











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
November 17, 2019, was the date of the first case of infection by SARS-CoV-2 (COVID-19). Patient zero was a 55-year-old male living in Hubei province, but it was not until December 27 that Zhang Jixian, a doctor at the local Provincial Hospital for Integrated Chinese and Western Medicine, warned health authorities about the new disease. On January 7, 2020, at the Chinese Center for Disease Control and Prevention (CCDC), the causative agent of this pneumonia of unknown etiology was identified as a coronavirus associated with acute respiratory syndrome. It was named SARS-CoV-2 due to its similarity to the SARS-CoV, which was discovered in 20031,2.
In Mexico, the first case of COVID-19 was detected on February 27, 2020. The number of cases increased rapidly throughout the world, following an exponential growth pattern that led the World Health Organization (WHO) to declare a pandemic on March 11, 20203,4.
During the following year, the spread of the infection and the intensive use of resources to fight it led to changes in health systems throughout the world5,6.
In the attempt to provide health services to the greatest number of patients infected by SARS-CoV-2, hospital institutions adapted by changing their logistical infrastructure, which led to a reduction or temporary suspension of surgical activity7,8.
As a result, the number of patients awaiting a surgical procedure has tended to increase in a context of an economic and health crisis that limits the ability of hospital institutions to provide the services usually demanded from them7.
Different strategies have been used to try to address this mismatch between supply and demand of health services, all of them without success. We consider that their failure was due to inadequate management, lack of inclusion criteria based on scientific evidence and lack of efficiency criteria for the use of resources. During a pandemic such as this, it is of utmost importance to implement initiatives to measure and improve the efficiency of surgical activities.
In economics, efficiency is conceived as the relationship between the results obtained and the resources used; it is the ability to achieve a desired effect with the least possible resources. The operating room is one of the most complex units found in hospitals due to the large number of processes and sub-processes associated, directly or indirectly, with the production of surgeries. Monitoring specific indicators for this unit can help develop management strategies that allow to re-evaluate and reorganize the activities of the surgical service, with the purpose of improving its efficiency9.
Due to the characteristics of our hospital institution, numerous indicators can be used in the surgical block, some of them associated with infrastructure and others with processes and results. For an initial evaluation, we suggest the following objective criteria:
Number of surgical interventions performed.
Cancellation rate.
Starting time of the procedure.
Opportunity for surgical emergencies.
Starting time of anesthesia.
Starting time of surgery.
Time of admission to the UCPA/ICU.
Turnover or replacement time.
Proportion of operating rooms in use10.
Material and methods
With the approval of the Local Health Research Committee (CLIS), and in order to measure the indicators of efficient use of operating rooms, a retrospective longitudinal descriptive study was conducted on a group of 3,554 patients from our institution, using the information that had been recorded in their clinical files.
On a daily basis, the chief of the operating rooms is responsible for drawing up the surgical schedule, while the medical assistants are in charge of registering in said schedule the surgeries canceled and performed, and for each of them, the time of arrival of the patient to pre-anesthesia and the time of discharge from the operating room and/or the post-anesthesia care unit (PACU).
Inside the operating room, the circulating nurse, in agreement with the anesthesiologist, is tasked with fixing the time for the anesthetic-surgical procedure: time of admission to the operating room, start of anesthesia, start of surgery, end of surgery, end of anesthesia and transfer to the PACU.
The onset of the pandemic significantly impacted the services provided by our institution; thus, we decided to analyze the new environment for surgical activities. This is why we included in the study only those patients scheduled for surgery during the period from March 11, 2020 to March 31 of 2021.
The list of patients scheduled for surgery during our study period was obtained by reviewing the database of the surgical opportunity indicator (INDOQ). The name and social security number of each were recorded to draw up an initial list of patients. We then asked for the clinical files of these patients to the clinical file department and reviewed the copies of the operative reports of the anesthesiology service. These reports included the 4-30-27/90 forms «surgical interventions carried out in the operating room» and the 2430-021-076 forms «clinical records and nursing interventions of surgical patients». Applying the criteria for non-inclusion and exclusion of subjects, a definitive patient list was drawn up. Once this list was prepared, the clinical records of each patient were checked to obtain the information needed to assess the variables under study. These variables included:
Number of surgical interventions performed: number of surgeries performed during the study period.
Cancellation rate: number of surgeries canceled on the day of surgery during one year, divided by the number of surgical procedures scheduled in the operating rooms in the same year and multiplied by one hundred.
Surgery starting time: time in minutes between the time a surgery was scheduled and the time it starts.
Opportunity for surgical emergencies: time in minutes between the request for an urgent operation in the operating room and the start of the surgery.
Time for the start of anesthesia: time in minutes between the moment the patient enters the operating room until the start of anesthesia.
Time for surgery starts: time in minutes between the moment anesthesia is administered and the start of surgery.
Time for admission to the PACU/ICU: time in minutes between the moment anesthesia ends and the moment the patient is admitted to the post-anesthesia care unit or the intensive care unit.
Turnover or replacement time: time in minutes between the moment a patient leaves the operating room for the recovery room or the intensive care unit and the moment the next patient enters for surgery.
Rate of use of operating rooms: time each operating room is occupied during the scheduled surgery day. Sum of the time it takes to perform each surgery plus turnover time, divided by the time available.
The data were collected using an easy-to-apply form. The process of identifying patient files was carried out by the resident anesthesiology physician.
The variables were analyzed using descriptive statistics: measures of central tendency and dispersion. Quantitative variables with normal distribution were described by arithmetic mean and standard deviation. Qualitative nominal variables were described by rates and proportions.
The data were processed using the statistical program SPSS for Windows, version 25.0. The results were presented in Tables and graphs.
Results
A total of 3,554 surgeries (1,309 emergency surgeries and 1,979 elective surgeries) were scheduled in the period under study, of which 266 were deferred (Table 1). The reported causes for surgery were as follows: lack of a bed (25.6%); the patient did not show up (12.0%); intercurrent disease (9.4%); other causes (53.0%), including insufficient operating room time due to a prolonged surgery, priority given to an emergency surgery, change of surgical criteria, another surgery was moved up in the schedule, etcetera (Table 2).
Table 1: Analysis of scheduled surgeries.
| Surgeries | n (%) |
|---|---|
| Deferred | 266 (7.48) |
| Performed • Elective • Urgent |
1,979 (55.68) 1,309 (36.84) |
| Total | 3,554 (100.00) |
Percentage calculated according to the total number of scheduled surgeries (N = 3,554)
Source: surgery reports.
Table 2: Causes of surgical deferral.
| Causes | n (%) |
|---|---|
| No bed available | 68 (25.6) |
| The patient did not show up | 32 (12.0) |
| Intercurrent illness | 25 (9.4) |
| Insufficient operating room time due to prolonged surgery | 20 (7.5) |
| Priority given to emergency surgery | 17 (6.4) |
| Change of surgical criteria | 15 (5.6) |
| Surgery was moved forward | 10 (3.8) |
| Intraoperative death | 10 (3.8) |
| Incomplete study | 6 (2.3) |
| Lack of special instruments or equipment (nonexistent) | 6 (2.3) |
| Fasting was not obeyed | 4 (1.5) |
| Lack of blood | 4 (1.5) |
| By surgeon’s indication | 4 (1.5) |
| Internal medicine did not authorize | 3 (1.3) |
| Absence of the anesthesiologist without warning | 3 (1.3) |
| Change of clinical picture (surgical indication) | 3 (1.3) |
| Change of anesthetic criteria | 2 (0.7) |
| Cardiology did not authorize | 2 (0.7) |
| Need for cardiological evaluation | 2 (0.7) |
| Poorly prepared patient | 2 (0.7) |
| Scheduling error | 2 (0.7) |
| Insufficient nursery staff | 1 (0.4) |
| Surgeon absence due to disability | 1 (0.4) |
| Hematology did not authorize | 1 (0.4) |
| Preanesthetic complication (due to medication) | 1 (0.4) |
| No clinical file | 1 (0.4) |
| Lack of authorization from the patient or person responsible | 1 (0.4) |
| Patient under study in another area | 1 (0.4) |
| Lengthened times | 1 (0.4) |
| Patient deceased before surgery | 1 (0.4) |
| Others | 17 (6.4) |
| Total | 266 (100.0) |
Percentage calculated according to the total number of scheduled surgeries (N = 3,554)
Source: surgery reports.
Regarding the proportion of surgical procedures by specialty, ophthalmological surgeries had the highest percentage (27.24%), followed by urological surgeries (20.26%) and neurological surgeries (17.53%) (Figure 1). Of the surgeries performed, most were carried out during the morning shift (Table 3). Table 4 shows the time corresponding to each process of the surgical procedure.
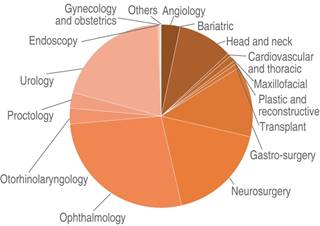
Figure 1: Surgeries by specialty. Percentage calculated according to the total number of scheduled surgeries (N = 3,554). Source: surgery reports.
Table 3: Analysis of surgeries by shift.
| Surgeries | n (%) |
|---|---|
| Deferred | 266 (7.48) |
| Performed Morning Evening Night |
2,213 (62.26) 767 (21.58) 574 (16.16) |
| Total | 3,554 (100.00) |
Percentage calculated according to the total number of scheduled surgeries (N = 3,554).
Source: surgery reports.
Table 4: Surgical times.
| Variable | Time (min) |
|---|---|
| Starting time of the procedure | 42.32 ± 37.04 |
| Opportunity for surgical emergencies | 104.69 ± 102.55 |
| Starting time of anesthesia | 10.11 ± 9.85 |
| Starting time of surgery | 40.03 ± 24.68 |
| Time of admission to the UCPA/ICU | 15.35 ± 29.94 |
| Turnover or replacement time | 177.97 ± 174.33 |
PACU = post-anesthesia care unit. ICU = Intensive Care Unit.
Source: surgery reports.
During the period under study there were 296 days of surgical activity. The recorded surgical time was 27.70% active time and 72.30% inactive time.
Discussion
During the SARS-CoV-2 (COVID-19) pandemic there has been a general trend towards an increase in the number of patients awaiting a surgical procedure. This represents a serious problem, since it significantly compromises the principle of equity that inspires public health systems around the world, giving rise to discontent and complaints by the users. It is thus necessary to monitor performance indicators in order to check whether medical institutions are meeting the population needs effectively, especially in this period of uncertainty.
Following institutional regulations saves time and resources; it also avoids conflicts11. Regulations indicate that the beginning of the surgical procedure should take 15 minutes12, which differs significantly from what we observed (42.32 ± 37.04 min). Although it is true that this excess time at the beginning of the procedure is attributable to the changes in preoperative logistics induced by the pandemic, this could be improved by starting the intervention at the scheduled time in order to take full advantage of the time allotted to it. In the present study, only 106 procedures (2.98%) began at the scheduled time. Other authors reported longer starting times. Requesens et al13. reported an average of 67 minutes, while Martín-Pérez reported a starting time of 12.5 minutes14.
Once the patient leaves the operating room, there needs to be a high degree of coordination between the team tasked with cleaning the operating room and the team getting the next patient into it, a process that should last 30 ± 15 minutes15-19. In our hospital institution, the average duration of this combined process was 104.69 ± 102.55 minutes. Other studies have shown that the prolongation of the turnover time has repercussions such as staff dissatisfaction, delays, use of overtime and cancellation of surgeries20. In this regard, the results of the present study are well above the time reported by other studies. Prieto et al21. reported a turnover time of 20 minutes, while Jerico MC13 reported a turnover time of 50.2 minutes.
The correct operation of the surgical block can be measured by means of the index of operating room occupancy or surgical performance, which is the ratio between the surgical time used and the surgical time available on the same day in the same operating room10. Other authors reported significantly lower values10,13,15-21. This is ultimately attributable to the restrictions imposed by the COVID-19 throughout the world.
The efficient use of the operating room depends on the fulfillment of specific functions by all the personnel involved and on a strict adherence to scheduled times.
The performance of the operating rooms depends on the first case of the day beginning at the scheduled time, on minimizing turnover time, maintaining a low cancellation rate, making few scheduling errors and drawing up a precise surgical schedule.
Surgery is an indispensable therapeutic alternative in medical practice; it saves lives and increases the survival of patients with degenerative and chronic pathologies. The number of surgeries during the COVID-19 pandemic will increase as new protection measures and equipment for health staff and patients facilitate and improve surgical procedures. However, it is essential to adapt to the new conditions, since the risk of infection by SARS CoV-2 is still present, adding to the complications inherent to these interventions. Institutional efforts are aimed at improving the response capacity of surgical teams in terms of the diversity of procedures and the timeliness with which surgical services are provided. In this work we report the impact of the COVID-19 pandemic on the intensity, diversity and dynamism of surgical activity in an institutional setting.
Conclusions
A surgical unit is made up of an entire work team, so good organization is required to manage resources appropriately. One of the most important resources is surgical time. Optimal use of the operating room depends on the efficient performance of the staff, which should take advantage of all the surgical time available to it and adhere to the schedule.
The results of the present study show that the time used by surgical teams in the institution under study does not conform with established standards, and differs enormously from the results published by other authors.
Regarding the management and organization of the surgical day, a significant improvement could be achieved by starting the first intervention of the day as closely to the scheduled time as possible, reducing turnover times and avoiding mistakes in the surgical schedule. These measures could be the key to a successful surgical unit.
Analyzing the time taken up by each surgical procedure, as this work has done, can undoubtedly help make an error-free surgical schedule. Knowing the average time of each surgical intervention and the average time for patient turnover can help make full use of all the time available for the surgical day, minimizing residual time, the prolongation of surgical procedures and cancellations due to lack of time.
As future lines of research, I propose the analysis of surgery times, of all specialties, with respect to certain clinical aspects of the patients and other aspects of the intervention, in order to observe if the study variables influence or not the duration of the intervention.

