










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista mexicana de ingeniería biomédica
versión On-line ISSN 2395-9126versión impresa ISSN 0188-9532
Rev. mex. ing. bioméd vol.35 no.1 México abr. 2014
Artículo de investigación original
Amplitude Modulation Approach for Real-Time Algorithms of ECG-Derived Respiration
Desarrollo de Algoritmos en Tiempo Real para Derivar la Respiración del ECG Bajo el Criterio de Amplitud Modulada
J.L. Vargas-Luna*,** W. Mayr** J.A. Cortés-Ramírez*
*Centro de Innovación en Diseño y Tecnología, Tecnológico de Monterrey, Campus Monterrey, México.
**Center for Medical Physics and Biomedical Engineering, Medical University of Vienna, Austria.
Correspondencia:
J.L. Vargas Luna
Ave. Eugenio Garza Sada 2501
Sur Col. Tecnológico C.P. 64849
Correo electrónico: joseluis.vargasluna@gmail.com
Fecha de recepción:23 de Noviembre de 2013.
Fecha de aceptación: 24 de Marzo de 2014.
ABSTRACT
This work presents the development of an ECG-Derived Respiration (EDR) methodology based on the amplitude modulation approach. It allows to redefine actual methodologies in order to obtain a continuous EDR signals with high correlations and small delay between EDR and respiration activity. Two algorithms are implemented: one of them using the amplitude modulation of the R-peak (EDRAM) and another one applying a band-pass filter in the bandwidth of respiration. Unlike other techniques in literature, conventional low order filters are applied without sacrifice of correlation factor (0.76 and 0.67) and a minimum delay of 0.27s (with EDRAM) in a ∼6s cycle. A robustness test was performed, and it shows a noise tolerance of up to 20% of the maximum value before its correlation factor drops considerably. The application into a wearable sensor was successfully implemented. The two methodologies proposed show advantages like real-time processing and robustness under certain noises. The proposed AM perspective supports the use of both algorithms for typical applications with high efficiency, low computational cost and ease of implementation. These characteristics result on a technique that facilitates the development of wearable systems, and to increase the information of actual databases.
Keywords: amplitude modulation, ECG, EDR, respiration, real time.
RESUMEN
Este trabajo presenta una metodología para la extracción de la actividad respiratoria derivada de un ECG (EDR, por sus siglas en ingles), basado en el enfoque de amplitud modulada (AM). Esto permite redefinir las metodologías actuales para obtener una señal EDR más continua, con altos factores de correlación y un retraso menor entre la EDR y la actividad respiratoria. Se implementaron dos algoritmos: uno utilizando la modulación de la amplitud del pico R (EDRAM) y el otro aplicando un filtro paso-banda en el espectro de frecuencia de la respiración. A diferencia de otros trabajos en la literatura, se utilizan filtros convencionales de bajo orden pero sin sacrificar el factor de correlación (0.76 y 0.67) y manteniendo un retardo de ∼0.27s (con EDRAM) en un ciclo de ∼6s. Se realizó una prueba de robustez, donde se muestra una tolerancia a ruido blanco de hasta un 20% del valor máximo antes de que el factor de correlación bajara considerablemente. El algoritmo EDRAM se aplicó con éxito en un prototipo de sistema portable. Las dos metodologías propuestas muestran ventajas como el procesamiento en tiempo real y robustez bajo ciertos ruidos. La perspectiva de AM propuesta soporta el uso de ambos algoritmos para aplicaciones típicas con alta eficiencia, bajo costo computacional y facilidad de implementación. Estas características hacen que esta técnica facilite el desarrollo de sistemas portátiles, así como para incrementar la información de las bases de datos actuales.
Palabras clave: amplitud modulada, ECG, EDR, respiración, tiempo real.
INTRODUCTION
The respiratory activity is an important clinical parameter that is not commonly monitored. Many techniques have been developed to measure the respiration activity directly, e.g. nasal temperature, airflow, chest impedance, body-volume change, among others. Some indirect methods are Electrocardiography (ECG) Derived Respiration (EDR), Blood Pressure Derived Respiration (BPDR), and Photoplethysmography Derived Respiration (PDR) [1]. With indirect methods, software of conventional ECG, BP or PPG monitors can be updated to achieve the respiration monitoring without any hardware adjustment.
The most studied indirect method to monitor respiratory activity is the EDR, because the ECG is commonly monitored [1-9].
The EDR techniques are based on three facts: 1) the relative position of the heart to the electrodes changes during respiration, what increases/decreases the distance of the ECG source to the electrodes [3]; 2) the thoracic impedance varies with the airflow in the lungs, which changes the medium’s resistivity that signal must cross to reach the electrodes [3,10] and; 3) the mean electrical axis of the cardiac vector changes its direction during respiration [10,11]. These facts induce an amplitude modulation (AM) of the ECG amplitude detected at the electrodes.
Many approaches have been proposed for EDR calculation [12]. Among them are the R-peak amplitude [6], RS-peak's amplitude difference, QRS area [5,13], and filtered ECG. Some mathematical tools have also been used as principal component analysis[10,14], wavelet transformations [9,10], adaptive filters [2], special ECG-geometry features [8] and other statistical tools [3].
The most popular EDR techniques are those related to the QRS complex features. However, all these techniques are very sensitive to baseline wander. Recent research that use these approaches focused, most of the work, in an effective baseline-wander removal technique, in order to clean the ECG without affecting the frequency properties of the signal [1,3,6].
Some common principles used to generate an EDR signal are [12]:
Band-pass filtered ECG: Using this principle it is possible to generate an EDR signal from band-passing the ECG in the bandwidth of respiratory activity (0.15-0.8Hz or 9-48bpm) [11,15,16]. The main disadvantage is that it is sensitive to baseline noises, because target frequencies overlap with noise sources that produce the baseline drift. Consequently, it is necessary to include an effective baseline wander removal with non-conventional filters.
R-peak amplitudes: In this principle, the amplitude variations of the R-peaks, induced by respiratory activity, are detected. These points are used as discrete samples of the EDR, and a signal reconstruction is computed based on them. As mentioned before, this technique is very sensitive to noise although R-peak has a big Signal-to-Noise ratio (SNR) [3].
RS-peak's amplitude difference: This principle uses the detected R-peaks, S-peaks, and their amplitude differences. Such differences are then used as discrete samples for a signal reconstruction. With the use of two points, slightly more computation is needed, but more robustness to baseline wander noise may be achieved.
QRS area: This principle uses the detected Q-, R-and S-peaks. Based on such points, a triangle is generated for each QRS complex and its area is quantified. For this method, those areas are the discrete samples used for the signal reconstruction. With the use of three points, more computation is needed, but more robustness to baseline wander noise may be obtained [13]. However, it is important to mention that Q-and S-peaks have a low SNR. Therefore, these are harder to identify, what introduces other error sources.
From all the methods mentioned above, only the band-pass filtered ECG allows a continuous monitoring of the respiratory activity, while others have relatively long and non-constant sampling periods (one per heart beat). Considering the fact that high respiratory activity imply high heart rates, as well as own observations in conventional measurements, it is possible to assume that there are more than two heartbeats per respiratory phase (unless the respiratory rate is increased intentionally). This means that Nyquist's frequency is achieved and, therefore, respiratory phase and rate can be monitored.
Although the EDR is not a new technique, the technological trend to develop wearable systems has renewed the interest for methodologies that allow the reduction of signal processing, hardware and energy requirements for multiple signal acquisition [10]. The huge databases freely available, like PhysioNet [17], are also a core application for the EDR, since it may provide additional information if ECG is present. It is also important for applications where a reduced number of sensors is valued, like sleep studies [18], measurements on children or patients with neurological impairment [19].
This work is focused on the development of an EDR algorithm based on the AM of the ECG caused by the respiratory activity. The main objective is generating an EDR signal with an output frequency of at least 1Hz, a correlation factor bigger than 0.4 and a minimal delay between the EDR and the actual respiration.
METHODOLOGY
For the development of this work, the mathematical approach of the Amplitude Modulation of ECG is initially presented. Two algorithms are defined as suitable continuous and small delay EDR methods, one related with the R-peak amplitude (EDRAM) and another with the band-pass filtering of ECG (EDRBP). A quantitative comparison is made with other algorithms. A statistical evaluation of robustness is also done to the proposed algorithms. Finally, the EDRAM is also test with raw data obtained from a wearable system.
Mathematical Approach
An electrical signal can be expressed as the sum of all of its electrical components. The signals that compose the acquired ECG can be mainly categorized as: pure ECG signal (y), power line noise (npl), higher frequency noises (nh), white noise (nw) and the baseline wander noises (nbl).

Where t stands for time. It is important to notice that Eq. (1) does not express the existence of the EDR because it is not an electrical component but a modulation effect over the ECG. Table 1, describes the source and bandwidth of each of the components in Eq. (1).
The AM is a technique used in telecommunication, which sends a desired signal (e.g., EDR) over a carrier signal of higher frequency (e.g., ECG). In the case of the respiration, the physio-anatomical structure of the body induces this modulation naturally. It is necessary to keep in mind that the ECG is not a unique-frequency signal, but it has frequency components along the bandwidth of 0.67-300Hz [20,21]. Without loss of generality, y(t) is decomposed into a Fourier series and, because the respiration activity is express along the whole spectrum of the carrier signal, only one component is taken (e.g., 10Hz). Such component corresponds to a frequency considerably higher (>10) than respiratory rate (up to 0.8Hz). In addition, if the respiration is assumed as a constant sinusoidal signal, then the amplitude modulated ECG can be expressed as follows [22]:

Where yEDR is the respiration signal, yECG is the carrier signal, y the modulated signal, m the modulation index (AEDR∕AECG), and xn the modulation signal [22]. The main effect of the AM is bandwidth displacement of the low frequency signal into the frequency ωECGt. Since our carrier signal is the ECG, then the EDR bandwidth is extended to the same frequency range of ECG.
Proposed algorithms ECG-Derived Respiration based on AM (EDRAM)
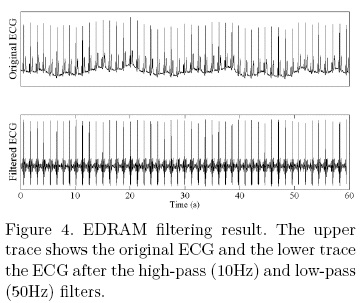
Considering the AM caused by the respiration over the ECG, it is possible to assume that the respiratory signal is reflected not only in the bandwidth of respiration (0.2-0.8Hz) but also over the spectrum of the ECG. Based on this, it is possible isolate the y and nw components in Eq. (1) using a 2nd order Butterworth low-pass filter (fc=50Hz) - to remove nh and partially npl - and a high-pass filter (fc=10Hz) - to remove nbl. Notice that the use of such filters also removes important components of the ECG signal. It causes that the QRS complex is no longer present, and only a modified R-peak can be detected.
The method for AM demodulation is the contour detection. Because the filtered ECG modulation signal [6,7]. The R-peak detection is achieved based on the stereotypical shape of the QRS complex, where the R-peak is: a local maximum, over a threshold and, sharply pointed (signal falls near 0V in ±20ms).
Once the discrete samples are acquired, they can be directly used for control or processing purposes or, if a visual feedback is necessary for patient or medical staff, a reconstruction algorithm could be implemented. For this report, a moving average, with a span length of the 25% of the sampling frequency, is applied offline, in order to generate a smooth visual representation.
Many algorithms are found in literature, but when a multi-lead ECG is not used, an accurate estimation of the ECG's baseline must be done because the EDR bandwidth overlaps with the one of the nbl [3,5,6,10]. But considering the AM effect, it is possible to filter this noise with a conventional 2nd order Butterworth high-pass filter.
EDR based on Band-Pass filtering (EDRBP)
A second algorithm is implemented with the conventional approach, where the spectral components of the EDR are taken directly from the ECG signal with a Band-Pass filter (EDRBP).
Under this basis, it is possible to assume that a band-pass filter, with the same spectrum of respiratory activity (0.2-0.8Hz), will almost isolate the modulation signal (xn) [15,16]. In this case a FIR filter of 64th order is implemented with a bandwidth of 0.2-0.4Hz.
The filter described above eliminates most of the noises mentioned in Table 1, except for partial baseline wander and white noise. The last one can be neglected since its uniform probability distribution make that the probability of noise affecting the bandwidth of 0.2-0.4Hz tend to 0 because of its infinite nature.
However, the noise of the baseline wander interferes with the respiration bandwidth. This is shown in Fig. 1, where the output of the band-pass filter basically describes nbl. A postprocessing stage, based on the derivative of the signal, is necessary to unmask the respiratory activity embedded on it.

Test and Comparison
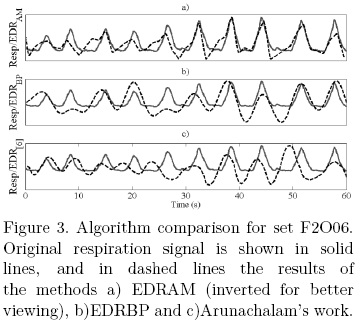
For test the algorithms, the Fantasia data set of the PhysioNet/PhysioBank is used [17,23]. This set contains ECG and respiratory (chest belt [6]) data of young and elderly people at rest in supine position. The data are acquired at 250S/s [23]. A quantitative comparison is done using the Pearson correlation coefficient (r) to measure the level of correlation and delay between the respiration and the computed EDR. The delay is calculated as the value in which the correlation coefficient reach its maximum level [24]. From the comparison, the files F2Y10 (segment from 00:20-01:20) and F2O06 (segment from 01:00-02:00) are shown because of their significant baseline drift [6]. The proposed algorithms are compared with others found in literature [6,10,25]. Specifically, the one proposed by Arunachalam and Brown is shown graphically, because it is developed directly for real time implementations, uses a single-lead ECG, employs similar algorithms to others found in literature [9,10,25], and it is tested with freely available databases, what allows us to make a direct comparison.
Evaluation
In order to test the robustness of the proposed algorithms, white noise is induced at percentage levels of 0, 1, 10, 25, 50, 75, 90, 99 and 100% relative to the maximum ECG value. The correlation test is used as a parameter to measure the degradation of the performance of each algorithm with the induction of noise. 500 iterations are used to obtain the mean value of the correlation test, preventing in this way a false parameter due the randomness of the induced noise.
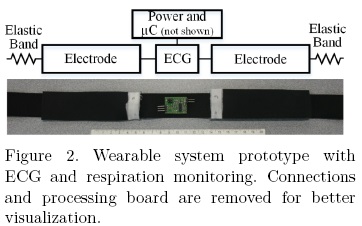
The viability of the algorithm to be implemented into new developments is evaluated with in-house measurements. For this purpose, a ground-free ECG is developed based on the work of Dobrev et al. [26]. The design is selected for its simplicity and its potential to be embedded into a wearable system. As shown in Fig. 2, the system is mounted into a custom-made prototype of a chest belt sensor, with two embedded conductive-rubber electrodes (Schuhfried Medizintechnik, Austria) of 11 × 3.5cm each (cross-resistance of 90Ω). No conductive solution is applied during acquisition. Raw data is acquired at 1kS/s with MATLABTM (Mathworks, Inc., USA). Although, the raw data of the device is not optimal due electromagnetic interference and baseline wander, the data is adequate to evaluate the EDR algorithms.
RESULTS AND DISCUSSION
The algorithms are implemented in MATLABTM (Mathworks, Inc., USA).
The results for set F2O06 are shown in Figs. 3 and 4. The first one shows a visual comparison of the respiration and the EDR calculated by the two methodologies proposed and the reconstruction of the results presented in [6]. Fig. 4 shows the results of the filtering process for the EDRAM method. Fig. 5 shows the visual comparison for the set F2Y10.

In both sets, the EDR signal preservation, despite the implementation of high-pass filters, is consistent with the proposed mathematical approach. It confirms that typical filters can be implemented for baseline noise removal without losing respiratory data.
The comparison of the correlation test is shown in Table 2, for both sets. It is shown that both algorithms show a bigger correlation and better synchronization (except EDRBP on F2Y10) than other real-time algorithms [6], although simple filters are used. EDRAM also reaches similar correlation factors than some offline methodologies that range between 0.66-0.80 [10, 25].

It is important to notice that respiratory signal is acquired with a respiration-belt[6], and such signal is not in phase with the actual respiration (airflow). Control measurements done in-house, show that thoracic-belt-based measurements are 1s (for a 3s respiratory cycle) anticipated at the spirometer-based measurements. Therefore, although specific details of the sensors used are not available, it is reasonable to assume that delay values in Table 2 may be smaller when compared with actual respiration.
The evaluation of robustness is presented in Fig. 6, which shows how each algorithm decreases its efficiency when white noise is induced at different levels.

The EDRAM shows significantly better results when the original ECG is used. But, when white noise is induced, the correlation falls because the signal-to-noise ratio decreases rapidly. Fig. 6 gives a guideline for choosing the correct algorithm for a specific need. The EDRAM shows stability for values of wide spectrum noises under 15% (of the maximum ECG value). But, for situations where wide spectrum noise suppression can't be guaranteed, then the EDRBP becomes the better option.
The implementation of the algorithm into a ground-free ECG is presented in Fig. 7. Because of the big baseline noise levels presented by the wearable system prototype, the EDRAM is selected due its capabilities mentioned before. Fig. 7 shows that the algorithm is able to deal with high baseline and electromagnetic (50Hz) noise.

For this evaluation the EDRBP shows instability on when non-natural respiration and baseline wander are present. However, this method seems to be more efficient for real-time. This is because it is obtained by a series of conventional FIR filters, and it is possible to get measurements in every sampling period. This provides a contrast with other methods that only obtain one sample per heartbeat.
CONCLUSIONS
A mathematical amplitude modulation approach is presented for EDR calculation. This approach claims that although the respiration information is essentially conformed by a low frequency signal; it is also contained in higher frequencies due the AM of the ECG. This way, it is possible to apply conventional low-order high-pass filters and still be able to generate an EDR signal from the demodulation of ECG's higher frequencies. Two different algorithms are implemented, tested against white noise and compared with other methods found in literature. The EDRAM shows a correlation factor up to 0.76 and the EDRBP up to 0.67.
The output frequency of the EDRAM is not controllable, since it depends on the cardiac frequency. However, at low heart rates, the respiration can be considered also slower, so these are enough to detect the respiratory phase and rate.
The EDRAM algorithm is faster than other techniques found in literature, since the EDR sample can be extracted directly from the last QRS complex. This, unlike other real-time algorithms that first use a batch of complexes or samples to extract the baseline drift and, after that, acquire the EDR sample [6,9]. The delay of the EDR signal in relation to the respiration results smaller when compared with others methods. Also, the AM approach allows the construction of less computation-effort algorithms with similar or better results than the ones currently used.
The EDRAM also proof its potential to be implemented in embedded wearable systems. Currently, its performance in long-term measurements (during sleep and daily activity) is under study.
The algorithms have shown that can be implemented to generate additional data from actual databases. In addition, the proposed AM perspective supports the use of both algorithms for typical applications with high efficiency, low computational cost and ease of implementation. These characteristics make this technique useful for the development of wearable systems because, if ECG is monitored, no additional sensors are required, which implies less instrumentation, energy consumption and discomfort to the patient.
REFERENCES
1. Travaglini A, Lamberti C, DeBie J, Ferri M. Respiratory signal derived from eight-lead ECG. Comput. Cardiol. 1998. Cleveland, USA: IEEE; 1998. p. 65-8. [ Links ]
2. Varanini M, Emdin M, Allegri F, Raciti M, Conforti F, Macerata A, et al. Adaptive filtering of ECG signal for deriving respiratory activity. Comput. Cardiol. 1990. Chicago, USA: IEEE Comput. Soc. Press; 1990. p. 621-4. [ Links ]
3. Ding S, Zhu X, Chen W, Wei D. Derivation of respiratory signal from single-channel ECGs based on Source Statistics. Int. J. Bioelectromagn. 2004;6. [ Links ]
4. Madhav KV, Ram MR, Krishna EH, Komalla NR, Reddy KA. Estimation of respiration rate from ECG, BP and PPG signals using empirical mode decomposition. Instrum. Meas. Technol. Conf. 2011. Binjiang, China: IEEE; 2011. p. 1-4. [ Links ]
5. Moody GB, Mark RG, Zoccola A, Mantero S. Derivation of Respiratory Signals from Multi-lead ECGs. Comput. Cardiol. 1985. Washington, DC: IEEE Computer Society Press; 1985. p. 113-6. [ Links ]
6. Arunachalam SP, Brown LF. Real-time estimation of the ECG-derived respiration (EDR) signal using a new algorithm for baseline wander noise removal. Eng. Med. Biol. Soc. 2009. EMBC 2009. Annu. Int. Conf. IEEE. Minneapolis, USA: IEEE; 2009. p. 5681-4. [ Links ]
7. O'Brien C, Heneghan C. A comparison of algorithms for estimation of a respiratory signal from the surface electrocardiogram. Comput. Biol. Med. 2007;37:305-14. [ Links ]
8. Lazaro J, Alcaine A, Gil E, Laguna P, Bailon R. Electrocardiogram derived respiration from QRS slopes. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2013;2013:3913-6. [ Links ]
9. Ramya K, Rajkumar K. Respiration Rate Diagnosis Using Single Lead ECG in Real Time. Glob. J. Med. Res. 2013;13:7-12. [ Links ]
10. Langley P, Bowers EJ, Murray A. Principal component analysis as a tool for analyzing beat-to-beat changes in ECG features: application to ECG-derived respiration. IEEE Trans. Biomed. Eng. 2010;57:821-9. [ Links ]
11. Zhao L, Reisman S, Findley T. Respiration derived from the electrocardiogram during heart rate variability studies. Proc. 16th Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. Baltimore, USA: IEEE; 1994. p. 123-4. [ Links ]
12. Widjaja D, Taelman J, Vandeput S. ECG-derived respiration: Comparison and new measures for respiratory variability. Comput. Cardiol. 2010. Belfast, Northern Ireland: IEEE; 2010. p. 149-52. [ Links ]
13. Mazzanti B, Lamberti C, de Bie J. Validation of an ECG-derived respiration monitoring method. Comput. Cardiol. 2003. Thessaloniki, Greece: IEEE; 2003. p. 613-6. [ Links ]
14. Pflugradt M, Mann S, Feller V, Orglmeister R. On-line Learning Algorithms for extracting respiratory activity from Single Lead ECGs based on Principal Component Analysis. Biomed. Tech. (Berl). 2012;57:352-4. [ Links ]
15. Boyle J, Bidargaddi N, Sarela A, Karunanithi M. Automatic detection of respiration rate from ambulatory single-lead ECG. IEEE Trans. Inf. Technol. Biomed. 2009;13:890-6. [ Links ]
16. Guyton AC, Hall JE. Tratado de Fisiología Médica. 12a ed. ELSEVIER, editor. 2011. [ Links ]
17. Goldberger A, Amaral L, Glass L. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation. 2000. [ Links ]
18. Babaeizadeh S, Zhou SH, Pittman SD, White DP. Electrocardiogram-derived respiration in screening of sleep-disordered breathing. J. Electrocardiol. 2011;44:700-6. [ Links ]
19. Moussavi ZK, Leopando MT, Pasterkamp H, Rempel G. Computerised acoustical respiratory phase detection without airflow measurement. Med. Biol. Eng. Compu. 2000;38:198-203. [ Links ]
20. Prutchi D, Norris M. Design and Development of Medical Electronic Instrumentation. Hoboken, NJ, USA: John Wiley & Sons, Inc.; 2005. [ Links ]
21. Company-Bosch E, Hartmann E. ECG Front-End Design is Simplified with MicroConverter. Analog Dialogue. 2003;37:1-5. [ Links ]
22. Godse AP, Bakshi UA. Communication Engineering. Technical Publications; 2009. [ Links ]
23. Iyengar N, Peng CK, Morin R, Goldberger a L, Lipsitz L a. Age-related alterations in the fractal scaling of cardiac interbeat interval dynamics. Am. J. Physiol. 1996;271:R1078-84. [ Links ]
24. Pereda E, Quiroga RQ, Bhattacharya J. Nonlinear multivariate analysis of neurophysiological signals. Prog. Neurobiol. 2005;77:1-37. [ Links ]
25. Anand S, Sanjay H, Suraj K, Krishnaswamy U. ECG-Derived respiration as a Screening Tool for OSA. Indian J. Sleep Med. 2012;7:94. [ Links ]
26. Dobrev D, Neycheva T, Mudrov N. Simple two-electrode biosignal amplifier. Med. Biol. Eng. Comput. 2005;43:725-30. [ Links ]

