










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista mexicana de ingeniería biomédica
versión On-line ISSN 2395-9126versión impresa ISSN 0188-9532
Rev. mex. ing. bioméd vol.36 no.3 México sep./dic. 2015
https://doi.org/10.17488/RMIB.36.3.5
Nota técnica
Ambient Computing to Support the Association of Contextual Cues with Medication Taking
Cómputo Ambiental para Facilitar la Asociación de Pistas Contextuales con la Toma de Medicamentos
M.D. Rodríguez1, E. Zárate1, K. Stawarz2, J.P. García-Vázquez1, E.J.E. Ibarra1
1 Fac. de Ingeniería, Universidad Autónoma de Baja California, Mexicali, México.
2 University College London, U.K.
Correspondencia:
Marcela D. Rodríguez
Ave. Alvaro Obregón S/N Col. Nueva, C.P. 21100.
ónico: marcerod@uabc.edu.mx
Fecha de recepción: 12 de abril de 2015.
Fecha de aceptación: 31 de agosto de 2015.
ABSTRACT
The most common reason for non-adherence to medication among older adults is forgetfulness. Contextual cues, such as daily routines, serve as implicit situational information that increases the retrieval process of the intended action. The main contribution is an overview of the process and the technical details of Ambient Computing displays we developed to help seniors use contextual cues to remember actions associated with medication intake (i.e. remember to take medications or remember having taken them earlier). Through a qualitative study, we obtained evidence about the potential of our technological approach to make seniors more responsible and independent for taking medications.
Keywords: older adult, medication, ambient computing.
RESUMEN
Las razones más comunes para que adultos mayores no se apeguen a la medicación es el olvido. Las rutinas de vida diaria sirven como pistas contextuales que mejoran el proceso cognitivo relacionado con recordar realizar una acción planeada. Nuestro propósito es presentar el proceso de desarrollo, así como detalles técnicos, de Sistemas de Cómputo Ambiental que proveen pistas contextuales al adulto mayor para ayudarle a recordar acciones de su medicación (e.g., recordar medicarse o recordar que se medicaron). Mediante un estudio cualitativo, obtuvimos evidencia del potencial de nuestra tecnología para que el adulto mayor sea más responsable e independiente para medicarse.
Palabras clave: adulto mayor, medicación, cómputo ambiental.
INTRODUCTION
Approximately 50% of chronically ill older adults do not adhere to their prescribed medication regimens [1]. One of the most common reasons for non-adherence among older adults is forgetfulness, which has been associated with the fact that multiple cognitive processes are involved in remembering to follow a medication regimen [1,2]. Prospective memory is a crucial ability to support the functional independence of older adults, causing deficits on activities of daily living [3]. Insel et al [2] report that "older adults show substantial deficits when they rely on working memory and executive resources for prospective remembering, but minimal deficits when they rely on mostly preserved and relatively automatic associative retrieval processes". Our work is based on the fact that external cues support relatively automatic retrieval of the intended action [2]. Older adults are prone to use daily rhythms and routines as natural prompts for keeping track of their medications [4]. We will refer to these prompts as contextual cues, since they are used as implicit situational information that increases the retrieval process of the intended action (taking medications). Through an interview-based study, we identified common contextual cues that older adults use to prevent forgetting their medications. The results of this study informed the design of Ambient Computing displays that take into account the routine nature of older adults' lives.
Ambient Computing (AC) refers to an environment in which computing devices are seamlessly integrated into the users' environment to support their activities. The development of AC demands an interdisciplinary approach, borrowing methods and techniques from several Computer Science fields, such as Ubiquitous Computing and Human-Computer Interaction (HCI). Ubiquitous Computing refers to an environment saturated with heterogeneous computational and wireless communication devices aiming to provide information and services whenever users need them, in a proactive fashion. Furthermore, the services provided by the environment have to be accessible to diverse and non-specialist users through simple and natural means of interaction; thus, Human-Computer Interaction research is important in the AC field.
We have implemented AC displays that present useful and relevant information to the users in the intended setting. AC displays should be unobtrusive, unless they require the users' attention. Additionally, users should be able to easily monitor the display to obtain the desirable information [5]. To achieve it, AC displays use information representational modalities based on pictures, sounds, light and movement.
The methodology we followed for developing AC displays is based on User-Centered Design (UCD) [6], an approach to user interface development that involves users throughout an iterative process.
The main contribution of this technical note is an overview of the process we followed to develop AC displays that help older adults use contextual cues that support remembering medication intake (i.e. remember to take medications, or remember having taken them earlier).
In the next section, we describe the UCD stages followed when developing the AC displays. Next, in the Discussion section, we discuss the pros and cons of the technology that can be used to implement these systems; afterwards, we provide qualitative evidence about systems' utility and acceptance by older adults. Finally, we present our conclusions and future work.
METHOD
We followed the methodology illustrated in Figure 1, which is based on the User-Centered Design approach [6]. It consisted of the following stages:
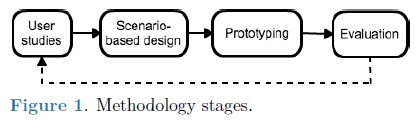
• User Studies: through interview-based studies with older adults, we have built an understanding of their needs and problems related to medicating, and the strategies they used to help them remember their medications. Based on the results, we were able to outline system requirements.
• Scenario based-design. This step consisted of providing stories that describe how seniors conduct medication related tasks ('persona scenarios'); how subjects will interact with our technological proposal (vision scenarios); and how the components of the implemented systems communicate with each other (application scenarios).
• Prototyping. We have implemented prototypes with different levels of fidelity such as paper mockups that depicted the main user interfaces' components and semi-functional prototypes [7].
• Evaluation. We conducted prototype evaluations with Usability Engineering and Geriatrics experts who identified usability problems and new systems requirements for improving the expected systems' utility [7].
As we present in this paper, our most recent user study and qualitative evaluation with potential users enabled us to understand how older adults use contextual cues that help them follow their medication routine.
User study
We conducted structured interviews with 87 older adults who attended day centers during weekdays and who take more than 3 medications every day. Interviews focused on understanding respondents' remembering strategies and situations in which they forget to take medications. The results showed that the main reasons for forgetting were being busy and distracted (40%), simple forgetfulness (37%), and changes in the routine (25%). We identified that for 31% of the participants it was important to take medications at specific hours. Most of the participants reported using contextual cues to help them remember, which we classified as:
• Daily routines. Participants took medications before sleep (56%) or in the morning after waking up (48%). Meal times also supported remembering: 28% of participants took medications after breakfast and 31% after lunch.
• Medications as reminders. Location of medications provided visual cues: i.e. 46% of the participants kept their medications by the bed and 44% in the kitchen (23% in a cabinet and 21% on a table). In addition, 24% of participants kept them in a bag (20 women) or a wallet (1 man). They used these locations because of easy access to medications and better memory support (41%), medications being at hand when needed (23%) and better visibility (14%).
• Alerts. Only five participants relied on their phone's alarm clock and three used a regular clock to remind medication (including one person who used both).
System requirements
The study reported in the previous section enabled us to understand how seniors select and use contextual cues that support their medication routines. The following persona scenarios depict actual situations of two of the interviewees:
Persona 1: Sonia, an 82 years old woman, takes 6 medicines daily for coping with diabetes, hypertension and glaucoma. She associates her medications intake with her daily routines (such as: waking up, after taking breakfast, and at night before going to bed). The only exception are her glaucoma eye drops as she needs help with applying them, therefore she uses them when her daughter visits her (event), which happens between 7:00 pm to 10:00 pm. When Sonia spends time socializing with her neighbors at night, she may go to bed later than usual, which may cause her to forget to take the insulin before 10:00 pm as prescribed by her doctor.
Persona 2: Pedro, a 69 years old man, takes 10 medications for controlling his blood pressure, the pain he feels due to his permanent physical trauma condition, and for coping with medications' side effects (digestive disorders). As he spends most of the day lying down on his bed, he maintains the medications on a bedside table (location). He follows a strict medication schedule, which he associates with daily routines. For instance, he takes enalapril and lozartan for blood pressure early in the morning (6:00 or 7:00 am), two hours before taking breakfast; along with the breakfast (8:00 or 9:00 am) he takes omeprazole for chronic digestive disease, and two hours later (10:00 or 11:00 am), the sulindaco to ameliorate pain. Sometimes, his wife reminds Pedro to medicate (event); but other times he asks her if he took medications, since he is afraid of forgetting them.
We have inserted tags in the previous persona scenarios, which emphasize the type of cues that these older adults reported to use: daily routines, location, and events. After illustrating the problem to address with persona scenarios, we specified the following system requirements (summarized in Table I):
• Provide older adults with notifications that help them learn how to create implementation intentions [23]. As proposed by Stawarz et al, it can be realized by apps that suggest pairing medication-taking with an existing routine [8].
• Augment medication location to provide visual cues. It supports retrieval of the action and may prevent elders from taking wrong medications.
• Help older adults create cues that enhance their awareness about whether the medication was taken as intended. The cue should be an action that makes the medication taking more salient and distinct, as it will make it easier to remember whether the medication was taken [9].
System design
To address the above-mentioned requirements, we decided to use three ambient modalities to represent information:
• auditory notifications to call the older adults attent ion when they have not taken the medication in a pre-established time window according to the medical prescription;
• pictograms-based notifications that encourage elders to irnplement their intention to take the correct medication doses when the contextual cue arises; i.e When [(condition], then [action][2, 23]. For instance, "When I have my orange juice with breakfast, I will take one pill of omeprazol".
• Light-based notifications to draw attention to the mediation containers whenever medications need to be taken.
To iniplement the requirements from Table I and the ambient modalities specified above, we designed Remind-Me and GUIDe-Me. Both are described below.
Remind-Me is an AC system for mobile devices to that provides auditory and pictogram-based notifications (see Figure 2). Pictograms represent critical information of the medication regimen: a) medication to take, b) the health problem addressed, c) the dose, and d) daily routines selected as contextual cues (e.g. Figure 2 shows that medication needs to be token after waking up and before going; to bed; additionally, it informs the user that the morning; dose has been taken).

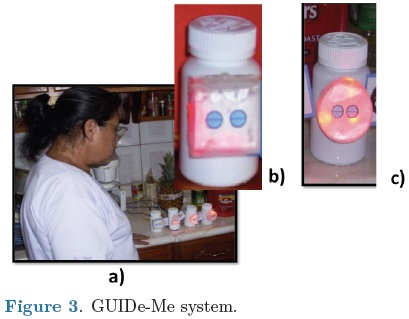
GUIDe-Me system (see Figure 3a) consists of a set of geometric user interfaces that display visual cues, which are attached to each medication container. The number of sides on each geometrical interface shows the number of times per day (frequency) that the medication has to be taken. The number of highlighted sides indicates the doses the user has to take. For example, Figure 3b shows a square with two sides illuminated to remind taking the second medicine dose of the day.
The following vision scenarios illustrates how AC systems may support the situations described in the persona scenarios:
Vision 1: At night, Sonia is visited by one of her friends. It is 10:00 pm. AOs the Remind-Me system has not been notified that Sonia has taken her insulin before going to sleep, it produces an auditory alarm and shows the pictogram illustrated in Figure 2. Sonia realizes that she still needs to take this medication before going to sleep.
Vision 2: While Pedro's wife is preparing breakfast, she asks him if he took the losartan pill. He is able to confirm that he did it, because he remembers moving the Remind-Me system closer to the losartan container, which deactivated the light of its geometrical user interface (GUIDe-Me) (see Figure 4).

System architecture
Figure 5 presents the architecture of Remind-Me and GUIDE-Me components, which are described) below.
Remind-Me. It includes the Prescription Manager sub-system with software components to tailor this system to users' needs. Through the Medication Manager and its Geometric User Interface (GUI Manager) we register the medication prescription and the images that will be used for the pictograms-based notifications.
The Reminder Manager sub-system comprises the software components to administer remainders (auditory and pictograms): the Reminder Aware Component accesses the local copy of the Medicines Information database to create the notifications to bee presented during thee day. Our design considers that a database replication can improve the performance and protect the availability of the medications information stored in a remote server. For example, in case of network inability, Remind-Me might normally access the local database rather than the remote server. This also improves the portability of the Remind-Me system, while enabling the remote managing of medications by members of the senior's fare network. For each medication, the Reminder Display creates a pictogram-based notification using pictures from the Images Repository; the Medication Taking Register updates the Medicine Information database to indicate if the medication was taken or not; and the Communication Unit is the component that informs the GUIDe-Me system which medications need to be taken (should be highlighted) or has been taken (should be de-highlighted).
GUIDe-Me system. Each geometric user interface is composed of a Processing Unit, a hardware component preprogrammed to light the geometrical user interface when it receives a notification of Remind-Me via its Communication Unit component. The geometrical user interface component represents the technology used for displaying light notifications.
System Implementation
To illustrate how the Remind-Me software components communicate (see Figure 6), we revisit the first vision scenario.
Sonia has a Remind-Me version for Android tablets. As presented in Figure 6, the Remind-Me Aware Component daily creates an instance of Alarm Manager class.
This is an Android class, which schedules the execution of the Remind-Me app based on the information stored on the local Medicines Information database. As Sonia has not taken the last dose of insulin before going to sleep(which should happen before 10:00 pm), the Alarm Manager object creates an instance of the Reminder Display class, which obtains the images (get Meditation Images()) necessary to create and present the pictogram-based notification through the display Reminder() method. After Sonia injects the insulin, she moves the mobile device closer to the insulin container. As depicted in Figure 4a, the container has attached a Near Field Communication (NFC) tag that is detected by the NFC reader of the Android tablet. This invokes methods to register that the insuline has been taken in the Medicines Information database (registerMedIntake()), and to turn off GUIDe-Me (deactivate()).
Figure 7 presents a photo of the electronic circuitry arranged for controlling a graphical user interface of GUIDe-Me. It uses a microcontroller preprogrammed with interrupt service routines (ISR) to highlight the sides of the geometric interface. Figure 8 shows the design of the electronic circuitry. In Figure 8a the Processing Unit is represented. It was implemented with the PIC16F877A, an 8-bit microcontroller that uses an arrangement of a pair of capacitors and an external crystal of 4MHz to regulate its work frequency. Additionally, the microcontroller has a push button and a resistance arrangement to have control over the microcontroller reset. The Graphical User Interface to Display cues (GUI-D) is composed of a set of light-emitting diodes (LEDs). Each LED has a diameter of 5mm and emits high intensity (8000 mcd) light (see Figure 8c). To illuminate each side of the geometric; interface, we used a pair of LEDs covered with a diffuser to ensure a proper light dissemination. Each LED is connected to a pin of the microcontroller output port (B-PORT) through 330 ohms resistances that limit the flow of current. Finally, Figure 8b illustrates that the main element of the Communication Unit is a RN-42 Bluetooth module, coupled to the microcontroller through a voltage divisor that processes Che logic voltage levels of the microcontroller. When the Communication Unit receives the instruction to deactivate the geometric user interface from the Remind-Me system (see Figure 6), it triggers the Interrupt Service Routine on the microcontroller to turn off the LEDs.

DISCUSSION
In this section we first discuss how we designed cost effective AC systems that may easily be modified to extend their functionalities. We mainly analyze the advantages and disadvantages of the hardware and software technologies that we used for implementing the systems. Afterwards, we compare our technological approach with related work reported in research literature and with commercially available technologies.
Mobile platforms
Remind-Me system was conceived for tablet devices, since they possess characteristics that may help seniors to easily interact with the system, such as the display size and its touch-based interaction.
The previous stage of the project was implemented for iOS devices, however, this platform limited sensing; capabilities for monitoring the medication intake. In contrast, using Android devices has enabled us to take advantage of their sensing and wireless communication capabilities, such as the Near Field Communication (NFC) technology. Remind-Me system was implemented by using the Eclipse IDE and Android Development Tools plugin that extends the IDE's capabilities to develop applications in Java [10]. Thus, Android provides an open programming platform, which facilitates interfacing mobile devices with other computing platforms, such as microcontrollers. This may enable us to upgrade the functionality of the GUIDe-Me prototype without requiring changing the main Remind-Me software components.
As the design of Remind-Me can be implemented for any mobile platform, it is important to analyze the advantages that other mobile devices impose over the platforms that we have already used, i.e. devices -with i OS and Android (US. In this sense, we identity that devices with Firefox OSS can be a viable alternative. It is a mobile operating system that is based on WEB APIs. feature that gives the advantage, over other mobile platforms, to develop applications that can communicate with the device's hardware and native functions, e.g. Bluetooth, Wi-Fi. Furthermore, Firefox OS is free from rules and restrictions of existing proprietary platforms such as iOS.
Compact electronic devices
Regarding the GUIDe-Me system, its implementation allowed us to prove our concept and test the capabilities of the selected electronic components and parts, as well as the integration of its three modules. However, there are several improvements that would account for a more stable, reliable and scalable system, providing developers with a broader range of choices for enhancing the performance of each of its modules:
Processing Unit (PU). We implemented this hardware component by using the PIC16F877A microcontroller [11], which requires additional circuitry and a voltage regulator for a stable voltage supply. At an average of $5 USD per unit, depending on package type and additional features, it represents a simple and cost effective solution. However, other commercially available options exist with more powerful characteristics, both in hardware and software, such as the Single board computers (SBC), which presents the characteristics summarized in Table II.
SBC are platforms that integrate all of the required components a computer needs for processing and controlling applications. Most recent SBCs are based on different microcontrollers and microprocessor architectures, including interfaces that allow developing applications in specific fields, such as Biometry. More important, some of the external circuitry that the microcontroller requires is already on board, which makes SBC more compact and robust. An important aspect in selecting a microcontroller or SBC for an application is to identify one that closely fits the requirements of the app; this allows developers to keep the whole system within specified constraints, such as budget, size and power consumption. In the case of GUIDe-Me, it is constrained by the small dimensions of the medicine containers, and the requirement for communicating wirelessly (through Bluetooth) with the app running in a mobile device (Remind-Me).
An alternative for implementing GUIDe-Me is using the IOIO-OTG board [12]. It is an SBC designed to allow implementation of hardware that connects to Android mobile devices and personal computers (PCs). IOIO-OTG is built around a PIC24FJ256 microcontroller, which is a 16-bit microcontroller that includes an 8MHz internal oscillator. This board allows applications to interface with external hardware using a high-level Java API, leveraging the integration of software and hardware, and hiding low-level details of microcontrollers I/O interface programming. The board can connect to an Android device by using a USB connector or a Bluetooth dongle, allowing control of external hardware from an application running on the Android device. It is powered by using a supply voltage between 5V and 15V that goes through one of the internal voltage regulators to remain at a stable and safe level. These regulators also allow the board to provide pins that interface to external devices working at either 5V or 3.3V, which avoids the need of additional circuitry for voltage conversion. The board's dimensions are 71x32mm; in case of using a USB Bluetooth dongle, the length increases by about 1cm.
A key factor in selecting a board is the community support behind it, which makes the Arduino board and its derivatives one of the most recommended choices [13]. Arduino was designed with an open hardware philosophy, with the reference designs published under a Creative Commons license. This has led to the creation of several derivatives, or community-designed boards based on Arduino, that share some features, while extending the original design or reducing its exposed interface in order to adapt it to specific applications. Similarly, the board capabilities are extended by means of stackable boards, called shields, which provide additional interfaces and functionality, such as motor driving, Ethernet connectivity, and reading from and writing to SD cards. The Arduino software is open source, which eases the addition of user-created libraries for the Arduino, its derivatives, and the several shields. The programming language has syntax similar to C.
The Arduino Pro Mini has one of the smallest form factors among the Arduino derivative boards. At 18x33mm and a weight under 2 grams, it is easy to embed in dimension-constrained applications.
This board is built upon the ATMega328 8-bit microcontroller and runs at 8Mhz; it is a low-voltage board, needing no external circuitry to interface with devices and modules using 3.3V. The board includes a voltage regulator that allows a power supply from 3.3V to 12V. Wireless communication can be achieved by interfacing a Bluetooth or WiFi module.
Another Arduino derivative with small form factor (35x18mm) is the Teensy LC board. This board features a 32-bit ARM Cortex-M0+ processor at 48MHz and has a total of 27 I/O pins, which provide interfaces similar to those in the Arduino Pro Mini.
An enhanced version of this board, the Teensy 3.1, maintains the same form factor of the Teensy LC, increasing most of its internal characteristics (speed, memory) in at least a factor of 2. While that increase would be unnecessary for the requirements of GUIDE-Me, this board features a real time clock (RTC), which could allow the geometrical user interfaces to keep track of time and work even without the interaction with the Android device.
The four boards previously described provide different characteristics that could help improve the current GUIDe-Me prototype. The IOIO board is an interesting fit, with the most available pins for interfacing with external hardware and a Java library that makes it easy to integrate in an Android application. Its major disadvantage lies in the logic of the system residing in the Android device, requiring it to be near the geometric user interfaces, or at least wirelessly connected, at all times to achieve the desired results. In addition, it has the largest form factor and highest cost of all the compared boards. Regarding the Arduino derivatives, their cost range from $9.95 (Arduino Pro Mini) to $19.95 US dollars (Teensy 3.1). The Arduino Pro Mini has the smallest form factor, though only 2mm shorter than the Teensy. The Teensy boards seem to be adequate fits for enhancing the current prototype, given their small form factor, more powerful and faster processors than the other boards and lower power supply requirements.
Geometrical User Interface to Display cues (GUI-D). An immediate improvement to GUI-D could be achieved by using addressable RGB LED strips [14], which are sets of connected RGB LEDs that are driven by a single digital pin of a microcontroller and individually selectable. A common LED density is 60 LEDs/m, which gives a separation of 1.65cm between LEDs; these strips are cut to the desired length and are flexible enough to shape them to project needs. A different choice could be the use of a dual color LED matrix [14]. This portrays an 8x8 matrix of LEDs where each position can be turned on or off individually. By means of these matrixes, the design of the geometrical interfaces could be changed to a logical shape instead of a physical one. The matrix would draw the geometrical shape that resembles the frequency of medication. A benefit of this would be a reutilization of the containers for different frequencies.
Communication Unit (CU). We opted for using Bluetooth communication between Remind-Me and GUIDe-Me systems. The RN-42 Bluetooth module [11] currently used in our GUIDe-Me prototype, is an adequate device that can be also easily integrated to Arduino-based systems. However, the IOIO-OTG board seems to be the most flexible for using Bluetooth communication, since it only requires a Bluetooth dongle connected to its USB port without requiring additional programming.
Feasibility study
We conducted a study to assess the feasibility of our approach. We implemented a prototype of the system design presented in Figure 5, to specifically evaluate two of the system's functionalities described in Table I:
a) Auditory notifications to call users attention, and the pictograms-based notifications to inform them about the medications to take. These notifications were presented through the Remind-Me system implemented for an Android tablet.
b) The generation of event-based cues to help elders to remember if they have taken their medications. This functionality was implemented by attaching NFC tags to each of the seniors' medication containers. Thus, elders have to approach the tablet and the medication container in order to generate an event cue.
Study design. A system was placed in the homes of two seniors to be used during 4 weeks. We decided to include seniors with Mild Cognitive Impairment (MCI), since they present a "cognitive decline greater than expected for an individual's age and education level, but which does not cause significant functional impairment" [15]. To recruit participants, we prepared a pamphlet describing the study, which was disseminated through social web sites. Eight relatives of interested participants contacted us. We visited them to assess potential subjects' eligibility by using the MMSE (Mini-Mental State Examination) to measure the elders' cognitive decline. Additionally, we interviewed them and their family caregivers in order to identify their deficiencies for medicating. The two seniors selected were those described in the persona scenarios earlier. They used the system during a month and received a weekly gift certificate ($500 pesos). We conducted a 40-minute training session for teaching the participants to use the system. Afterwards, we tailored Remind-Me system to the participants' medication regimens and placed it on a bedside table as they kept and took their medications in the bedroom. During the study, we conducted weekly in-home semi-structured interviews with caregivers and seniors. We asked them about any usage problems, which system's features they perceived as more useful and easy to use, and which ones they perceived as less useful and more difficult to use.
Perceived benefits. Even though participants experienced some technical and usability problems, they also reported the benefits of using the system. The problems were mainly associated with the medication registration functionality. Some NFCs stopped working during the first week (which were immediately replaced) and the font size of the medication registration messages was not appropriate (i.e. messages informing which medication was registered since its NFC tag was detected by the tablet).
The most useful functionality was the auditory reminder, and it was consistently reported as useful for the seniors throughout the study. Participants reported feeling more responsible and independent. For instance, Sonia's worry that she would miss the auditory notification when she was not near the tablet increased her focus on remembering medications. She reported to be more alert to the auditory reminders: " it has helped me a lot; before [using the system] I missed the times for taking medications... I did not hear some reminders during first week [of system usage], but now, I hear it even though I am in the kitchen" (reported in week 3). Thanks to the system, Pedro, who took several medications for pain relief, realized the importance of taking them with the frequency prescribed and not under-medicating (which may increase his pain) or overmedicating (which most worried him and his wife). Regarding this, Pedro reported: " Before [using the system] I used to skip the doctor instructions; now I listen to the system and I feel more supported" (reported in week 2). His wife complemented Pedro's comment by mentioning: "[the system] reminds him that he should not take his pills for pain relief before the auditory reminder... however, when the pain is very intense, then he does not wait for the reminder".
The system made caregivers feel less worried about the elders' medication compliance. Pedro's wife perceived that the system helped Pedro to reduce over-medication. She felt calmer, since the system encouraged Pedro to follow the medication schedule whenever his pain allowed it. Similarly, Sonia's daughter reported to feel more confident that her mother was forgetting less: " Now the system provides the times she [her mother] should medicate; and before, [using the system] my mother used to say: 'did I take it [a medication]?' Now she can check [in the system] if she took it". Sonia's daughter thought that her mother has improved her compliance to the glaucoma eye-drops, which was the main situation that worried her. Finally, she reported consulting the system once a day, every day: "If I don't check it in the morning, I check it in the afternoon; now I don't have to ask my mom about her medications".
Suggestions to improve system utility. We received several recommendations from the caregivers, which suggested that they envision new ways to deal with their caregiving burden:
• Providing historical reports of medication compliance. Caregivers wanted to be able to consult older adult's medication compliance of any day in the past (e.g. weekly reports).
• Reminding to execute daily routines relevant for elders' medication taking. Sonia's daughter suggested providing her mother with reminders for preparing meals at the lunchtime, as she needs to eat before taking the insulin.
Related work
As reported by Stawarz et al [8], available adherence technologies for mobile phones tend to focus on reminding users to take medications on time. Additionally, commercially available electronic pill containers and dispensers, such as Vitality Glow Caps [16], PivoTell [17] and Philips Medication Dispensing Service [18], have been designed to supply and dispense medications when necessary, freeing the patient from the burden of medication remembering. However, by focusing on reminders, these technologies reinforce the idea that users do not have to remember on their own and can rely on technology.
To the best of our knowledge, the situation is similar within research on Ambient Computing. Instead of providing reminders, the focus has been on using persuasive strategies to motivate older adults to follow their medication regimens. One example is MoviPill, a mobile phone app that gamifies the medication activity by awarding adherent users and promoting social competition [19]. Similarly, dwell Sense is an ambient display that shows representations of users' medication adherence to encourage reflection about their medication errors [20]. These ambient computing approaches neglect the habitual nature of daily routines, which become appropriate contextual cues when older adults learn to associate them to medication intake.
CONCLUSIONS
This technical note presents a description of the implementation of AC systems designed to help users form associations between contextual cues and medication taking. The main contribution is a description of the process we followed and technical details of AC systems that supports older adults' existing behavior, which can be used as guidelines for developing similar systems.
Our systems may be used to enhance interventions that have been proved to effectively address the common barriers to adherence, such as behavioral interventions, educational interventions and involvement of family caregivers [21]. Behavioral interventions are designed to change or influence a specific behavior and with this aim, we envisioned how the AC systems could support older adults by providing guidance related to taking correct medications and doses. Additionally, the involvement of family is relevant since family caregivers play an important role in patient medication adherence by reminding, monitoring and/or administering medication. However, studies suggest that large and complex medication regimens create hassle for family caregivers [22]. Therefore, providing older adults with the AC systems would help to reduce caregiving burden. Finally, educational interventions help patients to acquire the ability to self-medicate. In this sense, the AC displays can teach older adults to create and follow their implementation intentions, i.e. conceiving exactly when and where they will perform the intended action [23]. The principle to support is: 'when X arises, I'm going to perform Y' [2]. To reach this end, AC displays have to be tailored to older adults needs by taking into account their daily routines, specific tasks that may act as good contextual cues, prescribed medications regimens (e.g. medication frequency and doses), and type and characteristics of medications (e.g. pills, drops, shape and color of pills).
While tailoring may contribute to AC systems adoption, some medical-related factors can be barriers for adopting the systems [24]. First, decreased visual acuity and hearing of older adults may make it difficult for them to use some of the systems' functions. For example, they may not be able to read prescription labels or differentiate the tablet colors presented in the pictograms. Secondly, as cognitive decline progresses, they may not be able to autonomously use the systems. However, AC systems could support caregivers to provide elderly with External Memory Aids (EMA), which is an intervention recommended for coping with demented patients' disorientation, repetitive questioning, and apathy for carrying out activities of daily living, such as taking medications [25].
This technical note presents results that enabled us design Remind-Me and GUIDe-Me, and to illustrate how their features can help older adults remember to take medications. Our feasibility study provides preliminary evidence of the potential of our approach and that it could be useful and accepted by older adults. Participants' overall experiences were consistently positive, even though some technical and usability issues were also reported. Their responses indicated that they appreciated the potential of this technology to make older adults more independent and responsible for taking their medications. Additionally, caregivers reported how the systems may enable them to heighten their peace of mind.
As a future work we plan to evaluate the effectiveness of the AC displays to support older adults' medication adherence and to reduce caregiver burden. We plan to recruit 20 senior-caregiver dyads (10 for using the ambient display and 10 for the control group), who will be monitored during four months (including pre-intervention and intervention phases). To overcome the difficulties of recruiting participants, we will conduct this evaluation by collaborating with the Nursing School of the UABC University. Additionally, nursing students will make weekly visits to assess the elders' medication adherence (pills counting), their self-efficacy for medicating and the family caregivers' burden.
Nevertheless, even though further evaluation is planned, the design process and the results of the feasibility study show that it is possible to design adherence technologies that support contextual cues and existing daily routines.
ACKNOWLEDGEMENTS
We would like to thank UABC and CONACYT (no. 153863) for the funding provided to conduct this project, and the scholarship provided to the fourth author. We also thank to the students who helped conducting the study interviews and the older adults who participated in it.
REFERENCES
1. Murray, M. D., Morrow, D. G., Weiner, M., Tu, W., Deer, M. M., Brater, D. C., & Weinberger, M. "A conceptual framework to study medication adherence in older adults". The American Journal of Geriatric Pharmacotherapy, vol. 2, no 1, pp. 36-43, 2004. [ Links ]
2. Insel, K. C., Einstein, G. O., Morrow, D. G., & Hepworth, J. T. "A multifaceted prospective memory intervention to improve medication adherence: Design of a randomized control trial". Contemporary Clinical Trials, vol. 34, no. 1, pp. 45-52, 2013. [ Links ]
3. Smith, G., Della Sala, S., Logie, R.H., & Maylor, E.A. "Prospective and retrospective memory in normal ageing and dementia: A questionnaire study". Memory, vol. 8, pp. 311-321, 2000. [ Links ]
4. Palen, L. and S. Aaløkke. "Of pill boxes and piano benches: 'home-made' methods for managing medication". In ACM Proc. of the SIGCHI Conf. on Computer Supported Collaborative Work, Banff, Canada, pp. 79-88, Nov. 2006. [ Links ]
5. Mankoff, J., Dey, A.K., Hsieh, G., Kientz, J., Lederer, S., and Ames, M. Heuristic evaluation of ambient displays. In Proc. of the SIGCHI Conference on Human Factors in Computing Systems (CHI '03). ACM, New York, USA, pp. 169-176, 2003. [ Links ]
6. Hix, D., & Hartson, H. R. "Developing user interfaces: ensuring usability through product & process". John Wiley & Sons, Inc., 1993. [ Links ]
7. García-Vázquez, J.P., Rodriguez, M. D., Andrade, A.G., Bravo, J. "Supporting the Strategies to Improve Elders' Medication Compliance by Providing Ambient Aids". Pers Ubiquit Comput, vol. 15, no. 4, pp. 389-397, 2011. [ Links ]
8. Stawarz, K., Cox, A.L., and Blandford, A. "Don't forget your pill!: designing effective medication reminder apps that support users' daily routines". In Proc. of the SIGCHI Conference on Human Factors in Computing Systems (CHI '14). ACM, New York, NY, USA, pp. 2269-2278, 2014 [ Links ]
9. McDaniel MA, et al. "Repetition errors in habitual prospective memory: elimination of age differences via complex actions or appropriate resource allocation". Aging Neuropsychol Cogn, vol. 16, no. 5, pp. 563-88, 2009. [ Links ]
10. ADT Plugin Release Notes (n.d.) Retrieved from: http://developer.androidcom/tools/sdk/eclipse-adt.html
12. IOIO Microcontroller (n.d.). Retrieved from: https://github.com/ytai/ioio/wiki
13. Android (n.d.) Retrieved from: http://www.arduino.cc/
14. https://www.sparkfun.com/products/
15. Thompson, C., Henry, J.D., Rendell, P.G., Withall, A., Brodaty, H.: Prospective memory function in mild cognitive impairment and early dementia. J Int Neuropsychol Soc., vol. 16, pp. 318-325, 2010. [ Links ]
16. Vitality. (n.d.). Glow Caps., Retrieved from: http://www.glowcaps.com/
17. PivoTell. (n.d.). PivoTell Automatic Pill Dispenser Mk 3-11. Retrieved from: http://www.pivotell.co.uk/
18. Philips. (n.d.). Philips Medication Dispensing Service. Retrieved from: http://www.managemypills.com/content/home
19. Oliveira, R., Cherubini, M., & Oliver, N. "MoviPill: improving medication compliance for elders using a mobile persuasive social game". In Proc. of the 12th ACM international conference on Ubiquitous Computing - Ubicomp '10, New York, New York, USA: ACM Press, pp. 251-260, 2010. [ Links ]
20. Lee, M., & Dey, A. "Real-time feedback for improving medication taking". In CHI 14 Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, pp. 2259-2268, 2014. [ Links ]
21. Steinman, M. A.; Hanlon, J. T. Managing medications in clinically complex elders: "There's got to be a happy medium". JAMA, vol. 304, no 14, pp. 1592-1601, 2010. [ Links ]
22. O'Quin, K. E., Semalulu, T., & Orom, H. Elder and caregiver solutions to improve medication adherence. Health Education Research, cyv009, 2015. [ Links ]
23. Gollwitzer, P. Implementation Intentions: "Strong Effects of Simple Plans". American Psychologist, vol. 54, no. 7, pp. 493-503, 1999. [ Links ]
24. MacLaughlin, E. J., Raehl, C. L., Treadway, A. K., Sterling, T. L., Zoller, D. P., & Bond, C. A. Assessing medication adherence in the elderly. Drugs & Aging, vol. 22, no. 3, pp. 231-255, 2005. [ Links ]
25. Navarro, R.F., Rodriguez, M.D., and Favela, J. "Intervention tailoring in augmented cognition systems for elders with dementia." Biomedical and Health Informatics, IEEE Journal, vol. 18, no. 1, pp. 361-367, 2014. [ Links ]

