











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The heart rate (HR) is the number of times the heart contracts for a minute, your cardiovascular measurement is easy to perform and adequate HR is essential for the proper functioning and evaluation of the heart.1,2 Actually exist devices for making heart rate; including porTable pulse oximeter and the Polar system that has proved more effective and accurate than manual take.
The maximum heart rate (MHR) is the maximum number of beats that can reach the heart at a high physical exercise, because the body responds to exercise increasing its MR and, if exercise is intense enough MHR will be obtained. This is very easy cardiovascular measurement, compared with invasive or noninvasive used to estimate stroke volume and cardiac output procedures. The MHR is used to determine, control and monitor training intensity and likewise know the limit of beats per minute that can reach the heart without compromising the health (ACSM 1994).
Consequently, the HR measurement routinely used to assess response and/or recovery of the heart to exercise, as well as to prescribe exercise intensities according to the MHR individual.3 The MHR can be determined in two ways: the first is through a record of the highest HR obtained after a high-intensity effort;4,5 the second, by means of equations that estimate a subject MHR.6 The estimate of the MHR has been a feature of exercise physiology and applied sciences, since late 1938 Robinson7 began raising the formula 212-0.77 * Age, which is very different from the widely accepted formula "220-Age" which, has long been the major reference in the estimation of the MHR. However, this equation is presented in books, sports medicine, and exercise physiology; without an explanation or citation of research.8 Likewise, Tanaka et al. in 20019 suggest a formula very well received today (208.75-0.7 * Age) apparently healthy adult subjects. In addition, there are more than 45 equations to determine the MHR according to different variables such as age and gender; but there are other variables that can influence the response of the MHR and that have not been taken into account by these equations.10
Similarly, the stress test is an important clinical tool for assessing11 from two points of view: a) protects the health through prevention and early diagnosis of coronary heart disease or ischemic heart disease (angina pectoris, myocardial infarction, sudden death), and b) support scientific physician training process.12 And it is not limited to that, but allows conclusions about the functional capacity, the response of blood pressure (BP), maximum heart rate, arrhythmias, the result of a given medical or surgical treatment, among others. It is one of the tests that provide more information at a lower cost.13
Currently, the stress tests are performed through established protocols known multistage, ie comprise several phases or stages usually about 2-3 minutes, with progressive increase of the load requires increased physical effort, and is the highest degree of effort reached corresponding to the functional capacity of patients in the study, as with the Bruce protocol, one of the most used internationally (Maroto y De Pablo 2011). However, for some patients the Bruce protocol can be very demanding, so there are other protocols like Naughton, which is to increase a little softer load every two minutes. This protocol has been widely used in the assessment of patients with heart failure or elderly patients.
Therefore, during the approach of this research came the question: How valid and effective are the equations to find the maximum heart rate?, in order to perform this research, I set out to achieve identify the validity and effectiveness of existing formulas comparing them with the results obtained through a stress test according to the Bruce protocol.
Material y methods
An observational, descriptive and cross-sectional study quantified the cardiovascular risk was performed, the maximum heart rate obtained through a stress test and theoretical equations in a population of 300 (181 women and 119 men) participants with an average age of 26 ± 10 years, who they attended the Rehabilitar Cucuta IPS located in the city of Cucuta-Colombia. The participants must be 18 years old, apparently healthy and to sign an informed consent, endorsed by the ethics committee of the institution. We excluded participants with lower limb pain, dyspnea and/or fatigue greater than 3, participants with cardiovascular disorders or a history of cardiovascular surgical type or acute myocardial infarction. As retirement criteria were taken into account hemodynamic instability during the test and the manifestation of not wanting to continue.
To collect sociodemographic, anthropometric and physiological data an instrument, which was used for the filled of questionnaire the patient. We proceeded first to perform measurements sociodemographic (gender, age, ethnicity, identifying risk factors, personal history, family history), physiological (blood pressure, heart rate, blood oxygen saturation) and anthropometric (weight, height, BMI) by the balance (Health o Meter) previously calibrated (accuracy = 0.1 g and 0.1 cm respectively), weight and height of patients was evaluated determined by placing the patient standing with Frankfort plane and shoulders relaxed to avoid lordosis. Was obtained Z score (Z-score) for BMI (kg/m2) through Excel, developed based on the WHO reference. The Z score of BMI allowed the sample group in underweight, normal weight, overweight and obesity. The stress test was performed on a treadmill with the Bruce protocol; patients could not drink alcohol, coffee, and smoke or use any drugs or medication that could interfere with the MHR. Perceived dyspnea and effort were assessed by the modified Borg scale (Table I).14

Heart rate was obtained by the Polar RS800CX Multisport system, while blood oxygen saturation with porTable pulse oximeter (Nellcor Puritan Bennett); both measurements were taken before, during and after the stress test. Systolic and diastolic blood pressure was taken manually at the start, end and after 5 minutes the stress test ended.
It was considered as a dependent variable (or result) the value of the MHR obtained after a maximum effort. As independent variables (or predictors) were taken the various equations formulated to calculate the MHR (Table II).

The design and development of the research was conducted under the ethical considerations of the Declaration of Helsinki and Resolution No. 008430 of the Ministry of Health of Colombia.
Statistic analysis
For the description of quantitative variables, it was necessary to express as the arithmetic mean and standard deviation. Regarding the comparison of the MHR between theoretical equations versus that obtained in the stress test, it was performed by ANOVA (analysis of variance one-way) to compare the differences of gender and age in the different variables studied. Also, post hoc test by Tukey test, to see the differences between the different age groups and anthropometry. In all cases the level of significance was set at 5% (p < 0.05); like the variables were correlated by Pearson's R and all analyzes were performed in Stata (Data Analysis and Statistical Software).
Results
After analyzing the data obtained during the fieldwork; which it was conducted with a total sample of 300 (181 women and 119 men) participants from the city of Cucuta, Colombia who attended the Rehabilitar Cúcuta IPS. Among the sociodemographic characteristics studied an average age for both genders of 26 ± 10 years identified; made up of 60% women and 40% men.
On the academic level, 58% were university graduates, 26% had studied up to high school, 9% were high school graduates, 6% were technical or technological and 1% had completed only primary. The risk factors identified were: blood pressure, overweight and/or obesity, diabetes, smoking, family history (diabetes, acute myocardial infarction and hypertension), alcohol intake and fatty foods; being most prevalent smoking, alcohol intake, overweight and/or obesity in men than in women and 93% of women eat many times month fast food, according to BMI the underweight, overweight and obesity was higher in men than women (Table III).
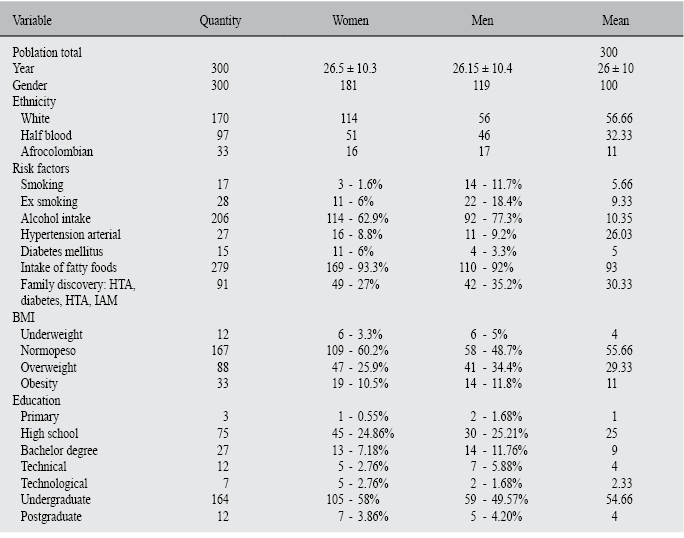
Moreover, we note that the stress tests performed were significantly high intensity for participants, since 80% (M: 84.03% versus W: 76%) mentioned an effort between strong and extremely strong (rating 5 to 10) after the stress test according to the Borg scale for fatigue; for the assessment of dyspnea 70% (M: 76% versus W: 63%) mentioned by the Borg scale dyspnea severe to extremely severe (grade 5 to 10) after the stress test.
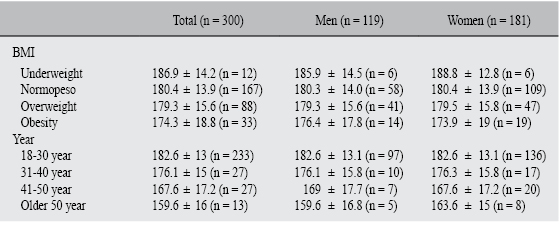
Likewise, the results of the stress test show similar values for men compared to women (178.49 bpm ± 16.64 versus 180.46 bpm ± 14.10; p = 0.272) (Table IV), and according to the BMI, the patients with underweight they reached a maximum heart rate of 186.9 bpm ± 14.2, normal weight 180.4 bpm ± 13.9, overweight 179.3 bpm ± 15.6 and obesity with 174.3 bpm ± 18.8 (p = 0.061) (Table V).

Similarly, it was determined that the equations with less arithmetic difference between the predictive equations for participants with underweight were the formula Morris (1 bpm, p = 0.434) and Graettinger (2 bpm, p = 0.567). Normoweight the equations of Morris (3 bpm, p = 0.123). And the participants with overweight or obesity were the equations of Morris (p > 0.05), Graettinger (p > 0.05) and 210-Age (p > 0.05) with an arithmetic difference between the stress test of 1 bpm (Table VI).

Similarly, by linking the age with maximum heart rate obtained in the stress test, it demonstrated in the study population that to older age less was his MHR obtained (18 to 30 years: 183 bpm ± 12; 31 to 40 years: 176 bpm ± 15; 41 to 50 years: 167 bpm ± 13; older to 50 years: 163 bpm ± 13; p < 0.001) (Table V). And the equations with less arithmetic difference respect to the beats per minute (blp) was Morris and Graettinger with 1 and 2 bpm respectively for the ages between 18 to 30 years. For ages between 31 and 40 years were the equations of Graettinger (p = 0.863) and 210-Years (p = 0.807) with less of 1 bpm of difference. In the group of the participants with ages between 41 to 50 years and older of 50, existed less arithmetic difference in the equation of Morris (p > 0.05), Astrang (p > 0.05) and Graettinger (p > 0.05) (Table VII).

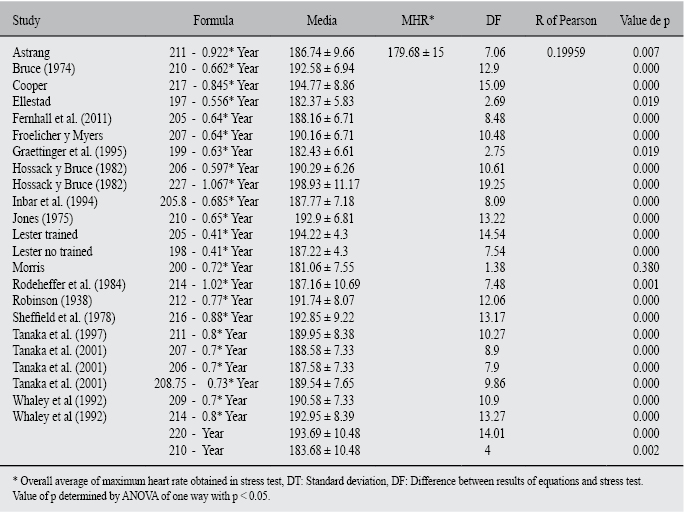
At the same time, the MHR obtained in a stress test was compared and determined by the equations, showing an overestimation by the equations up to 19 beats for minute. The equation 220-Age was not found valid and effective in determining the MHR, this formula obtained a difference in average of 14 bpm (p = 0.000) and Tanaka et al. (1997) and (2001) differences obtained 10 (p = 0.000) and 9 (p = 0.000) beats for minutes respectively. Accordingly, it is considered that the equations currently used to estimate the MHR are not accurate to prescribe ranges of heart rate training. Therefore, it was advisable to make a more specific analysis of correlation according to Pearson's R for the characteristics of the study population; this being a weak positive correlation (r = 0.19959) (Table VIII).
In reviewing the results of the analysis through ANOVA and by Tukey test was determined that only the formula of Morris (200-0.72 * Year) no significant differences with respect to a stress test with Bruce protocol in apparently healthy participants.
Discussion
The analysis of the results corroborates the various investigations that question the applicability of formulas to determine maximum heart rate.8,26-28 However, these equations are frequently used in hospitals, books and research. In addition, formulas and related concepts are included in most certification exams, exercise physiology and fitness. Despite more than 20 years that reveal the great error inherent in the estimation of the maximum heart rate (standard error of estimate 7-11 bpm)8 through predictive formulas.
Our results correspond partially to those reported by Chiacchio29 who compared the performance of formulas for MHR predicted by the equations 220-Age, Tanaka and Gellish; finding an overestimation of the HR in the younger subjects, while tended to underestimate the values in subjects 50 to 70 years. Like, he observed coincidence of the three formulas to 40 years.
One study,30 compared the MHR obtained through a tapestry, with estimated values by equations Jones21 and Tanaka et al.9 with a sample of 86 men, mean age 22.2 ± 3.9 years. The authors' conclusions are similar to those obtained in this research, not recommend the use of the equation Jones (MHR = 210-0.65 * Year).
But, the study considers accepTable equation of Tanaka et al. (MHR = 208.7-0.7 * Year), which is not recommended in this study for the population of this research, which showed a margin of error of 9 lpm. Also, a job31 made the same comparison of a stress test on treadmill versus 220-year. The values of MHR were obtained in the test 185.3 bpm ± 11.3 versus 188.7 bpm ± 12.3 obtained by the equation. Observed that the MHR calculated is significantly higher than obtained. These results are consistent with data obtained in the present study, in which 220-age equation overestimates the MHR for men and women.
Studies conducted by authors like Engels H.,32 Ricard R.33 y Robergs R.34 affirm and recommend in their research that should not be used 220-age equation as a means to calculate the MHR, as you could incur serious errors in prescribing exercise as much as in cardiac patients, as in apparently healthy people; suggestion is supported by the results presented in this research.
At the same time, Machado Fabiana y col.35 concludes that the equation "220-age" is not valid or appropriate because overvalued in average. Thus, and despite its widespread application, the formula "220-age" need samples to know its origin, author and age range used for processing, because the date is unknown.36,37
Conclusions
For the study population of the city of Cucuta, Colombia in the 25 equations evaluated to determine the maximum heart rate, no significant difference was found in the formula of Morris (200-0.72 * Year) (p = 0.380), therefore it considered appropriate to calculate the MHR in this population. However, we suggests conducting a stress test with the Bruce's protocol or Naughton for older people or with some degree of alteration where the Bruce protocol is contraindicated; for true maximum heart rate and no serious mistakes in planning training.
Furthermore, we identified significant difference in other equations evaluated; especially 220-Year, Hossack y Bruce (227-1.067 * Year), Cooper (217-0.845 * Year) and Lester (205-0.41 * Year) (p = 0.000) whose arithmetic mean differences were above 14 beats per minute. In turn, it is emphasized that in participants with lower BMI or younger, the MHR was much higher.
In addition, exist the need to continue this investigation in the coming years with a larger population to determine the most accurate and in effect creating an indigenous equation that meets the characteristics of the region is highlighted equation.

