











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Initially is important highlight two types of systematics responses to the exercise, one is the acute and the other is the chronic. The first one is about the increase in the oxygen consumption (VO2), and the chronic is about adaptive changes, given at a long term and it can be also seen at rest.1 Hill et al. described for the first time the VO2max as the highest rate at which the body is able to consume oxygen during intense exercise.2 It is also important to mention that this Vo2max varies according to lean body mass, age, gender and genetic characteristics of the individual.3
Other authors have defined the VO2max as the maximum amount of oxygen that the body is able to absorb, transport and consume per unit of time.4,5 Highlighting that the VO2max is the measure used to talk about the intensity of an exercise, determining that the exhaustive exercise is above 70% and the slight exercise below 40%.3
Currently, there are many methods to determine VO2max. either in laboratories or outdoors. Among the field test, the most widely used worldwide is the Course Navette 20 meters, also known as 20 m Shuttle Run Test, test round trip in 20 meters or test of Leger.6,7
The test of Course Navette or test of Leger 20 meters after more than 30 years of use and recognition remains one of the most widely used to study the cardiorespiratory component, in both sexes and in a broad age range. This is because: 1) the correlations obtained with the direct VO2max; 2) the predictive stability in subjects with different levels of physical condition; 3) the good test-retest reliability; 4) the sensitivity to monitor post-training changes; 5) your relationship to health and diagnostic capacity; 6) the possibility of dosing workloads correcting the final speed reached and 7) mainly, the original idea of carrying it out on a tour round trip in 20 meters.5
On the other hand, the exercise not only causes changes in VO2max. but also in the different body systems; either acutely or chronically, but within the relatively less considered, is the hematological. Of this latter, the literature refers to changes in blood volume, in the activity of white blood cell populations, as well as changes in cellular and humoral immunity, and in the count and platelet shape.8
Firstly, as an initial response to the exercise has shown that during and until one hour after a strenuous physical exertion, there exist dehydration and hemoconcentration with increased in the Hb concentration, in the hematocrit (Hct) in the erythrocyte count and decrease in total blood volume (BV) at the expense of decreased primarily plasma volume (PV),9,10 which can be, with respect to pre-exercise values of up to 18%. These changes are greater as they go longer and the exercise is intense, and lowers if the degree of training is higher; likewise, if the exercise is less than 40% VO2max during training sessions tend to not altered the above hematological parameters.
The World Health Organization and most medical organizations recommend associate diet and physical activity to promote health and reduce the growing incidence of obesity in the world population.11,12 One strategy that has arisen to increase the «burn» fat is to perform a moderate intensity exercise and fasting prior to the session.13,14 Understood by fasting according to the Royal Spanish Academy as «Abstinence from all food and drink from twelve o’clock antecedent».
Therefore, during the approach of this research came the question: What are the hematological changes and cardiopulmonary results after the test of Course Navette? In order to know the physiological changes that generates this test on students at the University of Santander, headquarters on Cucuta-Colombia.
Material and methods
An observational, descriptive and transversal study was realized that quantifies cardiovascular risk, VO2max and hemodynamic changes through the test of Leger in a population of 100 (57 women and 43 men) students was performed with an average age of 21 ± 2.43 years, they attended the premises of the University of Santander, headquarters on Cucuta-Colombia. At an altitude of 320 meters above sea level. Geographical coordinates: 7o54 of north latitude and 72o30 West of Greenwich.
Participants must be over 16 and under 26 apparently healthy and to sign an informed consent, supported by the research committee of Physiotherapy program at the university. We excluded participants with pain in lower limb, breathlessness or fatigue bigger than 3, participants with cardiovascular disorders or a history of cardiovascular surgical type or acute myocardial infarction. As retirement criteria were taken into account hemodynamic instability during the test and the manifestation of not wanting to continue.
The scheduled day of the test, began with the collection of demographic data (gender, age, ethnicity, personal history, family history and identification of cardiovascular risk factors) using a questionnaire for the identification of cardiovascular risk factors and personal data of the students. Then, the physiological measures (heart rate, blood pressure, blood oxygen saturation, dyspnea and fatigue) were determined pre and post-test Course Navette, using a portable pulse oximeter (Nellcor Puritan Bennett) for heart rate and saturation arterial of the oxygen. Systolic and diastolic blood pressure was taken manually and perceived dyspnea and fatigue by the modified Borg scale.
Anthropometry (weight, height, BMI, abdominal and hip circumference) it was determined by Tezzio TB-30037 digital scale previously calibrated and placed on a flat surface and with a good support, with all of its angles in contact with the floor. And the size with the measuring rod Adult Acrylic Wall Kramer 2104 placing the patient standing with his head in Frankfort plane and shoulders relaxed to avoid lordosis, in an upright position making sure that the back of the heels, calves, buttocks, back and head touched the wall. Z score obtained (Z-score) for BMI (kg/m2) through software Microsoft Excel 15.0, developed on headquarters with the reference of the World Health Organization was obtained. BMI Z score allowed the sample group in underweight, normal weight, overweight and obesity.
For abdominal circumference was necessary that the participant was lightly clothed in a standing position, with the abdomen relaxed and with arms folded across his chest, the examiner surrounded the participant’s waist with metric tape; then, arms goes in a relaxed position and close to the trunk. The measurement was performed at the narrowest level, between the tenth rib and the iliac crest, at the end of a normal expiration without the tape pressing the skin. This measurement was performed with an inextensible anthropometric tape. To determine the normal values of abdominal circumference, the reference values were used according to Buendia et al.15 (Men 91 cm and Women 89 cm).
For cardiopulmonary component the test of Course Navette round trip 20 meters was performed to exhaustion. The race pace was determined by a beep. The initial velocity was 8.5 km/h-1 and increased to 0.5 km/h-1 with one minute intervals, called stages, in the morning time around the synthetic field at the University of Santander, headquarters on Cucuta. It should be noted that the participants were previously informed that they could not consume some kind of food or sugared drink after 7 o’clock at night and that state should remain until 7:00 am on the college campus, to wait for indications from the investigators. However the participants were called the night before the test at 6 pm to remember the instructions of the research. Likewise, could not drink alcohol, coffee, smoke or use any drugs or medication that could interfere with its performance on test day. After completing the anthropometric measures, questionnaires and first sample of blood glucose, the participants performed the test of leger under the parameters previously mentioned. Once the Leger Test is finished, the researchers take vital signs again and the bacteriology the second sample of blood glucose. After the completion of the entire fieldwork process; the participants were given a standard breakfast for their metabolic stabilization and supervision during the following 30 minutes of rest. Aerobic capacity was determined through maximum oxygen consumption VO2max, estimated from the equation Léger (Léger, Mercier, Gadoury, & Lambert, 1988). Also, hematological tests and glycemic were taken before and after the test by a professional Course Navette bacteriologist and then analyzed in the clinical laboratory.
The design and development of the research was conducted under the ethical considerations of the Helsinki Declaration and Resolution No. 008430 of the Ministry of Health of Colombia and under the authorization of the directors and program coordinators physiotherapy at the University of Santander, headquarters on Cucuta.
Statistic analysis
For the description of quantitative variables, it was necessary to express as the arithmetic measure and standard deviation. Regarding the comparison of pre and post data to the test Course Navette, the ANOVA (analysis of variance one-way) was performed to compare the differences of gender and ages in the different variables studied, in addition to testing post hoc by Tukey test, to see the differences between the different age groups, gender and anthropometry. In all cases the level of significance was established at 5% (p < 0.05) and were performed in Stata 12 (Data Analysis and Statistical Software) program.
Results
After analyzing the data obtained during the fieldwork; which it was conducted with a total sample of 100 (57 women and 43 men) students who attended the premises of the University of Santander, headquarters on Cucuta-Colombia, whose sociodemographic characteristics studied allow to identify an average age for both genders of 21 ± 2.43; made up of 57% women and 43% men. On the academic level, 100% were undergraduate students at the University of Santander.
The risk factors identified were: arterial hypertension, overweight and/or obesity, cardiovascular risk according to abdominal circumference, diabetes, smoking, family history (diabetes, acute myocardial infarction and hypertension), alcohol intake and fatty foods; being most prevalent family history as hypertension, myocardial infarction, diabetes, cancer and kidney failure. Regarding cardiovascular risk factors in the sample study, it was determined 8% to smoking, 30% alcoholism and intake of fatty foods more than 3 times per week and sedentary lifestyle was 60% and 56% respectively. Similarly, it was identified that 32.6% of men and 17.5% of women have a high cardiovascular risk related with abdominal circumference. With respect to cardiovascular risk associated with abdominal/hip circumference it was found that 18.6% and 40.4% of men and women respectively, present a high cardiovascular risk. And in relation to the abdominal/size circumference was identified that 41.9% of male and 45.6% women have a high risk (Table I).

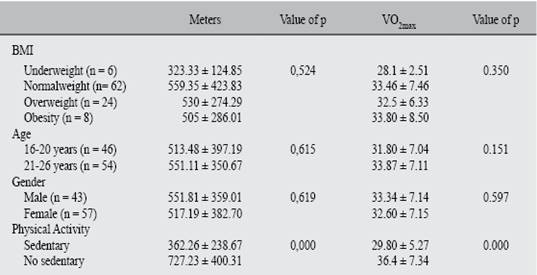
From the point of view anthropometric the 6% showed underweight, 62% normal weight and 24.5% and 8% overweight and obesity respectively. Next, the results achieved in the test were analyzed by the test of Course Navette obtaining 551.81 ± 359.01 meters traveled for men versus 517.19 ± 382.70 in women (p = 0,619); in VO2max. 33.34 ± 7.14 was achieved in men compared with 32.60 ± 7.15 for women (p = 0,597).
Also, according to the body mass index and the meters traveled, in underweight it was 323.33 m ± 124.85, 559.35 m ± 423.83 normal weight, 530 m ± 274.29 overweight and obesity with 505 m ± 286.01 (p = 0,524). When relating with VO2max. the students with underweight reached a VO2max of 28.1 ± 2.51, 33.46 ± 7.46 normal weight, and values of 32.5 ± 6.33 and 33.80 ± 8.50 for overweight and obesity respectively. With respect to physically active participants, it was determined that participants who exercise more than 3 times a week, run more meters (727.23 ± 400.31 versus 362.26 ± 238.67; p = 0,000) and greater VO2max (36.4 ± 7.34 versus 29.80 ± 5.27; p = 0,000) in the Leger test compare to sedentary participants (Table II).
On the other hand, we can stand out that the tests performed were significantly high intensity for participants, since 93% (M: 100% versus W: 94%) mentioned an effort between strong and extremely strong (score of 5 to 10) after the test according to the Borg scale for fatigue; for assessing dyspnea the 90% (M: 88% versus W: 91%) mentioned according to the Borg scale a dyspnea severe to extremely severe (grade 5 to 10) after the Course Navette test of 20 meters.
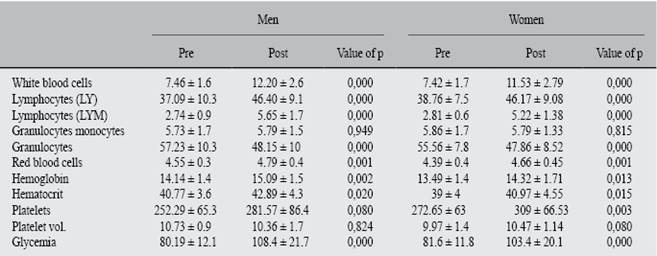
At the same time, comparing the glycemic levels after the test of Course Navette it was found that before the test was 80.99 ± 11.91 and after 105.59 ± 20.89 (p = 0,000). With respect to the hematological components there were significant changes in red blood cells, white cells, lymphocytes, granulocytes, hemoglobin, hematocrits and platelets (p = 0,000) in the samples post-test of Course Navette 20 meters (Table III and IV).
Table III: Physiological and hematologic differences post Course Navette test.
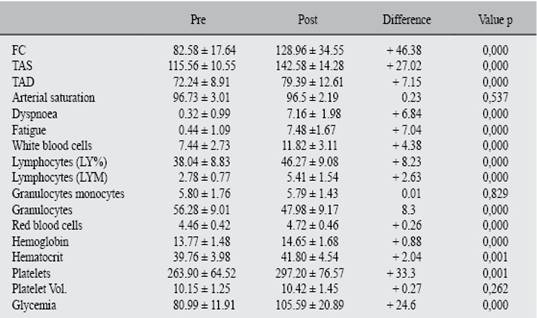
HR = Heart rate; SBP = Systolic blood pressure; DBP = Diastolic blood pressure.
Discussion
Some authors mention that exercise at moderate intensities, combined with a pre-carbohydrate intake, even in few portions and especially if high glycemic index, significantly decreased lipid oxidation in the exercise, so the recommendation is fasting, where priority is to decrease adipose tissue.16 However, various investigations have mentioned that fasting raises problems as favoring protein catabolism, decreased sports performance and the risk of hypoglycemia during exercise.13,14,17,18 Oetinger et al19 mention that exercise at fasting causes an increase in catecholamines, cortisol and high levels of peptide natriuretrico who plays an important role in exercise-induced lipolysis. In addition, leptin and insulin show a decrease in their concentrations. Being contrary to the results found regarding glycemia, which increased significantly in the undergraduate students evaluated, which is due to run-time test of Course Navette, being this relatively short compared to a moderate-intensity exercise for a minimum of 30 minutes to see these metabolic effects. It is for this reason that Moro C et al.20 emphasize that in short periods of exercise exists an increase of glucagon as a hyperglycemic hormone, which would suit the results.
According to VO2max. Baez Y. and Agudelo C.21 performed Course Navette test in young footballers resulting in 56.09 ± 4.05 mL/kg/min versus 31.80 ± 7.04 mL/kg/min found in our study population with a percentage of 56% of sedentary lifestyle; which shows clearly a better average VO2max. in young athletes versus sedentary young. Identical results when comparing the performance of young university students evaluated with the research of Silvestre et al. (2006),22 Oliveira (2007),23 Moraes & Herdy (2007).24
Likewise, Salcido J et al. in his work «Comparison of maximal oxygen uptake, adjusted to muscle mass, among young overweight and normal weight, with moderate level of physical activity» showed similar results in determining that university students with normal weight have a higher average VO2max and meters traveled compared with overweight youth.
Conclusions
In this investigation it was possible to conclude that significant changes in heart rate (p = 0,000), systolic blood pressure (p = 0,000) and diastolic (p = 0,000) but not in arterial oxygen saturation (p = 0,537). From the perception of dyspnea exercise (p = 0,000) and fatigue (p = 0,000) according to the Borg scale there were significant changes after test Leger.
Regarding hematological analysis, we conclude that there are no significant differences in monocytes granulocytes (p = 0,829) and platelet volume (p = 0,262) after test Leger. However, it can show that there exist significant changes in the levels of white blood cells (p = 0,000), red blood cells (p = 0,000), lymphocytes LY (p = 0,000) and LYM (p = 0,000), granulocyte (p = 0,000), hemoglobin (p = 0,000), hematocrit (p = 0,001) and platelets (p = 0,001) after test.
Indeed, it was determined VO2max levels. in the study population; concluding that there were no differences between men and women regarding VO2max (p = 0,059), speed (p = 0,794) and meters traveled (p = 0,794). But there were differences between physically active vs. sedentary participants (p = 0,000). Likewise, there was a higher consumption of VO2max in patients with a higher BMI and/or older.
With respect to blood sugar levels, it was evident an increase (80.99 ± 11.91 versus 105.59 ± 20.89; p = 0,000) after the Course Navette test.
These results obtained in this research allowed to determine and correctly analyze the fitness level of students at the University of Santander, headquarters on Cucuta-Colombia; indicating the need to implement strategies aimed at improving the fitness level and lifestyle of young university students in the city.

