











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Cardiovascular surgical teams are accustomed to use various risk adjustment models (scores) to predict perioperative morbidity and mortality with the purpose of establishing management plans for each patient. The clinical practice guidelines of the American Heart Association/American College of Cardiology consider it reasonable to use such models for two purposes: to control surgical and institutional quality and to estimate the risk of death from specific causes1.
Surgical risk is an extremely complex subject, particularly in cardiac surgery, as there are many different factors that can lead to an adverse result. Statistical predictions about the possibility of an eventuality during cardiac surgery are based on general trends or descriptive data, not on individual patients, and so it has been suggested that perioperative risk should be interpreted as the intersection of multiple components, including: the physical characteristics of the patient, the clinical context of the disease and the aggressiveness of the planned surgical intervention2. The complexity of the problem is such that various instruments have been developed to assess the influence of these factors on patient survival3.
One of these instruments is the surgical risk score for heart valve surgery (VMCP).
The VMCP score is a simplified score, created and validated in the Cardiology Institute of the Faculty of Medicine of the University of Sao Paulo, in Sao Paulo, Brazil, based on a study of 764 patients. This score is based on four fundamental parameters that characterize heart valve diseases: V [valvular lesion]; M [myocardial function]; C [coronary artery disease]; P [pulmonary artery pressure]. These are classified into four categories, and the sum of the score of the four parameters make up the VMCP score. In the institution in which it was developed, this score has been used to identify patients with a severe preoperative disease, and to assess the correlation between postoperative mortality and morbidity in valve surgery4.
Since the score was developed for a population that is different from the population of our hospital, we evaluated the performance of the score in our population.
If validated, the VMCP would facilitate the identification of at-risk patients and the development of management guides that could help minimize hospital costs and unnecessary risks. We would be able to use a simple score based on straightforward clinical parameters that would help improve the postoperative prognosis of our patients.
Subjects and methods
With the approval of the Hospital Scientific Research Commission in order to determine the validity of the VMCP score, a prospective cohort study was carried out.
All patients, of any age and gender, who underwent elective or urgent heart valve surgery in our hospital unit during the period from January 1 to December 31, 2019, were identified using the surgical schedule, and the VMCP score was applied using data obtained with an easy-to-fill form, with questions designed for that purpose. A previous evaluation of surgical risk was performed by the resident of cardiothoracic surgery.
Surgical mortality and morbidity, as well as the presence of comorbidities and intrahospital parameters, were evaluated 30 days after surgery by reviewing the clinical record.
The internal consistency and discriminatory power of the model were analyzed to assess its validity. The internal consistency was evaluated using Cronbach’s Alpha Coefficient. A value greater than or equal to 0.7 indicated that the model predicted well the probability of postoperative morbidity and mortality in the patients. The discriminatory power was analyzed by calculating the area under the ROC curve. A value less than or equal to 0.5 indicated that the model did not discriminate better than chance, while values close to 1 indicated an excellent discriminatory power. The sample was divided into two groups at a cut-off point of 8, which was previously established by Grinberg et al4. Morbidity and mortality in the two groups were compared using the χ2 test. The continuous variables were expressed as mean ± standard deviation; the categorical variables were expressed as percentages. The analysis was performed using SPSS v.25.0 (SPSS, Inc., Chicago, IL, USA).
Results
The data used to validate the VMCP score were obtained from a clinical series of 239 patients. The estimated morbidity was 35.98% while the mortality was 2.09%, since eighty-six patients presented perioperative complications, and five of them died. These findings suggest the need for studying the predictive capacity of risk stratification models for patients with heart valve disease.
Patients between 22 and 92 years old were included, most of them male. The clinical and demographic data of the patients are summarized in Table 1.
Table 1: Demographic data of the population. N = 239.
| Variable | |
|---|---|
| Age, years | 59.85 ± 13.74 |
| Gender (n) | |
| Male | 129 |
| Female | 110 |
| Valvulopathy, % | |
| Tricuspid | 4.6 |
| Mitral | 20.9 |
| Aortic | 46.4 |
| Pulmonary | 0.4 |
| Multiple | 13.0 |
| Valvular + ischemic heart disease | 14.6 |
| Type of surgery (E/U) | 237/2 |
| NYHA (I/II/III/IV) | 23/136/78/2 |
| CARE (I/II/III/IV/V/VI) | 38/178/19/2/0/2 |
| Cardiovascular risk factors, % | |
| Smoking | 53.1 |
| Hypertension | 79.9 |
| Diabetes mellitus | 40.6 |
| Time spent in the surgical anesthetic state, min | |
| Anesthetic time | 272.62 ± 77.65 |
| Surgical time | 235.48 ± 71.05 |
| Extracorporeal circulation time | 120.42 ± 62.1 |
| Aortic impingement time | 102.30 ± 74.26 |
| Type of valve prosthesis, % | |
| Mechanical | 68.2 |
| Biological | 30.5 |
| Mixed | 1.3 |
BMI = Body mass index, NYHA = New York Heart Association. CARE = Cardiac anesthetic risk.
The internal consistency of the model was poor (Alpha Cronbach’s coefficient = 0.59), which indicated that the parameters considered were very weakly correlated. This made us conclude that the score does not fit the population of our hospital.
Calibration and discrimination tests were used to assess the predictive capacity of the system.
The VMCP score was applied to all patients; based on the score values, the study population was divided into 2 groups: low risk and high risk.
Sixty-three high-risk patients presented serious complications; among those who did not, 79 patients were at high risk. Four deceased patients had been previously classified in the high-risk group; of the patients at low risk, only one suffered perioperative death (Table 2).
Table 2: Distribution of patients according to the VMCP score.
| Serious complications | Death | ||||
|---|---|---|---|---|---|
| VMCP score | Yes | No | Yes | No | Total |
| High risk | 63 | 79 | 4 | 138 | 142 |
| Low risk | 23 | 74 | 1 | 96 | 97 |
| Total | 86 | 153 | 5 | 234 | 239 |
The median score of low-risk patients was 7 (5-7); the median score of high-risk patients was 9 (8-14). Regarding the prediction of morbidity and mortality, the sensitivity, the negative predictive value and the positive likelihood ratio of the score were high. Table 3 shows the quality indices of the score.
Table 3: Quality indices of the VMCP score.
| Quality indices | VMCP score |
|---|---|
| Morbidity | |
| Prevalence* | 35.98 |
| Sensitivity* | 73.25 |
| Specificity* | 48.36 |
| Positive predictive value* | 44.36 |
| Negative predictive value* | 76.28 |
| Positive likelihood ratio | 1.41 |
| Negative probability ratio | 0.55 |
| Mortality | |
| Prevalence* | 2.09 |
| Sensitivity* | 80.00 |
| Specificity* | 41.02 |
| Positive predictive value* | 2.81 |
| Negative predictive value* | 98.96 |
| Positive likelihood ratio | 1.35 |
| Negative probability ratio | 0.48 |
* = percentage.
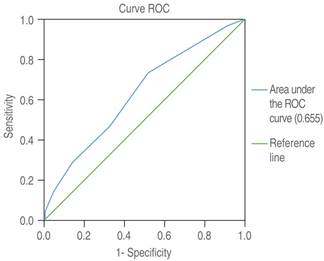
The ROC curve was created by plotting the true positives (sensitivity) and true negatives (1-specificity) at the cut-off point. The area under the curve indicated the discriminating power of the model, that is, its ability to distinguish between those patients who were predicted to have serious complications and/or perioperative death, and those who were not. It is important to note that the area under the curve for complications was 0.630 (Figure 1), and for the perioperative death 0.655 (Figure 2), indicating that the predictive ability of the model is poor.

Discussion
For several years, different models derived from mathematics, statistics and other sciences have helped predict the future evolution of patients through quantitative methods, and, although with certain restrictions, to make, in many cases, more accurate decisions5,6. This is the purpose of risk scores, which could be defined as an algorithm or clinical prediction rule that can help physicians to interpret the information obtained about the patient5,7,8.
At present there are multiple risk scores that can be used to categorize patients. In this study, we evaluated the VMCP risk model/score. Although the main purpose of this score is adapt the surgical treatment of heart valve diseases to the individual risk of each patient, it did not produce an adequate classification of our patient population, as evidenced by the poor predictive capacity of the model according to the results regarding the predictive capacity of this score were not those expected at the time the ROC curve was plotted.
This result could be explained because when a validation is carried out, by a different group of researchers or in a group of patients with different clinical settings. Since it is difficult to fully reproduce the clinical settings present in another study, since there are always natural variations that do not appear in the initial study9,10.
Heart valve pathologies are increasingly common, and so valve replacement has become an increasingly common intervention. The most prevalent preoperative diagnosis in our study was aortic valvulopathy followed by mitral valve disease, which coincides with the results reported by other authors11,12.
Paylo-Hernández and colleagues have pointed out that patients with aortic valve disease are more likely to present morbidity and mortality than those with other valve diseases due to their greater longevity, their low preoperative functional class, moderate to severe reduction of left ventricular function, and increased incidence of coronary disease and degenerative pathologies, as well as increased association with perioperative bleeding, which can led to reoperation and death13. In our population, 25.2% of patients with aortic valve disease suffered major complications, while 0.9% died. These outcomes differ from those reported by other authors in which the morbimortality of aortic valve disease did not surpass that of other valve diseases. Another independent risk factor for morbidity and mortality is the presence of multiple valve pathologies. In our study, the mortality of bivalvular procedures was 0.
Current guidelines indicate valve replacement for patients with ventricular dysfunction (LVEF < 55%) and increased ventricular size (end-systolic diameter [ESD] ≥ 45 mm)14-20. In our study, 83.3% of the patients who suffered serious complications and/or death showed ventricular ejection fractions equal to or greater than 50%.This may be due to the fact that contractility indexes (LVEF), although useful, often do not represent the true contractile state of the left ventricle.
The American Heart Association (AHA) considers ischemic heart disease as an important predictor of death in patients with heart valve disease, as there is a positive relation between it and mortality rates. Likewise, combined surgery implies a variable increase in the risk of mortality, ranging from 1.5 to 18% (depending on the type of valve), compared to isolated valve replacement surgery13.
In our population, 14.6% of patients with heart valve disease had concomitant coronary disease, in contrast with the proportion reported by Sodian et al21 of up to 40%. Morbidity and mortality did not show differences between patients with heart valve disease and concomitant coronary disease, and those who underwent isolated valve replacement surgery.
In valve replacement procedures, mortality is influenced by a fourth factor, pulmonary artery pressure. Pulmonary hypertension is a pathology of low prevalence but with a very significant influence on morbidity and mortality, as shown by Ramakrishna et al., among other authors, who found that this variable was a significant risk factor for mortality after surgery22,23. In our study, pulmonary hypertension was present in 96.5% of the patients who suffered serious complications and/or death, and in 94.1% of those who did not.

