











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
INTRODUCTION
Breast cancer is the most common type of cancer in women in the world, with an incident of 1.7 million of new cases in 2016 [1]. For women, it was the most common cancer in 131 countries and cause of cancer deaths in 112 countries [1] [2] [3] [4] [5] [6]. In 2018 the International Agency for Research on Cancer estimated 2.08 million of new breast cancer cases worldwide [7].
After breast cancer surgery, women might develop musculoskeletal impairments that affect movements of the upper limbs and reduce the quality of life. Complications following breast cancer surgery include infection, swelling, hematoma, seroma and psychological factors such as, anxiety or depression [3] [8] [9] [10] [11]. The complications are not always localized on the region of the surgery, as many of the treatments have larger regional systemic effects on body structures and functions [3] [8] [11] [12] [13]. Although women report upper limb symptoms between 6 months and 3 years after breast cancer, some of the comorbidities could remain for a longer-term. The etiology of morbidity seems to be multifactorial, with the most consistent risk factors being those associated with extension of cancer treatment [14].
The mastectomy produces dysfunctions on the upper limbs in a mid or long term, causes lymphedema, persistent pain [9] [15], weakness and restricts the movement of the shoulder [10] [14] [16]. Furthermore, it has been found that muscle activation can be affected after breast cancer surgery. The effect depends on the type of surgery and type of reconstruction of the breast [17] [18] [19] [20] [21]. It has been thought that the most frequent complications include long-term weakening of muscles within the shoulder and upper limb at the affected side [4]. It is believed that if one muscle is compromised, then other muscles might become more active to compensate for the lost movement. However, the muscle electrical activity can be influenced by age, dominance or pain on the limb [20].
Movements of the upper limbs and head are recommended as rehabilitation after a breast cancer surgery. Upper-body morbidity may be treatable with physical therapy. It has been found a 50-53% reduction in the risk of breast cancer deaths in women who are physically active after a breast cancer diagnosis [6] [14]. Although rehabilitation represents an alternative to reduce the complication after breast cancer surgery, many of the patients do not receive the appropriate treatment to address the complications [22] [23] [24].
The complications after mastectomy are well known, evaluated and treated from measurements such as goniometry, observation and strength tests with manual resistance [8] [10]. However, they do not provide specific scenarios for kinematic discontinuities of the shoulder movement. Moreover, there are few studies focused on the analysis of the biomechanics of the upper limbs on a three-dimensional space after breast cancer treatment [20] [25] [26] [27]. Biomechanical and muscular activation studies with equipment with higher accuracy are required to recognize these affectations and identify areas of opportunity to improve physiotherapeutic intervention plans.
Therefore, the objective of this research is to analyze the movement of the shoulder and the electrical activity of the trapezius, deltoid and pectoralis major muscles in patients with unilateral breast cancer surgery.
MATERIALS AND METHODS
Experimental protocol
Eight right-handed female participants, mean age 46.5 ± 5.45 years and mean body mass 71.21 ± 13.33 kg with unilateral breast cancer surgery (mastectomy), without breast reconstruction and without lymphedema symptoms after the surgery were included in the research, see Table 1. The sampled population was selected with non-probabilistic sampling. After the surgery, all the participants performed a rehabilitation process of the upper limbs. This rehabilitation was performed for 60 days and involved series of active movements of the head, flexion-extension and abduction-adduction of the arms. Participants which could not follow instruction, presented post-surgery issues or did not complete the rehabilitation were excluded.
Table 1 Anthropometric data and affected side of the patients. SD means Standard Deviation.
| Subject | Age (years) | Mass (kg) | Height (m) | Affected Arm | Dominant Hand |
|---|---|---|---|---|---|
| 1 | 36 | 61.35 | 1.62 | Left | Right |
| 2 | 50 | 53.6 | 1.5 | Right | Right |
| 3 | 50 | 57.6 | 1.48 | Right | Right |
| 4 | 51 | 82.3 | 1.56 | Left | Right |
| 5 | 45 | 64.05 | 1.55 | Right | Right |
| 6 | 52 | 84.3 | 1.64 | Right | Right |
| 7 | 42 | 86.1 | 1.72 | Left | Right |
| 8 | 46 | 80.4 | 1.6 | Right | Right |
| Mean | 46.50 | 71.21 | 1.58 | -- | -- |
| SD | 5.45 | 13.33 | 0.078 | -- | -- |
Once the rehabilitation was completed, the participants continue with the evaluation of the flexion-extension, abduction-adduction movements and the electrical activity of the upper trapezius, middle deltoid, and pectoralis major muscles. The motion of the arms was measured with seven infrared cameras of the VICON system at a sampling frequency of 100Hz (Nexus version 2.8.1.111866h x86, Vicon Motion System Ltd. Oxford UK). The muscle electrical activity was measured with surface electromyography (EMG) at a sampling frequency of 1000Hz (Myomonitor IV EMG System Bagnoli Delsys Inc, Boston MA, USA).
All the participants were asked to wear comfortable clothes to allow free execution of the movements. The participants were informed about the function and main parts of the motion capture system and the EMG equipment. They were allowed to perform exercises prior to the experimental tests to familiarize themselves with the equipment and the protocol. Simultaneously, personal data were recorded and saved on an encrypted computer for safekeeping. Then, the participants performed three trials of bilateral flexion-extension and abduction-adduction movement of the arms. Each trial consisted of ten cycles performed over a period of 20 seconds paced using a metronome. Three minutes were allowed among trials to give rest to the patients and avoid fatigue.
Subject preparation
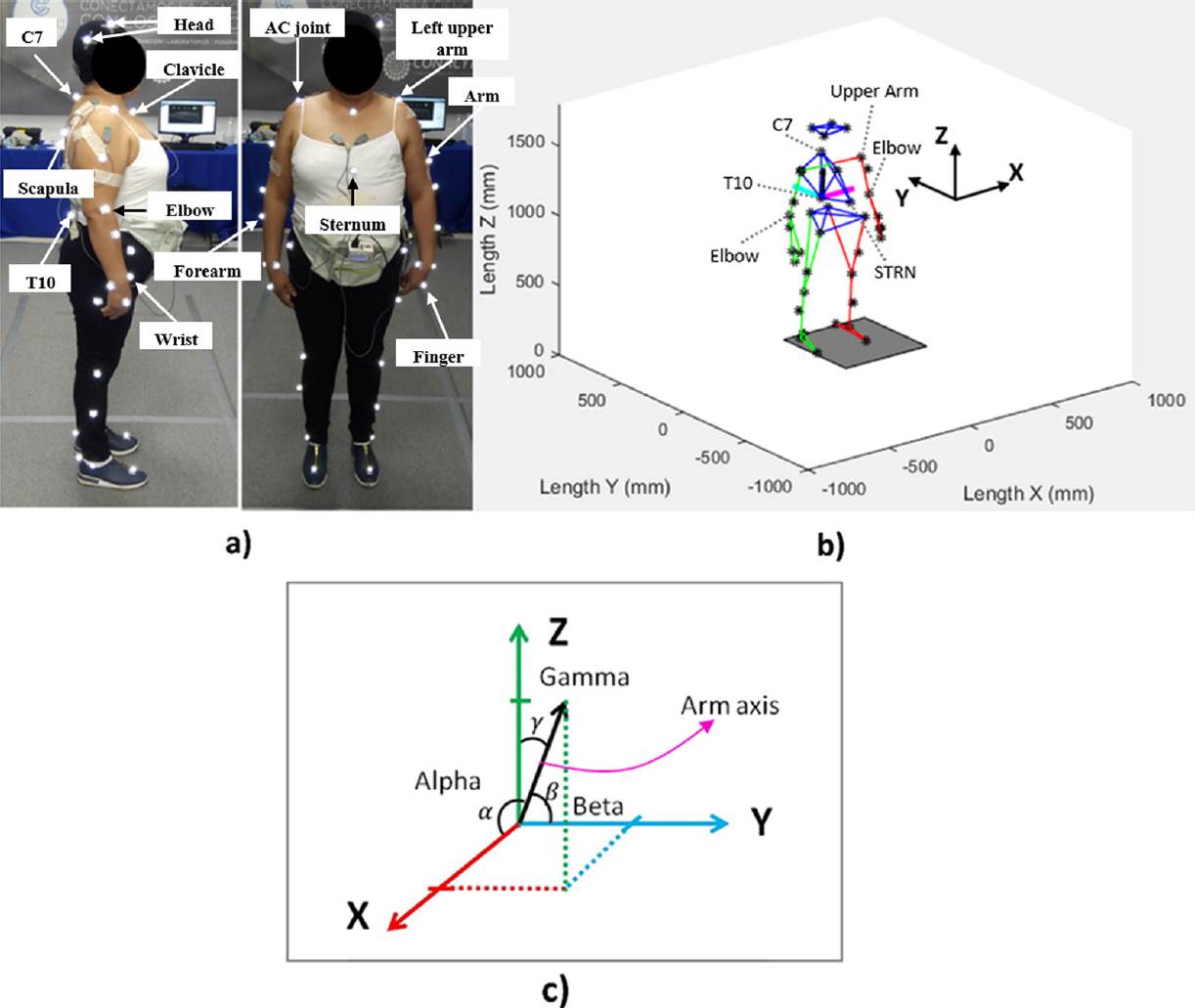
First, the setup of the infrared cameras of the VICON system was performed. Then, 39 spherical markers (10mm of diameter) were placed on anatomical bony landmarks of each participant, Figure 1a. The passive markers (inactive) were attached to the skin with double-sided tape following the VICON manual and the markers were labeled following the PlugInGait FullBody template. Thereafter, the skin on the upper trapezius, middle deltoid and pectoralis major muscles was cleaned with exfoliating cream and isopropyl alcohol for the placement of the electrodes. The placement of the electrodes was done following the recommendations of Surface Electromyography for the NonInvasive Assessment of Muscles (SENIAM). Furthermore, a ground/reference electrode was placed on the lateral epicondyle of the left arm.
Data processing
The data of the markers were exported to Matlab R2015a (version 8.5.0.197613, The MathWorks Inc., Natick, Massachusetts, USA) in a txt file for processing. An orthogonal coordinate system was created in the 10th thoracic vertebra (T10) using the markers of the 7th cervical vertebra (C7) and the sternum (STRN). The X axis pointed to the lateral side, the Y axis pointed backwards and the Z axis pointed upwards as shown in Figure 1b. Then, a rotation matrix 3x3 with the three-unit vectors was created. Furthermore, a vector was created between the upper arm and the elbow markers in order to describe the movement of the arm. Finally, the vector of each arm was orientated with respect to the coordinate system of the thorax. This was done by multiplying the inverse matrix times the vector of the arm. Once the transformation of the vector was done, the direction angles Alpha (X), Beta (Y) and Gamma (Z) were calculated as shown in Figure 1c. All the cycles from the three trials undertaken by each participant for each motion were averaged and time normalized from zero to 100% of the movement time.
The raw EMG data was filtered with a 2-pole zero-lag Butterworth band pass filter with cut-off frequencies of 5 and 400Hz in order to retain as much as possible of the electrical activity data and reject high frequency noise. The cut-off frequencies were obtained from a frequency spectrum analysis of the raw EMG data [28]. Then, the root mean square (RMS) value of every muscle burst for all the trials was calculated within a window of 100ms. The RMS window was calculated at the maximum peak of each burst (50ms forwards and 50ms backwards). Finally, the RMS values of the muscles were averaged and then, the healthy side was compared versus the affected side.
Statistical analysis
In order to determine the effect of the unilateral breast cancer surgery on the shoulder, a Student’s t-test for dependent samples was performed. The comparison of the direction angles and the electrical activity of the muscles was done for both sides. The significance level was taken to be p < 0.05.
RESULTS AND DISCUSSION
Flexion-Extension movement
The direction angles from Figure 2a show the movement of the arms during the flexion-extension motion (subject 8). As the movement is executed mainly in the sagittal plane, the direction angle of the X axis (alpha) does not change significantly. However, the movement of the arms with respect to the Y and Z axes (beta and gamma) changes. Figure 2a shows that the affected arm (subject 8-right arm) reduces the direction angles (beta and gamma) when the arm is reaching the maximum elevation level. The direction angle with respect to the Y axis at 50% of the cycle was 118.52 ± 5.28 and 136.76 ± 2.56 degrees for the left and right arm respectively. This means that the right arm (affected) does not elevate as much as the left arm.

Figure 2 a) Direction angles of the flexion-extension movement of one subject and b) Direction angles of the abduction-adduction movement of one subject. Comparison of both sides, affected and non-affected side (Subject 8).
Similarly, the comparison of both arms with respect to the vertical Z axis showed that the right arm did not elevate as much as the left one. The direction angle with respect to the vertical Z axis at 50% of the cycle was 28.77 ± 4.98 and 48.27 ± 2.45 degrees for the left and right arm respectively, Figure 2a.
Table 2 shows the mean and standard deviation values (alpha, beta and gamma) of the eight subjects during the flexion-extension motion of both arms. In general, it was found that the affected side presented less amplitude of motion, excluding subject 5. The statistical analysis showed a significant reduction of the movement in the affected side (p < 0.05).
Table 2 Direction angles of the flexion-extension and abduction-adduction movement of all participants. The mean and standard deviation values are from the 50% of the cycle motion.
| Direction angles: Flexion-Extension movement | |||||||||
| ALPHA (°) | p | BETA (°) | p | GAMMA (°) | p | ||||
| Subject | Left (SD) | Right (SD) | 0.05 | Left (SD) | Right (SD) | 0.05 | Left (SD) | Right (SD) | 0.05 |
| 1 | 56.72 (3.02) | 48.02 (2.84) | 0.000 | 116.86 (2.95) | 97.72 (1.94) | 0.000 | 45.44 (2.84) | 43.06 (2.77) | 0.000 |
| 2 | 84.24 (1.14) | 86.86 (3.81) | 0.010 | 108.52 (5.86) | 113.87 (7.21) | 0.000 | 19.6 (5.45) | 24.6 (6.30) | 0.000 |
| 3 | 71.60 (2.31) | 77.65 (1.60) | 0.000 | 114.35 (2.25) | 144.61 (1.98) | 0.000 | 31.32 (3.18) | 57.48 (1.83) | 0.000 |
| 4 | 56.86 (1.44) | 82.71 (0.90) | 0.000 | 117.09 (1.70) | 115.47 (4.05) | 0.030 | 45.4 (1.52) | 26.71 (3.75) | 0.000 |
| 5 | 77.95 (3.00) | 86.51 (1.14) | 0.000 | 135.59 (4.11) | 124.2 (2.70) | 0.000 | 48.23 (3.19) | 34.46 (2.71) | 0.000 |
| 6 | 83.21 (3.33) | 70.92 (2.55) | 0.000 | 139.62 (9.20) | 144.82 (6.78) | 0.000 | 50.63 (8.82) | 61.92 (6.47) | 0.000 |
| 7 | 62.19 (3.48) | 81.98 (2.52) | 0.000 | 125.71 (2.34) | 115.24 (3.71) | 0.000 | 48.49 (2.52) | 26.8 (3.50) | 0.000 |
| 8 | 92.43 (2.18) | 80.79 (1.57) | 0.000 | 118.52 (5.28) | 136.76 (2.56) | 0.000 | 28.77 (4.98) | 48.27 (2.45) | 0.000 |
| Direction angles: Abduction-Adduction movement | |||||||||
| ALPHA (°) | p | BETA (°) | p | GAMMA (°) | p | ||||
| Subject | Left (SD) | Right (SD) | 0.05 | Left (SD) | Right (SD) | 0.05 | Left (SD) | Right (SD) | 0.05 |
| 1 | 29.30 (3.81) | 31.66 (3.32) | 0.008 | 101.42 (2.64) | 78.45 (2.27) | 0.000 | 63.52 (3.47) | 61.11 (4.05) | 0.007 |
| 2 | 102.43 (2.61) | 116.24 (3.47) | 0.000 | 102.48 (2.92) | 111.99 (2.96) | 0.000 | 17.88 (3.31) | 35.5 (3.90) | 0.000 |
| 3 | 21.52 (3.97) | 32.36 (2.48) | 0.000 | 101.51 (2.30) | 121.09 (1.70) | 0.000 | 72.21 (3.81) | 82.99 (4.45) | 0.000 |
| 4 | 60.40 (2.29) | 90.07 (0.91) | 0.000 | 116.33 (2.75) | 113.71 (2.23) | 0.000 | 41.7 (1.96) | 23.73 (2.22) | 0.000 |
| 5 | 80.88 (2.82) | 82.46 (2.21) | 0.030 | 119.86 (1.23) | 114.53 (1.10) | 0.000 | 31.64 (1.29) | 25.9 (1.13) | 0.000 |
| 6 | 78.60 (10.92) | 64.29 (7.01) | 0.000 | 118.04 (2.19) | 126.53 (4.96) | 0.000 | 32.23 (6.52) | 48 (1.14) | 0.000 |
| 7 | 47.36 (11.7) | 73.82 (15.15) | 0.000 | 115.01 (5.63) | 110.63 (4.71) | 0.000 | 53.62 (9.08) | 28.8 (10.90) | 0.000 |
| 8 | 92.95 (16.81) | 69.9 (12.65) | 0.000 | 118.23 (4.22) | 130.08 (4.37) | 0.000 | 32.67 (8.61) | 48.55 (8.85) | 0.000 |
Abduction-Adduction movement
Figure 2b shows the three direction angles (alpha, beta and gamma) of the abduction-adduction movement of the arms in subject number 8. The movement was performed mainly in the frontal plane. Therefore, the beta angle behaved almost like a flat line. Thinking that the major effect of the surgery could be found at the maximum elevation level of the arms, the analysis of the direction angles was done at 50% of the cycle. The direction angle with respect to the X axis at 50% of the cycle for this subject was 92.95 ± 16.81 and 69.9 ± 12.65 degrees for the left and right arm respectively. This means that the right arm (affected) does not elevate as much as the left arm. Similarly, the comparison of both arms with respect to the vertical Z axis showed that the right arm did not elevate as much as the left one. The direction angle with respect the Z axis at the 50% of the cycle was 32.67 ± 8.61 and 48.55 ± 8.86 degrees for the left and right arm respectively, Figure 2b.
The mean and standard deviation values (direction angles) of the eight subjects during the abduction-adduction movement are presented in Table 2. The gamma angles at 50% of the cycle motion indicate that the affected arm does not elevate as much as the non-affected arm, excluding subject 5. Similarly, the direction angle alpha indicates that the affected arm does not elevate as much as the opposite one, excluding subjects 2, 3, and 5. The statistical analysis showed a significant reduction of the movement in almost all affected sides (p < 0.05).
Muscle electrical activity during the flexion-extension movement
For flexion-extension movement, the trapezius showed the highest electrical activity followed by the deltoid muscle. Although the electrical activity was higher in some cases, the statistical analysis did not show a significant difference, as shown in Table 3 (p > 0.05). The trapezius in subject one was the only muscle with a significant statistical difference between the affected and non-affected side (p = 0.047). However, there was not a specific trend of the data to justify that the affected side increases or decreases the electrical activity after the rehabilitation post-surgery.
Table 3 Root mean square values of the electrical activity during the flexion-extension and abduction-adduction movement.
| RMS of the EMG: Flexion-Extension movement | |||||||||
| TRAPEZIUS (mV) | p | DELTOID (mV) | p | PECTORALIS (mV) | p | ||||
| Subjects | Left (SD) | Right (SD) | 0.05 | Left (SD) | Right (SD) | 0.05 | Left (SD) | Right (SD) | 0.05 |
| 1 | 0.411 (0.089) | 0.139 (0.018) | 0.047 | 0.043 (0.019) | 0.021 (0.008) | 0.669 | 0.010 (0.005) | 0.015 (0.005) | 0.839 |
| 2 | 0.362 (0.057) | 0.175 (0.044) | 0.072 | 0.195 (0.058) | 0.200 (0.051) | 0.930 | 0.009 (0.002) | 0.011 (0.002) | 0.869 |
| 3 | 0.061 (0.009) | 0.069 (0.026) | 0.894 | 0.057 (0.015) | 0.065 (0.017) | 0.846 | 0.026 (0.015) | 0.014 (0.007) | 0.740 |
| 4 | 0.277 (0.038) | 0.141 (0.042) | 0.170 | 0.099 (0.015) | 0.025 (0.008) | 0.153 | 0.006 (0.005) | 0.006 (0.002) | 0.997 |
| 5 | 0.204 (0.039) | 0.099 (0.025) | 0.240 | 0.041 (0.006) | 0.027 (0.004) | 0.665 | 0.010 (0.006) | 0.018 (0.004) | 0.794 |
| 6 | 0.146 (0.014) | 0.151 (0.035) | 0.940 | 0.037 (0.007) | 0.030 (0.010) | 0.824 | 0.007 (0.002) | 0.008 (0.002) | 0.966 |
| 7 | 0.234 (0.055) | 0.170 (0.028) | 0.509 | 0.059 (0.009) | 0.071 (0.010) | 0.797 | 0.041 (0.010) | 0.011 (0.004) | 0.397 |
| 8 | 0.091 (0.013) | 0.108 (0.015) | 0.682 | 0.035 (0.006) | 0.020 (0.005) | 0.705 | 0.018 (0.004) | 0.007 (0.003) | 0.709 |
| RMS of the EMG: Abduction-Adduction movement | |||||||||
| TRAPEZIUS (mV) | p | DELTOID (mV) | p | PECTORALIS (mV) | p | ||||
| Subjects | Left (SD) | Right (SD) | 0.05 | Left (SD) | Right (SD) | 0.05 | Left (SD) | Right (SD) | 0.05 |
| 1 | 0.389 (0.077) | 0.144 (0.019) | 0.043 | 0.061 (0.014) | 0.112 (0.067) | 0.609 | 0.017 (0.008) | 0.015 (0.006) | 0.935 |
| 2 | 0.246 (0.064) | 0.159 (0.057) | 0.348 | 0.159 (0.056) | 0.160 (0.028) | 0.992 | 0.007 (0.002) | 0.008 (0.002) | 0.930 |
| 3 | 0.117 (0.013) | 0.036 (0.008) | 0.059 | 0.077 (0.010) | 0.064 (0.013) | 0.787 | 0.003 (0.001) | 0.004 (0.002) | 0.972 |
| 4 | 0.357 (0.055) | 0.218 (0.019) | 0.143 | 0.144 (0.023) | 0.028 (0.003) | 0.061 | 0.006 (0.005) | 0.005 (0.001) | 0.975 |
| 5 | 0.250 (0.059) | 0.103 (0.018) | 0.092 | 0.054 (0.010) | 0.060 (0.010) | 0.882 | 0.009 (0.005) | 0.019 (0.022) | 0.845 |
| 6 | 0.147 (0.031) | 0.141 (0.055) | 0.933 | 0.056 (0.014) | 0.074 (0.014) | 0.703 | 0.009 (0.005) | 0.013 (0.005) | 0.894 |
| 7 | 0.250 (0.059) | 0.181 (0.023) | 0.478 | 0.061 (0.009) | 0.073 (0.012) | 0.770 | 0.040 (0.031) | 0.010 (0.006) | 0.613 |
| 8 | 0.116 (0.018) | 0.115 (0.016) | 0.986 | 0.054 (0.007) | 0.039 (0.005) | 0.653 | 0.007 (0.003) | 0.007 (0.003) | 0.990 |
Muscle electrical activity during the abduction-adduction movement
The RMS and the standard deviation values of the three muscles during the abduction-adduction movement are registered in Table 3. Although it was expected to find a significant difference among the muscles, the statistical analysis did not show a significant effect. The electrical activity of the trapezius muscle in subject one presented a significant statistical difference (p = 0.043). However, it could not be established a specific trend of the EMG behavior.
The results show the effect of the breast cancer surgery on the shoulder movement and the muscle electrical activity between the affected and non-affected side. There was a significant reduction of the range of motion (ROM) in the affected side in most of the patients for flexion-extension and abduction-adduction movements. These outcomes agree with other studies which have reported the reduction of the ROM during the first year after breast cancer surgery [10] [11] [14] [27] [29]. Furthermore, the reduction of the ROM could restraint the performance of some activities and then, have an impact on the quality of life of the patients [8] [9] [10] [26]. It has been mentioned that the scar tissue formation and protecting posturing after the breast cancer surgery could lead to shortening of the anterior chest wall. Therefore, the reduction of the ROM of the upper limbs found in this study could be related to the shortening of the breast chest [13] [16].
Some studies have found a significant reduction in the ROM of the upper limbs after breast cancer surgery using goniometry [8] [10] [17]. Our study used infrared cameras and provided more accuracy and a deeper analysis of the ROM of the shoulder joint in the sagittal and frontal planes. Although the markers and electrodes could produce discomfort to the participants, time and practice of movements were given to get used to the materials and perform the movements in a natural way. It has been reported that the mayor impairments in the upper limbs occur in the first or second year after the surgery. The development of the current study two months after the surgery allows us to identify the effects of the surgery on the kinematics of the shoulder in a short term. In a longer period of time, the effects of breast cancer surgery could be hidden due to the fact that the patients tend to adopt strategies and try to cope with the morbidities [10] [11].
The electrical activity of the muscles did not present a significant difference between the affected and non-affected side. Perhaps this could be produced due to the fact that the patients unconsciously try to elevate the upper limbs without too much effort. Furthermore, from the anthropometric data (Table 1), most of the participants were overweight or obese. We believe that overweight or obese participants will have different muscle electrical activity than the normal weight participants as the fat tissue could attenuate the EMG signal. This could be hidden the real effect of the muscle electrical activity when the affected and non-affected sides are compared. On the other hand, it has been suggested that humeral elevation of the arm, upward movement on the affected side, and left shoulder movement will increase the electrical activity of the muscles regardless of which side is affected [17]. Some studies have found significant difference in the EMG activity and muscle strength reduction after breast cancer surgery [19] [21] [30]. Although our study considers patients without pain, all of them were treated with coadjutant therapy (chemotherapy), which could have an effect on the electrical activity [18] [21]. Furthermore, it has been found that the EMG activity depends on parameters such as age, dominant hand, affected side, type of surgery, abnormal activation patterns and breast cancer treatment [17].
It has been recognized that exercise training part of the rehabilitation program will reduce the risk of breast cancer deaths in women who are physically active after breast cancer diagnosis [6]. Therefore, it is recommended to continue with the practice of physical therapy for improving the ROM of the affected side [6]. Although there are several studies related to the upper limb dysfunction after breast cancer surgery [4] [10] [11] [23], to the authors knowledge, this is the first study developed in the female Mexican population using infrared cameras and reflective markers. In addition, the results found in the study provide new knowledge to understand the impact of the breast cancer surgery on the upper limb dysfunction, so understanding the kinematics and electromyography of the upper limbs could help practitioners to improve patient education and influence treatment decisions [31].
The current study presents some limitations. First, the results cannot be generalized due to the sample size considered in the analysis. Second, some of the complications after mastectomy occur in a longer period of time, therefore, the results found in this study in the first two months could have a different effect beyond this date. Third, although different search engines were used to seek articles related to the research (google scholar, web of science and ScienceDirect), few works with conclusive information were found, making a comparison of the results difficult. However, although there are some limitations in the study, the results indicate a clear significant trend in the reduction of the ROM of the affected side after two months of the mastectomy, mainly when the arm is trying to reach the maximum elevation level. In future work, we expect to develop a study comparing the kinematics of the upper limbs before and after the surgical procedure. Furthermore, a sample of healthy participants without surgery but with similar demographic and anthropometric characteristics will be considered in the study.
CONCLUSIONS
The results suggest that the surgical procedure could compromise the range of motion of the affected side. This research contributes to clarify the effect of the surgical procedure in the ROM of the upper limbs after two months and provides new knowledge to understand the biomechanics of the upper limbs after mastectomy. Furthermore, from the results found in this study, it is reasonable that the patients with breast cancer surgery continue the rehabilitation program for a longer period of time.

