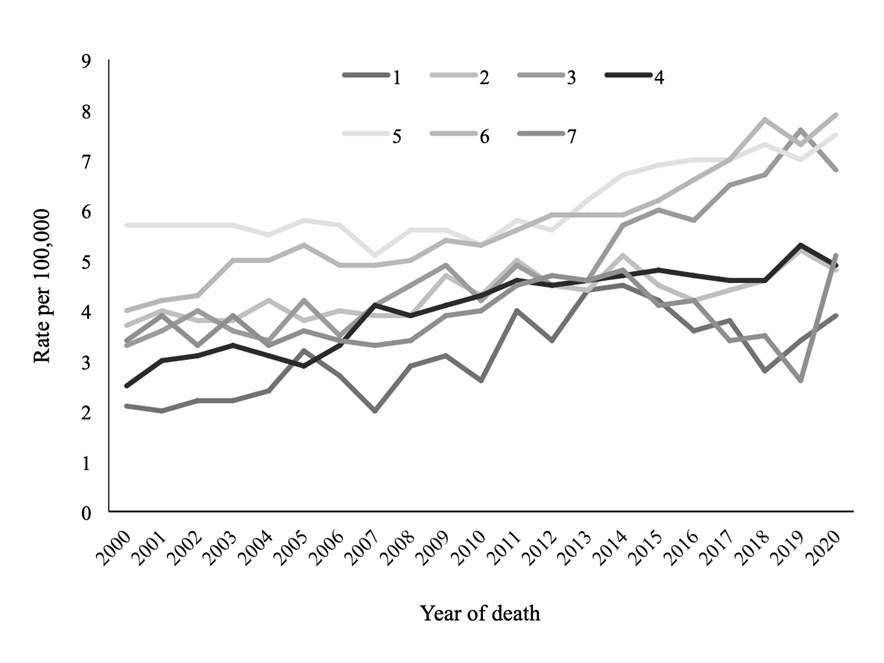
Note: Rate per 100,000 inhabitants adjusted by direct method using national population as standard population.
Source: Analysis by the author of data obtained from the National Institute of Statistics and Geography for the years 2000-2020, and from the National Population Council: population estimates, period 1990-2010 and population projections for 2015-2030.
Figure 5 Age-adjusted suicide rate by socioeconomic region. México, 2000-2020
Region 1 presented the lowest suicide rate, except in the years 2005, 2015, 2017 and 2019, in these years; regions had the lowest rate were region 4 (2005) and 7 (2015, 2017, 2019). Region 1 in the year 2000 and 2019 the suicide rates were of 2.1 and 3.4, and for region 4 in the year 2005 was 2.9 and for the region 7 in the year 2015, 2017 and 2019 was 4.1, 3.4 and 2.6 (Figure 5).
In the years 2000-2020, region 5 had the highest risk of dying from suicide, except in 2012, 2018-2020, in which region 6 had the highest risk. In region 5 in the year 2000 and 2017 the risk of suicide was 2.8, 95%CI 2.4-3.3 and 1.9, 95%CI 1.7-2.1, respectively; in region 6 in 2012 and 2020, the risk of suicide was 1.8, 95%CI 1.6-2 and 2.1 95%CI 1.9-2.3, (Table 4).
Table 4 Relative risk of dying from suicides by socioeconomic region and 95% confidence interval, according to Poisson Regression. Mexico, 2000-2020
| Regions | 2000 | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | Regions | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 1.8 (1.5─2.1) |
2.1 (1.8─2.5) |
1.8 (1.6─2.1) |
1.8 (1.6─2.1) |
1.8 (1.6─2.1) |
1.2 (1.1─1.4) |
1.6 (1.4─1.8) |
2 (1.7─2.3) |
1.4 (1.2─1.6) |
1.6 (1.4─1.8) |
2 | 1.7 (1.5─1.9) |
1.3 (1.2─1.4) |
1.4 (1.2─1.5) |
1 (0.9─1.2) |
1.2 (1.1─1.3) |
1.1 (1─1.2) |
1.2 (1─1.3) |
1.2 (1.1─1.3) |
1.7 (1.5─1.9) |
1.5 (1.4─1.7) |
1.3 (1.1─1.4) |
| 3 | 1.6 (1.3─1.9) |
1.9 (1.6─2.3) |
1.9 (1.6─2.2) |
1.7 (1.5─2) |
1.4 (1.2─1.7) |
1.3 (1.2─1.5) |
1.3 (1.2─1.6) |
2.1 (1.8─2.5) |
1.6 (1.4─1.8) |
1.6 (1.4─1.8) |
3 | 1.7 (1.5─1.9) |
1.3 (1.1─1.4) |
1.3 (1.2─1.5) |
1.1 (1─1.2) |
1.3 (1.2─1.4) |
1.5 (1.3─1.6) |
1.6 (1.4─1.8) |
1.7 (1.6─1.9) |
2.5 (2.2─2.8) |
2.2 (2─2.5) |
1.8 (1.6─2) |
| 4 | 1.3 (1.1─1.5) |
1.6 (1.4─1.9) |
1.5 (1.3─1.7) |
1.6 (1.4─1.9) |
1.4 (1.2─1.6) |
1 (0.9─1.1) |
1.3 (1.2─1.5) |
2.2 (1.9─2.5) |
1.4 (1.3─1.6) |
1.4 (1.2─1.6) |
4 | 1.7 (1.5─2) |
1.2 (1.1─1.3) |
1.4 (1.2─1.5) |
1.1 (1─1.2) |
1.1 (1─1.2) |
1.2 (1.1─1.3) |
1.3 (1.2─1.5) |
1.2 (1.1─1.4) |
1.7 (1.5─1.9) |
1.6 (1.4─1.8) |
1.3 (1.2─1.4) |
| 5 | 2.8 (2.4─3.3) |
3.1 (2.7─3.6) |
2.8 (2.4─3.2) |
2.8 (2.4─3.2) |
2.4 (2.1─2.8) |
1.9 (1.7─2.2) |
2.2 (2─2.6) |
2.7 (2.3─3.1) |
2.1 (1.8─2.3) |
1.9 (1.7─2.2) |
5 | 2.1 (1.9─2.4) |
1.5 (1.4─1.7) |
1.7 (1.5─1.9) |
1.5 (1.3─1.7) |
1.6 (1.4─1.7) |
1.7 (1.5─1.9) |
2 (1.8─2.2) |
1.9 (1.7─2.1) |
2.7 (2.4─3.1) |
2.1 (1.9─2.3) |
2 (1.8─2.2) |
| 6 | 2 (1.7─2.3) | 2.3 (2─2.7) |
2.1 (1.8─2.4) |
2.4 (2.1─2.8) |
2.2 (1.9─2.6) |
1.8 (1.6─2) |
1.9 (1.7─2.2) |
2.6 (2.2─3) |
1.8 (1.6─2.1) |
1.8 (1.6─2.1) |
6 | 2.1 (1.9─2.4) |
1.5 (1.3─1.6) |
1.8 (1.6─2) |
1.4 (1.3─1.6) |
1.4 (1.2─1.5) |
1.5 (1.4─1.7) |
1.9 (1.7─2.1) |
1.9 (1.7─2.1) |
2.9 (2.6─3.3) |
2.2 (2─2.4) |
2.1 (1.9─2.3) |
| 7 | 1.8 (1.5─2.1) |
2.3 (1.9─2.7) |
1.7 (1.4─2) |
2 (1.7─2.4) |
1.6 (1.3─1.8) |
1.3 (1.1─1.5) |
1.4 (1.2─1.7) |
1.9 (1.6─2.2) |
1.3 (1.1─1.5) |
1.4 (1.2─1.6) |
7 | 1.7 (1.5─2) |
1.2 (1─1.4) |
1.5 (1.3─1.7) |
1.1 (1─1.3) |
1.1 (1─1.3) |
1 (0.9─1.2) |
1.2 (1─1.4) |
0.9 (0.8─1.1) |
1.3 (1.1─1.5) |
0.8 (0.7─0.9) |
1.4 (1.2─1.5) |
Source: Analysis by the author of the data obtained from the National Institute of Statistics and Geography for the years 2000-2020, and from the National Population Council: population estimates, period 1990-2010 and population projections for 2015-2030.
Regions 4 (years 2000-2006, 2012-2014); 7 (2007-2011, 2015-2019); 3 (2012); and 2 (2012 y 2010) had a lower risk of dying from suicides. Region 4 in the year 2000 and 2014 the RR of suicide was 1.3, 95%CI 1.1-1.5 and 1.1, 95%CI 1-1.2 and for region 7 in 2007 and 2019 were 1.9, 95%CI 1.6-2.2 and 0.8, 95%CI 0.7-0.9; for region 3 in 2012 was 1.3, 95%CI 1.2-1.5; and region 2 in 2012 and 2020 were 1.4, 95%CI 1.2-1.5 and 1.3, 95%CI 1.1-1.4 (Table 4).
Discussion
In Mexico, in the period from 2000 to 2020, age-standardized suicide rate increased from 3.7 to 5.7 per 100,000 individuals (percentage of change 35 per cent) (Figure 2). These results are in line with suicide trends worldwide. In the last 45 years, the suicide rate has increased by 60 per cent worldwide (Mascayano et al., 2015).
A wide spectrum of risk factors for suicide has been recognized. Risk factors are characteristics making it more likely that a person will think about suicide or participate in suicidal behavior. The WHO Report on Suicide Prevention has established a bioecological model to organize risk factors in five categories: a) Health system, b) Society, c) Community, d) Relationships, and e) Individual (Mascayano et al., 2015; WHO, 2014).
The factors that could be associated to the increase of suicide in Mexico are a) Health System, b) Society, c) Community and e) Individual. The scarcity of economic resources of the Health System (Mascayano et al., 2015) could be one of the factors associated with the increase of suicides in Mexico. In the country, of the total budget allocated to health, only 2 per cent is allocated to mental health (a figure much lower than that recommended by the WHO) of this amount, 80 per cent is destined to the maintenance of psychiatric hospitals. Consequently, health actions focused on community are very limited. Access to psychiatric hospitals is restricted by geographical barriers since most of these hospitals are located in large cities. These data indicate that mental illnesses are not included in the general health system, which limits comprehensive and multidisciplinary care of patients (Programa Sectorial de Salud 2013-2018., 2014; Programa de Acción Especifico, 2022).
The communities in which people live have an important association with mental health. One of the most important social factors related to suicide is violence and trauma. These conditions can increase emotional stress and can be the psychopathological basis of depression and suicidal behavior in people who are already genetically predisposed (Mascayano et al., 2015). In Mexico, violence and trauma could be other factors related to the increase of suicides. Mexico has the highest homicide rates in the world. The increase in homicide rates in Mexico during the period 2007-2014 has had a dramatic impact on the health status of the population (Canudas, Aburto, García and Beltrán, 2016). The National Survey of Victimization and Perception of Public Safety 2022, shows that in Mexico there is a very high rate of criminal prevalence in the last 10 years, in 2012 there was a rate of 27,337 crimes per 100,000 inhabitants and in the year 2021, was 24,207 (Encuesta Nacional de Victimización y Percepción sobre Seguridad Pública, 2022).
Another factor that could be related to the increase in suicide in Mexico is mental illness. It is known that the risk factors at the individual level for suicide include mainly mental health disorders such as depression, bipolar disorder, schizophrenia and drug and alcohol abuse (Dragisic, Dickov, Dickov and Mijatovic, 2015; Mascayano et al., 2015). Which have increased in Mexico. In the 2005-2013 period the cases of schizophrenia increased from 7,016 to 7,049 (0.47 per cent increase), and the depression increased from 4,556 cases to 7,421 (62.8 per cent increase) (Arredondo, Díaz, Cabello, Arredondo and Recaman, 2018). In relation to bipolar disorder, there is no recent epidemiological information. Regarding drug and alcohol abuse; the prevalence of the use of any drug increased in Mexico from 7.8 per cent in 2011 to 10.3 per cent in 2016. The prevalence of illegal drug use increased from 7.2 per cent to 9.9 per cent, between 2011 and 2016 (Villatoro et al., 2017a). Regarding the consumption of alcohol in the general population, the last addiction survey showed a significant increase in prevalence between 2002 and 2016 (64.9 per cent to 71 per cent) (Villatoro et al., 2017b).
In this study was seen that men committed suicide more frequently than women (male/female ratio of 4.4:1) (Figure 2). Similar results have been observed in other studies. Mascayano et al. in his review of suicides in Latin America, he mentions a male/female ratio of 4:1 (Mascayano et al., 2015) Some of the factors that could be associated with men committing suicide more frequently than women could be their vulnerability, which is reflected in their lack of will to obtain help when they are depressed, anxious or distressed (Sher, 2018). The crisis of masculinity could also be another factor related to the increase in suicides, especially of young men, since this crisis of masculinity results in men considering suicide as a way out to the social challenges they face (Canetto and Cleary, 2012).
In this study, the group of 20 to 34 years of age had the highest suicide rate (Figure 3). Suicide is among the three leading causes of death worldwide among people aged 20 to 34 years (World Health Organization, 2016). In Mexico, suicide rates have increased steadily, this is particularly worrisome among the young population, increasing rapidly in the 15-29 age group (Orozco et al., 2018). Suicide is a major public health issue and a leading cause of death among children and young people worldwide. Risk factors related to youth suicidal behavior could be categorized into several domains including social and educational disadvantage, childhood and family adversity, psychopathology, individual and personal vulnerabilities, exposure to stressful life events and social, and cultural and contextual factors. There is strong evidence linking adverse childhood experiences to an increased risk of suicidal behaviours in adults. Ashworth et al. (2023) found a significant association between suicidal crisis and several adverse childhood experiences. Specifically, evidence of clusters of adverse childhood experiences variables suggests two distinct groups of children and young people associated with experiencing a suicidal crisis: those experiencing “household risk” and those experiencing “parental risk” (Ashworth et al., 2023).
The main causes of suicide in Mexico in the years 2000-2020, were intentional self-harm by hanging, strangulation and suffocation (76.78 per cent), Intentional self-harm by other and unspecified firearms discharge (10.58 per cent), Intentional self-poisoning by and exposure to, pesticides (3.79 per cent), Intentional self-poisoning by and exposure to other and unspecified chemicals and noxious substances (2.90 per cent) and Intentional self-harm by other no specified means (1.15 per cent) (Table 2). These suicide methods correspond to those used in Latin American countries. The main methods used were suffocation (59.2 per cent), poisoning (17.7 per cent) and firearms (13.8 per cent), though they vary across countries and regions. The most widely used methods of suicide in the non-Hispanic Caribbean is poisoning (47.3 per cent), and in South America the use of firearms for suicide is almost as frequent as poisoning (15.6 per cent and 16.1 per cent, respectively) (Mascayano et al., 2015). The method chosen for suicide also varies with age. In general, the preference for suffocation declines with age, while the preference of firearms increases. A study in Bolivia revealed pesticides to be the most frequent method for suicide attempts. The results also suggested that younger individuals used more unplanned methods in comparison to older individuals (Jaen, Ribeiro, Whitfield and Mari, 2014).
Individuals with complete elementary school and high school not finished had a higher risk of suicide (RR 3.84, CI95 per cent 3.75-3.93). In other studies, similar results have been seen. Lorant et al. (2018) in their study of socioeconomic inequalities in suicide in Europe found that in 1990, people with the lowest level of education had 1.82 times more suicides than those in the group with the highest education, in the year 2000, this ratio rose to 2.12 (Lorant et al., 2018). In another study conducted by the same author in Europe, he found Across all age groups, the risk of suicide among those with the lowest level of education, compared to the most highly educated, was 1.61 (95% CI:1.53-1.70) at baseline and decreased to 1.46 (95% CI:1.38-1.55) ten years later, a decrease which was statistically significant. Education is a time-invariant marker of socioeconomic status. The higher risk of suicide in less educated individuals may be due to early-life factors reducing educational opportunities and increasing mental health vulnerabilities (Lorant, Kapadia, Perelman and Group, 2021). Phillips and Hempstead (2017) in a study that had the aim to document the association between education and suicide risk, in light of rising suicide rates and socioeconomic differentials in mortality in the U.S, concluded that the study findings offer insight into the important connection between education and suicide, during a period when levels of suicide and economic inequality have been rising. The differences in circumstances surrounding suicide deaths by education level highlight the greater volatility and fragility in the daily lives of those experiencing socioeconomic disadvantage (Phillips and Hempstead, 2017). In Mexico, people with low or no education are usually found in marginalized populations, in social, geographic and economic aspects (López, 2006), these factors could limit the comprehensive and multidisciplinary care of patients who have risk factors for suicide (Programa Sectorial de Salud 2013-2018., 2014).
In the study period, in the region 5, individuals had higher mortality rates and risk of suicide (Figure 5 and Table 4). Region 5 is formed by Baja California, Baja California Sur, Chihuahua, Sonora and Tamaulipas. One of the possible causes of which the region 5 has greater risk of suicide, could be due to the greater consumption of drugs in this region (Dragisic et al., 2015). According to the National Survey of Drugs, Alcohol and Tobacco 2016-2017, these states were among the 10 leading consumers of legal and illegal drugs in Mexico in 2008, except for Sonora that ranked 17 out of 32 states in Mexico. In 2016, these states were among the first ten consumers of cocaine, except Sonora and Tamaulipas, which ranked 14th and 15th of the 32 states of Mexico (Villatoro et al., 2017). Although region 5 is among the regions with the highest socioeconomic level, drug users are individuals who are mostly in a low economic stratum, since they do not have basic health services or are insufficient, the income level is low, have food poverty, capacity poverty and patrimony poverty, have little or no schooling, also live in northern border states, which are located among the 10 states with the highest risk for drug use in Mexico, where there is still a high consumption of heroin and methamphetamine (García Aurrecoechea, Rodríguez, Córdova and Fernández, 2016).
Suicide is a serious phenomenon of Public Health, most suicides can be prevented. It is estimated that in 75 per cent of suicides there is the presence of one or more mental and behavioral disorders, which results from a complex interaction of biological, genetic, psychological, sociological, cultural and environmental factors. No discipline or level of social organization can by itself be responsible for the phenomenon of suicide or its prevention. In México, networks are being established for the prevention of suicide with the participation of public institutions, non-governmental organizations, organized civil society, volunteer groups, religious associations and other types of aid organizations. For this reason, a multisectoral program aimed to the prevention of suicide is developed, which integrates measures of general prevention (such as better living conditions) and indirect prevention (through the treatment of physical and mental illnesses), and identifies the cases at risk through specific programs in schools and in the community and the offer of training to health personnel in the identification of cases, proper management and an adequate channeling of patients with mental disorders (Programa Sectorial de salud 2013-2018., 2014).
One of limitations of this study was that the suicide rate, and strength of association between educational level and mortality from suicide could be even greater, since in Mexico there is an underreporting of mortality, in the period 2001-2003, it was 9.7 per cent.
However, Mexico is considered by the Pan American Health Organization as a country where the underreporting of mortality is low (Pan American Health Organization, 2006).
Conclusions
Age-adjusted suicide rates per 100,000 inhabitants increased from 3.7 to 5.1 between 2000 and 2020, taking the world population age distribution as standard. Individuals with complete elementary school and high school not finished had the highest suicide rates. Socioeconomic region 5 and 6 had the highest mortality rates and risk of suicide.

