











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Cardiac tumors are either primary or secondary. Primary tumors are infrequent, with an estimated incidence of 0.001% to 0.03%; approximately three fourths are benign and the remaining malignant.1 The cardiac myxoma is the most frequent amongst the benign, approximately in 50%;1 although in some series, the papillary fibroelastoma is reported as being the most common.2 Less frequently the lipomas and rhabdomyomas can be found.1 The primary malignant are sarcomas in 95%; with the angiosarcoma being the most frequent and less than 5% of lymphomas.3 Cardiac and pericardium metastasis are more common that primary, specially in the case of lung carcinomas.4
The clinical manifestations vary according to the type of tumor, size and localization. In metastasis, initially there are no clinical findings and the diagnosis is done incidentally during the search of the primary tumor. They are detected because of the secondary symptoms of intracardiac obstruction, embolization or constitutional symptoms.5
The myxoma is found more often in women, with a 3:1 relation;6 between the ages of 30 to 60, and is usually located close to the fossa ovalis. About 75% are found in the left atrium and 20% in the right.2 Generally, these are unique masses, although in some instances they grow through the fossa ovalis compromising both atriums, in these cases the familiar myxoma or malignant tumors should be considered.6-8
The main techniques used for the diagnosis of cardiac tumors include echocardiography, magnetic resonance and tomography. Echocardiography is the most used, with excellent performance and allowing an estimate of tumor size, form, localization, mobility and valvular compromise, including the possibility of an evaluation of the rest of the cardiac structures. Additionally, it can differentiate other pathologies such as thrombi.2 In the case of unusual localization or findings, cardiac magnetic resonance or tomography, can aid in the diagnosis and determine the best therapeutic conduct.9
Clinical case
A 51-year-old male patient, whose chief complaint was short lasting episodes of temporo-spatial disorientation and a 4 kg weight loss in an 8 month period. As relevant past medical history the patient had a frontal meningioma resected 15 years ago, without recurrences on tomographic follow up. He had focal epilepsy as a sequel that was adequately controlled with carbamazepine 200 mg bid and levetiracetam 500 mg tid. The clinical and neurological exam was normal.
Neurology Department initiated studies to rule out ischemic cerebrovascular disease, with carotid duplex, which was reported as normal; 24-hour Holter monitoring, with sinus rhythm, without evidence of arrhythmias; and a transthoracic echocardiogram was performed finding an intracavitary mass (area 13 cm2, diameters 3.3 × 4.3 cm) that occupied nearly all of the left atrium, echogenic, with a pedicel that originated in the medial part of the interatrial septum and with irregular borders, that moved towards the entry tract of the left ventricle without obstructive phenomenon. Another image was located at the right atrium, of similar characteristics but of smaller size (area 1.4 cm2, diameters 1.7 × 2.4 cm); without being able to determine using this method, if it corresponded to the same mass that went through an interatrial septal defect or if it was independent. No valvular compromise or of the vena cava was observed (Figure 1).

Figure 1: Transthoracic echocardiogram. To the left, parasternal long-axis view where a mass in the left atrium is observed. To the right an apical four- chamber view where a mass that occupies the entire left atrium and partially the right is observed.
For better characterization of the masses, a transesophageal echocardiogram revealed 3 intracavitary masses in both atriums; the biggest occupied nearly all of the left atrium, with multiple lobes, another medium size mass in the right atrium that originated in the interatrial septum and seems independent of the mass, with color Doppler flow in the interior. Another small mass was documented in the right atrium attached to the lower part of the interatrial septum (Figure 2).

Figure 2: Transesophageal echocardiogram. To the left: TEE 27-degree view where a shunt in the mass of the right atrium is observed. To the right: TEE 50-degree view, a mass that goes through the interatrial septum, occupying the right and left atrium, is observed.
Due to the number of masses, the localization and the morphology of these, a cardiac magnetic resonance was performed, viewing one multi-lobed lesion hyperintense in T2, that compromised principally the left atrium and with lesser degree the right; in the dynamic sequences of early and late enhancement, there was a peripheral and patchy pattern uptake that persisted with capture defects in central nodular areas, findings that suggested as a primary diagnosis, a bi-auricular myxoma (Figure 3).
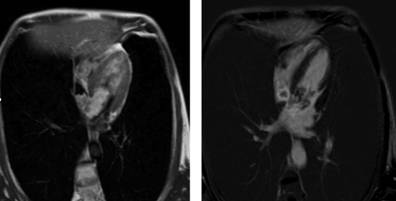
Figure 3: Cardiac magnetic resonance. To the left: mutilobed masses that compromise specially the right atrium and partially the left atrium, which are hyperintense on T2. To the right: peripheral and patchy enhancement of the contrast is observed and persists hypopcaptant in nodular central areas (characteristics of a myxoma).
A surgical resection of the tumor was recommended and preoperative tests were ordered; the coronariography showed epicardial coronaries without significant lesions and revealed a big branch originated from the circumflex that irrigated the tumor in the right topography (Figure 4).

Figure 4: Cardiac catheterization. Coronariography where a big vessel that originates in the circumflex artery is observed. It irrigates the mass in the right atrium.
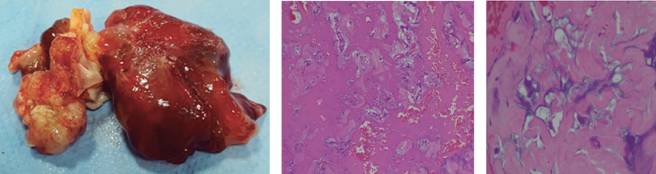
At the surgery a jellylike mass of 3 × 4 cm was located in the left atrium, that was implanted in the interatrial septum, invaded it and crossed to the right atrium, with different characteristics being pearl like with a «jellyfish» aspect with diameters of 2 × 2 cm. Frozen section biopsy reported findings compatible with a myxoma. During the surgical procedure a reconstruction of the interatrial septum with a bovine patch was required. The definite result of the pathology reported a bi-auricular myxoma (Figure 5).
Discussion
The primary cardiac myxoma is the most common primary tumor, presenting usually as unique lesions, and rarely show bi-auricular compromise because of invasive nature through a permeable foramen ovale, found only in 1% of the cases.6-8
The importance of an adequate imaging evaluation, depends that in the majority of the patients with myxoma or benign entities, the treatment is surgical removal, carrying an excellent prognosis. On the contrary, in patients with malignant disease such as lymphoma, radiotherapy and chemotherapy are the indicated treatment.10 An adequate diagnosis through imaging techniques can prevent unnecessary procedures without changing the patient’s prognosis.
Transesophageal echocardiography, allows a more sensitive evaluation of cardiac masses, even in sizes of less than 1 cm, lesions within the atrial appendage such as thrombus, tumors or fibroelastoma and determine the relationship with the cardiac valves.11 Despite this, echocardiography provides limited information of the tissue characterization, and the differentiation between benign and malignant tumors is not possible, nevertheless the magnetic resonance allows an excellent characterization of the cardiac masses.12
Several findings in tomography and magnetic resonance can help confirm the presence of cardiac myxoma. A mass with a stalk of small base that grows from the interatrial septum suggest the diagnosis of a myxoma. In thorax tomography, it frequently presents as an spheric mass with a smooth surface and typically with low heterogenous attenuation with calcifications in up to 14% of the cases.9,12
The variable quantities of mixed, hemorrhagic, ossific and necrotic tissue give an heterogenous appearance in the images of T1 and T2 in the cardiac magnetic resonance, with late patchy enhancement.12
In cases of tumors with atypical localization and morphology, the multimodal image study with echocardiography, tomography and/or cardiac resonance, must be done for the adequate diagnosis approach and to determine according to the findings, the best conduct for each patient.

