











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Vascular rings are anomalies of the aortic arch system that occur during the development of the embryo. In these anomalies, some vascular structures and the Ductal Ligaments (DLs) encircle the trachea and the esophagus, occasionally causing symptoms, like stridor and dysphagia. DLs are the result of the obliteration and fibrosis of the ductus arteriosus, and constitute an important component in the anatomy of vascular rings. The DLs close or complete the vascular ring.
Surgical and anatomic-pathological findings reveal the location of DLs in the different types of aortic arches:
In the left aortic arch, the DL is located in the aortopulmonary window, between the aorta and the left pulmonary artery. This happens even in the presence of aberrant right subclavian artery, with or without Kommerell’s diverticulum (KD).1-3 We have not found in the literature any description of a left aortic arch with aberrant right subclavian artery that forms a complete vascular ring.
In the right aortic arches, DLs can be found in the following locations: a) in the right aortic arch with a mirror-image branching pattern of the great vessels, the DL is located more frequently on the left side, between the left subclavian artery and the left pulmonary artery.4 b) Sometimes it is found on the right side, between the aortic arch and the right pulmonary artery. In no case does the DL close a vascular ring.5-7
In the right aortic arch with mirror-image branching and retroesophageal diverticulum, the DL is located between the retroesophageal diverticulum, which is a ductal diverticulum,8 and the left pulmonary artery.9,10 In this case, the DL always closes a vascular ring.
In a right aortic arch with aberrant left subclavian artery, DLs can be found: a) in the right aortic arch with aberrant left subclavian artery with KD, the DL is always located on the left side, between the left subclavian artery and the left pulmonary artery,1,6,3 and it always closes a vascular ring. b) In the right aortic arch with aberrant left subclavian artery, without KD, it has been reported that the DL is located on the right side, between the aorta and the right pulmonary artery, and it does not close a vascular ring.11 c) Right aortic arch with left aberrant subclavian artery without KD, with left ductus or DLs, is described in patients with Tetralogy of Fallot.12
In the circumflex right aortic arch, which is a right arch with retroesophageal component and left descending aorta, the DL is located on the left, between a ductal diverticulum located in the upper end of the descending aorta and the left pulmonary artery, and it always forms a vascular ring.4
In the double aortic arch we can find two DLs, one in each arch, but more frequently, there is only one DL located between the left aortic arch and the left pulmonary artery.11,13
In the right cervical aortic arch, which is similar to the circumflex right aortic arch, but higher up in the neck, it has a retroesophageal component, a left descending aorta and a left DL14 that always closes a vascular ring.
The only medically relevant DLs are those located in the double aortic arches, in the right aortic arch with aberrant left subclavian artery, in the right arch with a mirror-image branching with retroesophageal diverticulum, in the circumflex right aortic arch, and in the cervical aortic arch. In these locations, DLs close vascular rings. A common feature of all vascular rings is that they produce an indentation in the posterior face of the esophagus, shown in the contrast esophagogram.
Multi detector computed tomography (MDCT) and magnetic resonance imaging (MRI) provide images with excellent anatomic details of vascular rings, especially with the use of volumetric reconstruction (3D VR), whereas, it has been reported that, DLs cannot be seen using any imaging procedure.5,9,13,15-17
DLs division is described as part of the surgical treatment of symptomatic vascular rings.15,18 For this reason, we believe that finding the exact location of ductal ligaments before surgery would be useful.
The purpose of this study is to investigate the possibility of locating DLs with two imaging modalities: MDCT and MRI.
Material and methods
Between March 2006 and November 2016 we have diagnosed 102 cases of vascular rings. Of these, 82 were symptomatic patients with dysphagia, 15 were found while studying cardiopathies with MRI or MDCT, and 5 were found while studying other pathologies. In all the symptomatic patients, with dysphagia or stridor, we began the imaging study with a barium esophagogram, searching for a compression in the posterior face of the esophagus that would lead us to suspect the presence of a vascular ring. Patients with the radiological diagnosis of probable vascular ring were studied with MRI or with MDCT.
In our institution, we prefer to study congenital cardiopathies and vascular rings among the pediatric population with MRI and adults with MDCT, although we have studied several children using MDCT.
Of the 102 cases of vascular rings, 86 were studied with MRI, 46 of which were women and 40 were men, with ages ranging between 1 month and 17 years. The types of vascular rings studied with MRI are listed in Table I. We conducted the MRI studies with a Philips Intera 1.5T Scanner with a cardiac 5-channel synergy surface coil (Phased-Array) and electrocardiographic synchronization.
Children under seven years of age received sedation with chloral hydrate (40 mg/kg of body weight), and were monitored with electrocardiography and oximetry during the procedure. MR studies were made with the following cardiology protocol: a) Images without contrast in axial, coronal, long axis, short axis, and four chambers planes, in Turbo-Spin Echo T1 sequence (black blood), with a 170 to 250 mm field of view, depending of the size of the thorax, and a 512 matrix. b) Study with contrast, after intravenous injection of gadopentetate dimeglumine, 0.2 mL/kg of body weight, with acquisitions in Thrive T1 fast-field Echo for volumetric reconstruction images.
Of the 102 cases of vascular rings, 16 were studied with MDCT. Of these patients, 7 were men and 9 were women, with ages ranging between 4 and 83 years. The types of vascular rings studied with MDCT appear in Table II.

MDCT studies were made with a General Electric Light-Speed VCT CT scanner, without electrocardiographic synchronization. The following reconstruction parameters were used: 0.625-mm collimation, 0.625-mm slice thickness, tube potentials between 80 and 120 Kv. and a variable field of view according to the thickness of the patient. We used General Electric’s «ASIR» program to reduce exposure to radiation. The contrast material used is Iopramide 370 mg/mL, which is a non-ionic, low osmolar contrast, injected in a volume of 1.5 mL/kg of body weight.
The MR images were studied in a workstation, trying to visualize DLs in axial, coronal, long-axis, short-axis and 4-chamber slices, in Turbo-Spin Echo T1 sequence without contrast. Likewise, we reviewed the MDCT images in axial, oblique coronal, and oblique sagittal planes. The analysis was made using maximum intensity projections (MIP) with 3-mm thick slices and soft tissue window.
Findings
In none of the 86 vascular rings studied with MRI was it possible to visualize the DLs. In 14 of the 16 vascular rings studied with MDCT, we were able to visualize DLs and identify their location. The remaining two unidentified DLs, in the vascular rings studied with MDCT, were left aortic arches with aberrant right subclavian arteries, without KD. The location of DLs in vascular rings studied with MDCT is shown in Table III.

In five of seven cases of left aortic arches with aberrant right subclavian arteries, DLs were located on the left, between the aorta and the left pulmonary artery, and did not form vascular rings, even when the aberrant subclavian artery had KD (Figure 1). The DLs weren´t identified in the other two cases.

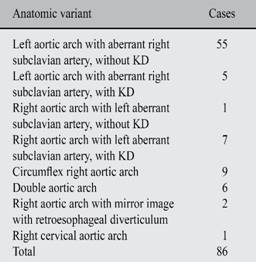
Figure 1: 43 year-old female with dysphagia. Contrast MDCT study shows a left aortic arch with right aberrant subclavian artery and KD. A) The 2D coronal reconstruction image shows right aberrant subclavian artery arising from KD (arrow). B) The oblique sagittal reconstruction 2D, 3-mm slice, shows a left DL (arrow), between the aortic arch and left pulmonary artery.
We found two cases of right aortic arches with mirror image branching of the great vessels. In the first, with situs inversus and dextrocardia,19 the DL was located on the right, between the aorta and the right pulmonary artery. In the second, with levocardia, we found a left DL located between the left subclavian artery and the left pulmonary artery. In none of the two cases a vascular ring was formed.
In the case of the right aortic arch with left aberrant subclavian artery emerging from a KD, the DL was on the left, between the left subclavian artery and the left pulmonary artery, and did form a vascular ring (Figure 2).

Figure 2: 71 year-old male. MDCT study shows right aortic arch with left aberrant subclavian artery arising from KD. A) Schematic drawing: a left DL (arrow) closes the vascular ring encircling trachea and esophagus. B) 3D Volume Rendered CT angiography shows a right aortic arch with left aberrant subclavian artery, arising from KD with calcified atheroma (arrow). C) 2D Oblique coronal reconstruction, 3-mm slice, shows a thick left DL (arrow) connecting KD to distal main pulmonary artery, completing the vascular ring.
In one of the two cases of right aortic arch with aberrant left subclavian artery without KD, the left DL closed the vascular ring (Figure 3). In the other case, the DL located on the right did not form a vascular ring (Figure 4).
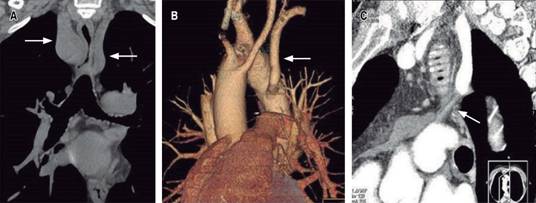
Figure 3: 62 year-old male with dysphagia. The MDCT study displays right aortic arch with left aberrant subclavian artery without KD, with left DL. A) 2D Coronal reconstruction image shows esophageal air compressed between the right aortic arch and the left aberrant subclavian artery (arrows). B) 3D VR of heart and great vessels shows right aortic arch with left aberrant subclavian artery (arrow) without KD. C) 2D oblique sagittal reconstruction image, 3-mm slice, shows left DL (arrow) between the aberrant subclavian artery and the pulmonary artery, completing the vascular ring.

Figure 4: 7 year-old child with dysphagia. Contrast esophagogram (not shown) suggests vascular ring. A) 3D VR MDCT angiography of heart and great vessels shows right aortic arch with left aberrant subclavian artery (arrow) without KD. B) 2D Oblique sagittal reconstruction image, 3-mm slice, shows right DL (arrow) between aortic arch and right pulmonary artery.
In the circumflex right aortic arches, left DLs located between a ductal diverticulum in the upper end of the descending aorta and the left pulmonary artery closed vascular rings (Figure 5).
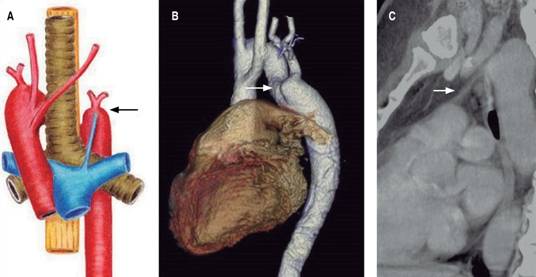
Figure 5: 40 year-old female with dysphagia. A) Illustrative drawing of right aortic arch with retroesophageal component and left descending aorta (circumflex right aortic arch). The left DL (arrow) closes a vascular ring. B) 3D VR MDCT angiography shows a circumflex right aortic arch, with ductal diverticulum in the upper end of the descending aorta (arrow). C) 2D Oblique sagittal reconstruction image, 3-mm slice, shows a left DL (arrow) between the ductal diverticulum and the left pulmonary artery, completing the vascular ring.
The two cases of right aortic arches with mirror-image branching of the great vessels and retroesophageal diverticulum presented left DLs, located between the ductal diverticulum and the left pulmonary artery, and they formed vascular rings (Figure 6).
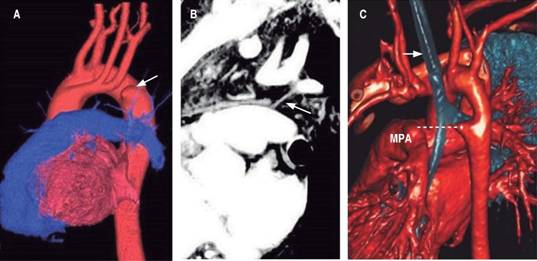
Figure 6: 50 year-old male with dysphagia and illustrative case. A) 3D VR MDCT angiography shows the right aortic arch with mirror image branching pattern, with retroesophageal diverticulum (arrow). B) The 2D oblique sagittal view, 3-mm slice, shows a left DL between the ductal diverticulum and pulmonary artery (arrow), completing the vascular ring. C) An illustrative case from AJR13 (with permission). CT angiography of 15-month old boy, displays right aortic arch with mirror image branching pattern and retroesophageal diverticulum (asterisk). Dotted line indicates location of DL.
In the 14 cases of vascular rings, in which we identified DLs, the indentation in the esophagus was caused by a compression of vascular elements, such as aberrant subclavian arteries, KDs or ductal diverticulums. In no case the indentation was produced by DLs compression, DLs cause the anchoring of the vascular elements with the pulmonary artery.
Discussion
We have not found in the medical literature any article that investigates the possibility of visualizing DLs with an imaging technique. However, some articles assert that DLs cannot be seen with any imaging technique.5,9,13,15-17 Our work was designed to investigate the possibility of visualizing these ligaments with MDCT and with MRI, with the parameters normally used in heart, and large vessel studies, and we found that with MRI, in the planes and sequence used by us, it was not possible to visualize DLs in any of the 86 vascular rings studied, and that with MDCT, it was possible to visualize them in 14 of the 16 cases. We couldn’t find an explanation for not being able to visualize the DLs In the remaining two cases studied with MDCT. Both patients had left aortic arches with aberrant right subclavian arteries without KDs and, without congenital cardiopathies that lead us to suspect agenesis of the ductus arteriosus.
The planes we used in the MRI study are those used in cardio resonance, and the sequence employed was Turbo Spin Echo T1. We have not tried this method with other planes or with other sequences.
We have found only two reports of casual visualization of DLs with MRI. The article by Paparo F.20 describes the visualization of the DL between the KD and the pulmonary artery in a right aortic arch with aberrant left subclavian artery. Paparo shows the DL in an oblique sagittal slice made with Fast Spin Echo T2 sequence. This means that he visualized the DL in one of the planes we used in our work, but with a different sequence. Whether this technique can be used to visualize DLs in a different type of vascular ring remains to be investigated. The article by Zachary CH21 presents a case of right aortic arch with mirror image-branching and retroesophageal diverticulum, where the DL was identified in an axial slice in T1-weighted sequence. It is our opinion that what Zachary CH shows does not correspond to a DL. The upper image in Figure 2 21 shows a fine, dashed line running from a vertebral body to the pulmonary artery, which the author describes as «a thick ligament running from the aorta to the pulmonary artery», while in the lower image in Figure 2,21 where we can clearly see the descending aorta with the diverticulum, no LDs are shown. The case presented by Zachary does indeed correspond to a right aortic arch with mirror-image branching and retroesophageal diverticulum. But in our opinion, the DL does not appear in these images.
DLs are fibrous structures that follow an oblique path, from top to bottom and back to front. Using MDCT, we were able to visualize 14 of these DLs in the oblique sagittal planes, and in just one case in an oblique coronal plane, but never in the axial planes. Multi Detector CT scanners have the capacity to reconstruct high-resolution coronal and sagittal planes thanks to the production of isometric voxels. The previous generations of CT scanners lacked this capacity, so probably these scanners could not identify DLs.
As in our casuistry we did not have any double aortic arch cases studied with MDCT, we do not know whether it is possible to visualize DLs in this pathology.
In the vascular rings studied with MDCT, we have found a right aortic arch with aberrant left subclavian artery without KD with a left DL, which formed a symptomatic vascular ring (Figure 3), a variant we haven’t found reported in patients without cardiopathies. This pattern is described in patients with Tetralogy of Fallot.12 According to the classic concept, right aortic arches with aberrant left subclavian arteries without KD have the DL to the right and do not complete rings,11 as in the case of Figure 4 of our casuistry. Probably, if we keep looking for DLs with MDCT we will find more cases of this type of rings.
In the cases where DLs complete vascular rings, we find that DLs do not cause compression of the trachea or the esophagus, vascular structures such as aberrant subclavian arteries, KDs and ductal diverticulums are responsible for the compression. DLs cause the anchoring of the vascular structures to the pulmonary artery, a finding that has already been reported.22
Conclusions
Although several sources of medical literature assert that DLs in vascular rings cannot be seen using any imaging procedure, it was possible to identify them using MDCT, in coronal and oblique sagittal planes in 14 of 16 cases. However, we were unable to locate DLs in any of the studies of vascular rings made with MRI, in the planes and sequence employed in Cardio Resonance, in our hospital.

