











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Cardiovascular diseases remain the leading cause of morbidity and mortality worldwide; increasing prevalence in all age groups. The World Health Organization (WHO) has estimated that by 2050 20% of the population will be elderly; which is why the number of octogenarian patients who undergo coronary angiography is rising.1
It is clear that the realization of PCI has improved the survival of patients with ischemic heart disease.2 However, the octogenarian patients, are usually excluded from clinical studies where the use of PCI were compared.3 Therefore, the management of these patients is based on the extrapolation of the results obtained in young patients.4
Patients over 80 years are the group of patients who have come to show a major change in prognosis when invasive coronary procedures are done, because the mortality of patients with acute coronary syndromes is more in elderly patients.5-7 Despite these findings, the number of octogenarian’s patients that undergo invasive procedure are less, studies have shown that this is mostly due to the fear of more complications.8
The RA has proven to be superior to FA in coronary angiography, because it has been shown that has fewer local complications, besides that patients can be mobilized faster. However, the RA is technically demanding.1
There are few studies comparing the use of PCI between patients younger and older than 80 years; and even less comparing the RA against FA in octogenarian patients, in terms of VC, RD, RT, mortality and LHS. That is why the aim of this study is to compare patients older than 80 years who underwent coronary angiograms against younger than 80 years; and secondarily compare both approaches in this group of patients.
Material and methods
This is a retrospective, observational, comparative, longitudinal, single-center study. All patients over 18 who underwent PCI during the period from January 2010 to March 2016 were included. The study was conducted at the Christus Muguerza High Specialty Hospital, which is a private hospital of 200 beds, located in northeastern Mexico, with two cardiac catheterization laboratories, where about 400 endovascular coronary diagnostic and therapeutic procedures are performed annually.
The patient data were collected from the files of catheterization laboratories. All those patients in whom there had not been full information for the purposes of the study were excluded. Patients were divided into two groups, the OG and the YG. Epidemiological variables such as diagnosis by which the patient underwent the PCI, comorbidities, access used, prevalence of multivessel disease, RT, RD, quantity of CM used, VC, death and LHS were collected. Furthermore, in the OG both access were compared.
Statutes governed by the Declaration of Helsinki were followed.
The MedCalc® program was used for statistical analysis. Continuous variables are presented as means with standard deviation or medians with their interquartile ranges, depending on whether or not show a normal distribution, and were compared using the Student t test or the Mann-Whitney test. Categorical variables are presented as percentages and were compared using the χ2 test or Fisher’s exact test. It was determined as statistically significant a p-value < 0.05.
Multivessel disease was defined as the presence of obstruction of more than 50% of two or more vessels. The VC were those related directly to the site of access and divided into local hematoma/bleeding, retroperitoneal hematoma, vascular dissection, thrombosis, pseudoaneurysm.
Before the procedure, bilateral femoral and radial pulses were evaluated by a physician. Selection of the access site was individualized per the preferences of the operator. Radial sheaths for diagnostic and interventional procedures had a diameter of 5- and 6-F, respectively. For the transradial approach, 0.3 mg isosorbide dinitrate to prevent radial artery spasm and 5,000 IU of unfractionated heparin (UFH) to prevent thrombosis were injected directly into the radial artery through the sheath; 5-F sheaths were used for transfemoral diagnostic procedures. Transfemoral interventions were performed using 6-F-7F. Hemostasis was obtained in the RA using a pressure bandage (TR-band), immediately applied to the puncture site without a period of manual compression. In the FA was obtained by manual compression and the patient were restricted to bed rest for 6 hours. After an interventional procedure via FA, vascular closure devices (Angioseal) were used in 150 of the patients (17%).
The angiographic unit is equipped with a flat panel image detector (Innova 3100, General Electric), which offers a choice of four-dimensional image field of 30 × 30 cm, 20 × 20 cm, 16 × 16 cm and 12 × 12 cm. In addition, the unit is capable of performance pulsed fluoroscopy at ranges of 7.5, 15 and 30 images per second, and acquisitions of 15 to 30 images per second.
The RD is the amount of energy deposited locally per unit mass tissue, it expressed in milligray (mGy).
The RT, in this study, was the amount of time in minutes when the pulsed fluoroscopy or acquisition of the images were activated.
Compliance with ethical standards
This study was not funded by anybody. Authors declare no conflict of interest. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Results
A total of 1,282 patients were collected (Table I), of whom 92 were of the OG and 1,190 in the YG. With an average age of 83 years (± 2.8) in the OG versus 61 years (± 10.9) in the YG. A proportion of 52% of men in the OG, compared to 76% in the YG (p ≤ 0.0001). A higher BMI was observed in YG (26.3 (± 4.2) versus 28.4 (± 7.5) in the OG; p = 0.01).
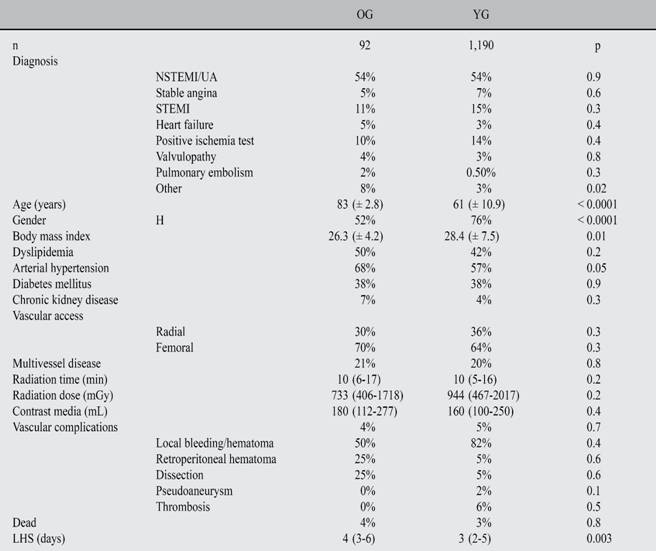
Among the most prevalent comorbidities in the two groups were dyslipidemia, hypertension and diabetes mellitus 2, there was significant difference in the proportions of hypertensive patients (68% OG versus 57% YG p = 0.05). Regarding diagnosis by which coronary angiography was performed, it was documented that in both groups the most common diagnosis was non-ST-segment elevation myocardial infarction (NSETMI)/unstable angina (UA) (54% versus 54%; p = 0.9); while in second place was ST-segment elevation myocardial infarction (STEMI), being slightly higher in the YG (11% versus 15%, p = 0.3).
The FA was the most used in both groups (70% YG versus 64% OG; p = 0.3). There were no statistically significant differences in the RT (10 (6-17) OG vs 10 (5-16) minutes YG; p = 0.2); nor in the RT (733 mGy (406-1718) OG versus YG 944 mGy (467-2017); p = 0.2); neither in the amount of CM administered (180 mL (112-277) OG versus 160 mL YG (100-250); p = 0.4).
In the aspect of VC related to the approach used, there were less complications in the OG (4% versus 5%; p = 0.7); in both groups the local bleeding/hematoma was the most common vascular complication. Mortality was similar (4% OG vs 3% YG; p = 0.8). OG patients hospitalized lasted more days (4 days (3-6) versus 3 (2-5); p = 0.003).
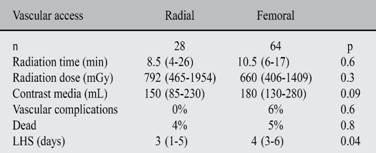
Comparing the RA versus the FA (Table II) in the OG, the latter was the approach most commonly used (70% (n = 64) versus 30% (n = 28)). There were no statistically significant differences in the RT (8.5 minutes (4-26) RA versus FA 10.5 minutes (6-17); p = 0.6), nor in the RT (792 mGy (465-1954) RA versus FA 660 mGy (406-1409; p = 0.3); neither in the amount of CM administered, although in the RT was lower the amount (150 mL (85-230) versus 180 mL (130-280); p = 0.09). There were no site-related VC in the radial access (0% vs. 6%; p = 0.6); the complications in the FA were 50% local bleeding/hematoma, 25% retroperitoneal hematoma and 25% dissection. Patients who underwent FA had more LHS (3 days (1-5) versus 4 days (3-6); p = 0.04).
Discussion
In this study, it was documented that only 7% of all patients who underwent a PCI, corresponded to the OG, which had already been described in the literature.9 This group of patients are poorly represented due to higher risk that reduces the number of such procedures offered to octogenarians.3,6,10
In this study it was observed that the NSTEMI/UA were the most common PCI in the OG, which is consistent with that reported by Kolte D, et al.11 There was a slightly larger proportion of comorbidities in the OG, as described Koutouzis M, et al 1 in their study. Significant difference was found in the proportion of patients with hypertension, being higher in the OG.
It is worth noting that the proportion of women (48%), increases to be almost equal to that of men (52%) in the OG; compared with the rest of the population, where the male is the dominant (76%)
There were no statistically significant differences between the two groups regarding the site of access, being more frequent in both the FA; this correlates with the report of Gunarathne A, et al,12 where also was the preferred access. However, there is literature5 in which the radial is the access site of choice.
A significant data of this study was that the proportion of patients with multivessel disease was similar in both groups of patients, in contrast to what was reported by Yan BP, et al 7 where they had reported that patients older than 80 years had more complex lesions and more multivessel disease.
No statistically significant differences as to the RD or RT in both groups were found. Hu F, et al13 had reported an increase in amount of 20 mL of CM on average in octogenarian patients, compared with the younger group, which could adversely affect renal function in these patients, increasing the risk of contrast-induced nephropathy.14 In this study there was a difference of 20 mL of contrast, with no significant differences between the two groups.
In both groups similar proportions of VC related to the procedure were documented, in contrast with those reported by Buber J, et al,15 which reported the more number of VC in octogenarian patients. The literature16 mentioned that after the procedures bleeding complications were a major risk factor for the outcome of octogenarian patients and more complications were reported, however, in the study this group of patients had not a higher incidence of complications. This correlates with mentioned by Martin, et al.5
There are many studies in which it is described that patients older than 80 years have a higher mortality subsequent to a PCI;1,7,10,17-19 this differs from this study since no statistically significant difference in mortality in both groups and even mortality was similar to that reported by Koutouzis M, et al.1
The group of octogenarians had higher LHS, this finding was also reported by Gale C, et al.6
Comparing RA vs the FA in the OG there was no statistically significant difference in the RT and RD, although they were discreetly higher in patients who underwent RA, this finding was already reported earlier;1,13,20 this may be because in these patients is more demanding this approach because vascular abnormalities.
There were no VC associated with a RA, compared to 6% in patients with FA, however, this difference was not significant. However, Martin AC, et al5 had already suggested that the RA should be used in these patients, especially those at high risk of bleeding complications.
Contrary to what was reported for Jaffe R, et al21 which mentions that RA requires greater amounts of CM, in this study was found that the FA required more amount of CM used, although it was not statistically significant, it could prevent the development of contrast-induced nephropathy using the RA, because it is a risk factor in this age group for the development of this clinical entity. Gunarathne A, et al12 reported that FA was associated with increased mortality in elderly patients, in this study mortality values were found similar in both access. There are reports in the literature22 where it is mentioned that RA is an effective therapeutic measure with equally successful, fewer complications and better clinical outcomes compared to the FA.
In the literature13 it has been reported less time in hospital and early mobilization of patients who undergo the RA, which could help reduce the risk of venous thrombosis and pulmonary embolism in this group of patients. Even Ziakas A, et al23 reported that in patients of this age is safe the hospital discharge on the same day of the procedure.
This study has limitations because is a single-center, observational and there was little sample in the OG, because of these there were not statistically significant differences comparing both approaches. It is relevant that exists few studies in the literature that report the outcomes of these access in this group of patients, which gives greater value to the data reported in the research.
Conclusion
There were no statistically significant differences in the type of access, RT, RD, amount of CM, VC associated with the site of access, and death between the OG and YG, however, octogenarian patients had more days in the hospital. When comparing, sites access in octogenarian patients there were no statistically significant differences in RT, RD, amount of CM, VC associated with site access, death, except that greater LHS in the FA.

