











 text new page (beta)
text new page (beta) English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The amount of non communicable diseases like obesity, diabetes and hypertension keeps increasing in the world and managing them constitutes one of the main challenges to the development in the XXI century.
It is estimated that non communicable diseases, communicable diseases, mainly of cardiovascular nature, diabetes, cancer and obstructive pulmonary diseases caused 38 million of deaths in 2005, which is the 60% of the deaths worldwide. This is a growing problem in the developing countries, since the 82% of non communicable disease deaths is registered in the low and middle income countries. Approximately, 16 million of these deaths correspond to people under 70 years old.(1) It is predicted that this increasing in the chronic diseases frequency and the population aging will become a bigger challenge for the public health, in terms of register and monitoring, particularly for the primary level care.
In Mexico, according to the recent survey of Health and Nutrition 2012, the prevalence of the chronic diseases has kept growing from 1993 to 2010, from which obesity represents the 56%, diabetes mellitus 127.5% and hypertension 28.5%.(2) Based in this issue, and because of the growing population it is necessary to have a systematic and efficient electronic record that can provide current information about managing and monitoring of the chronic diseases. The epidemiological surveillance systems are key to obtain accurate information, because they collect true data through authorized instruments easy to be managed in their capture but with the scientific rigor that allows them to offer valid and useful information.(3) In the last years, healthcare systems have been using electronic records that facilitate the access and analysis of the information. Experience has shown that using the electronic systems to record the information has had an impact and success if they have the conditions to be done and developed.(4) International organizations in charge of the international monitoring of diseases like the World Health Organization says that a systematic verification and validation method must be used (STEPwise method) to monitor the diseases risk factors, morbidity and mortality.(5)
In Mexico, the Secretariat of Health has different recording systems which are the Health Information System (HIS); it was implemented less than 10 years ago; the National Health Information System (NHIS) and the OLAP cube system. The constraining factor of these systems is that the information is not updated because it is uploaded each month or the systematic auto validation is not feasible. Because of this, in the Health Organization policies and in the framework of the National Strategy for the Prevention and Overweight, Obesity and Diabetes Control, it was decided to modernize the current information systems in order to ensure the information quality and the appropriate monitoring of patients. It was established to implement the Information System on Chronic Diseases (SIC in Spanish), it is an information system that operates in the hybrid mode (offline and online) that allows the health staff record the attention given to the people with chronic diseases, including personal information, the results of the medical assessments (weight, glucose results, as well as the laboratory tests), the prescribed pharmacological and non pharmacological treatment.
This system was established in all the primary level care units since September 2014. This ambitious implementation was in charge of the Secretariat of Health, through the Sub secretariat of Health Prevention and Promotion, and conducted by the Disease Prevention and Control National Center, which took care of the operational deployment and remained in contact with the state and the judicial authorities. The Carlos Slim Health Foundation backed up the implementations with technical and technological deployment of the Information System on Chronic Diseases (SIC) and helped the health staff in all levels with the Help Desk available through a multichannel platform (telephone, mail and chat.) This will transform the concept of the records encouraging a more critical vision since it will be possible to see the advances, to draw and compare data of morbidity per medical unit, region and state with full access for all the staff.
Due to the importance of the consistency in the data, it was established a step by step evaluation system with the following elements: 1) the implementation of specific indicators that evaluate weaknesses and strengths of the record, people and supplies; and 2) the review of the medical record in its content and legal regulations. This will led us, in an immediate future, to design and establish strategies that improve the detection, control and management. This will give the opportunity of having these documents on time and properly done with valid data which for the public healthcare is crucial to take actions.
Because of the importance of evaluating and report the experiences and development of the implemented program or system, the objective of this study was to review the records of the Information System on Chronic Diseases (SIC) and its relation with the data registered in the chronic disease records like hypertension, diabetes mellitus, obesity, dyslipidemia and metabolic syndrome and their validation with the information in the clinical records.
Method
A transversal retrospective and correlational study was done. To calculate the sample of the cases to be reviewed it was used a probabilistic formula for random samples, in which N=pathologic frequency; k=1.96 reliability level of the 95% with a k of 5%.
It was obtained an N sample for diabetes of 758, for hypertension 761, obesity 756 and dyslipidemia 750 with a total of n representative n of 3,120 cases. To select the representative number of clinical records to be reviewed, it was done a stratified sampling by stages (Figure 1). First, proportional to the frequency of different pathologies and their distribution in the 13 sanitarian regions, where the number of records to be reviewed was defined. Second, the selection of medical units was made randomly and by list of the strata units and the units by health region resulting in 659 units to be reviewed. The selection criteria of the medical units were the following: they must have a record of patients with chronic diseases SIC; to have the number of registered patients for the sample of the records and assigned pathologies. It was decided to note down the day of the register and the calculation of the samples because the data of the SIC is modified every day. Finally, the selection of the revised records was done randomly using a list of random numbers. The selection of the units where the records were revised, was based on the total of n registered in the SIC (702 health units) and by the proportion of the diseases records by medical units of the health regions. This selection was convenient and had the following criteria: they must have access, a place to check the records randomly selected according to the prevalence of the chronic diseases (NCCD). A validated evaluation format of the records was used in a pilot sample with a repeatability and validity of 95% (r=90). This format was designed to be able to change the values to qualitative ones and then do a correlated analysis. The variables assessed for diabetes mellitus were: the number of subsequently consultation in the last 60 days; register of glycated hemoglobin in the last 12 months; the register of how many intakes he had a year; the report on the value of glycated hemoglobin (with HbA1C less that 7, between 7 and 9 and greater than 9); demographic data stratification by age and gender group, years of treatment and gender, and comorbidity and gender. The quality care was determined by the percentage of the basic measurements in the last consultation like weight, waist circumference, blood pressure (BP), glucose and foot examination, and the pharmacological treatment. In the case of hypertension, it was determined by the subsequently consultation in the last 60 days, number of patients with BP measurement, the BP less than 140/90 or equal to or greater than 140/90 mmHg; demographic characteristics by age and gender group; stratified by years, treatment and gender; patients with basic measurements in the last consultation (weight, waist circumference, BP and glucose); disease control by gender, disease control by comorbidity and disease control by years of treatment, pharmacological treatments, prescribed treatment to all patients: preventive ARAII plus diuretics, ARAII, basic antihypertensive drugs, ACE inhibitors. In the case of obesity, if they had consultation in the last 60 days; if they have the register of the body mass index (BMI); patients with BMI in control and with BMI not controlled. (Men control: with a size of < 1.60 cm the BMI less than 25 and if greater the BMI has to be less than 30. In women in control: with a size of < de 1.50 cm BMI must be less than 25 and if greater the BMI it has to be less than 30) Demographic characteristics of people with obesity, quality care: patients with obesity with measurements in the last consultation (weight, waist circumference, BP and glucose), disease control with comorbidity (diabetes, hypertension, dyslipidemia). In the case of dyslipidemia, how many they have had consultation in the last 60 days, patients percentage with record measurements of LDL cholesterol (LDL-C), with LDL-C greater or equal to 100 mg/dL; demographic characteristics stratification by age and gender group; stratification by years of treatment and gender; stratification by comorbidity and gender; quality care: patients with measurements in their last consultation (weight, waist circumference, BP and glucose); disease control by gender, comorbidity, years of treatment, pharmacological treatment (statins and fibrates)
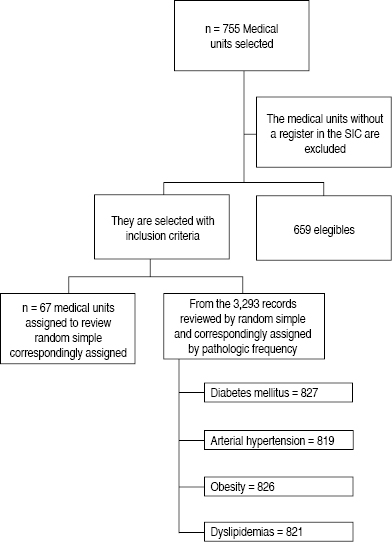
Figure 1: Selection process of the medical units and records in the 13 health regions of the Secretariat of Health of Jalisco.
Plan of Analysis
The data analysis was done using descriptive statistics, correlation of parametric data. The non parametric data was categorized correlating the frequency values reported in the Information System on Chronic Diseases (SIC) with the actions done based on the record. The correlation was used to explore the relation between the pathology recorded in the Information System on Chronic Diseases (SIC), also the appropriate register and the medical record, the management indicators in each pathology were reviewed. The level of statistical significance at α =.05 was established. Every single analysis was done in the program Statistical Package for the Social Sciences (SPSS) for windows 19. To check the validity of the data in terms of the quality care, it was reviewed the excellence in the chronic disease care; this also ensures the validity and reliability of the collected data. In order to do this, the following indicators were evaluated: completeness, which validated the empty fields in crucial variables like birth date, and affiliation number to the Popular Health Insurance. The data consistency validated that the prescribed treatment was consistent with the patient pathology. The data accuracy validated the non duplicity of patients and of the personal values like the affiliation number and address. The congruency was validated with the measurements to each patient. Based on this, the next indexes: (EI=meta (0.7 IV (veracity index) +0.3 QI (quality index), veracity and quality. All these indexes are referred and described in the website called Mexican Surveillance of Non Communicable Diseases(6) (Observatorio Mexicano de las Enfermedades No Transmisibles OMENT in Spanish).
Results
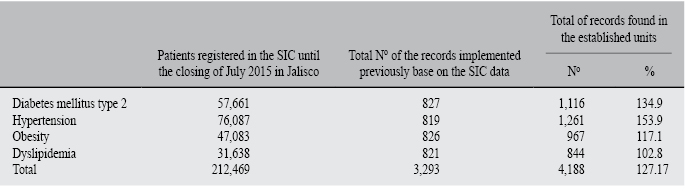
67 medical units were assessed, they were randomly selected from the 13 health regions in Jalisco State, with a total of 2,344 reviewed records within the period of a month (JULY). There were a total of 4,188 pathologies which were diabetes mellitus type 2, hypertension, obesity and dyslipidemia; the division of the reviewed records by pathology was like this: diabetes mellitus type 2 827; hypertension 819; obesity 826; dyslipidemia 821. The result of the records reviewed was as follows: diabetes mellitus type 2 (134.9% n = 1,116), hypertension (153.9%, n = 1,261), obesity (117.1%, n = 967), dyslipidemia (102.8%, n = 844) (Table I).
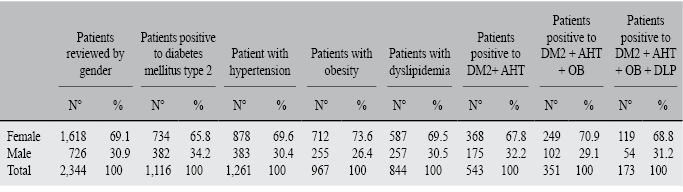
Table I: Description of the frequency in the chronic diseases and the amount of records reviewed and monitored.
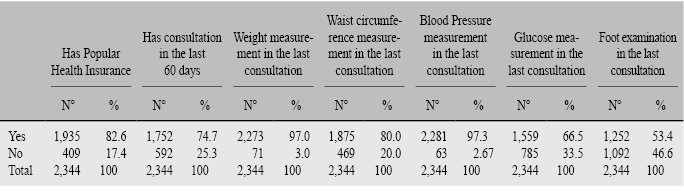
The basic measurements in the revision card were reviewed, they show that 82.6% (n = 1,935) of patients have Popular Health Insurance, 74.7% (n = 1,752) had a consultation in the last 60 days, 97% (n = 2,273) had a weight measurement, 80% (n = 1,875) had a waist circumference measured, 97.3% (n = 2,281) had the BP measured, 66.5% (n = 1,559) had the glucose measured, 53.4% (n = 1,252) had foot examinations (Table II).
Table II: Basic measurements taken in the last registered consultation of the patients with chronic diseases as core part in the control and management of the chronic diseases.
The gender prevalence was as follows n = 1,618 (69.1%) were female and n = 726 (30.9%) were male, demonstrating from the reviewed patients that there is more prevalence in the female. The diabetes mellitus prevalence was as follows 65.8% (n = 734) were female, 34.2% (n = 382) were males, for hypertension 69.6% (n = 878) females and 30.4% (n = 383) male. In the case of obesity 73.6% (n = 712) female and 26.4% (n = 255) male. Patients with dyslipidemia 69.5% (n = 587) and 30.5% (n = 257) female and male, accordingly.
The reviewed records were segmented into patients with two, three or four pathologies, this demonstrated that the diabetes mellitus type 2 and hypertension patients were 543 from which 67.8% (n = 368) were female and 32.2% (n = 175) were male. Patients with diabetes mellitus type 2 + hypertension+ obesity were found to be 351 from which 70.9% (n = 249) were female and the 29.1% (n = 102) were male. Finally, patients with diabetes mellitus type 2 + hypertension+ obesity+ dyslipidemia were 173, where 68.8% (n = 119) were female and the 31.2% (n = 54) were male (Table III). A comparative analysis of records to be reviewed (3,293) was done, it was proved that the referred pathologies were in fact the ones reported in the record. What it was found was that there were more records of the pathologies in the medical units (4,188) being not significant (p < 0.05). in the review of the records the presence of more than one pathology was found, which increases the pathologies but not the number of records registered. The diagram 2 shows how the quality, veracity and excellence indicators are automatically plotted for comparative purposes of the 32 Mexican states and with average results nationally. The diagram 3 summarizes the control model and the follow up of the chronic diseases indicators which are registered every day and for each patient, and which is reported in culmed medical units.
Discussion
This study shows the importance of having and electronic record system of the chronic diseases to control and manage them in a dynamic way and with data quality indicators. It was able to determine the consistency chronic pathologies electronic record, like diabetes, obesity, hypertension and dyslipidemia and their management; as well as the information in the clinical records of the medical units that offer a first level care for the chronic diseases which gives quality and valid data.
This report rectifies the gap in the health information systems of the chronic diseases with validated indicators that can be found in other health systems. This electronic health information consists of four important categories which are: general characteristics, quality care, disease control and pharmacological treatment; it also includes the immediate report of the forth mentioned characteristics in the tables and figures and the indicators report on the quality, veracity and excellence evaluation nationally and between the 32 Mexican states. This indicators help in the assessment and functionality of an information system for the policies, planning, institutions and human resources, and in the financing and infrastructure.
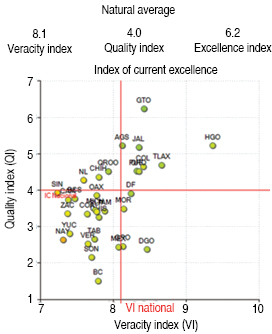
Figure 2: Excellence, veracity and quality index in the attention of chronic diseases where it is shown the national and state results, where the analyzed state (Jalisco) it is in the fourth place worldwide.
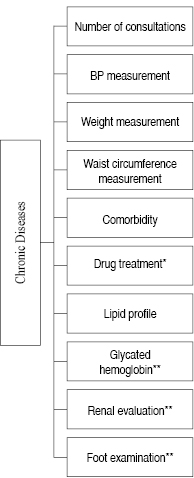
Figure 3: Monitoring model of the management and control of chronic diseases indicators in the Information System on Chronic Diseases (SIC) *Drugs according to the pathology, **This measurements are only reported in patients with diabetes mellitus diagnosis.
It also helps to promote heterogeneity of the data and facilitates the comparison by regions, states and with other countries, especially in Latin-America where in previous studies an analysis of the health systems was carried out. It showed that even when the Latin-American systems are heterogeneous in their indicators, Mexico and Costa Rica had higher indicators.(7) All of this shows the great potential an electronic system has to make comparisons in health indicators ad if it is kept updated and improved, it will give us information according to the current needs. The importance of having the data in an electronic way in all the country, is that we will have the opportunity of making data comparisons with other information sources like the Latin-American Network for the Strengthening of the Health Information System known as RELACSIS(8) in Spanish, which is a longitudinal Latin-American repository, generated in one or more medical care encounters.
The electronic record includes demographic data of the patient, the evolution or case notes, problem lists, or diagnosis, drugs, vital signs, lab result similar to the reported in this system among others. This will help the comparison of the patient care quality, the doctor management; it will help in decision making based on evidence, quality management and the report of the clinical care results. Having an electronic system in health care has implications and benefits in at least three basic points: 1) Gives essential elements for the diagnosis to the health policy makes, 2) to the professionals in health care and 3) their patients and their management. For the policy makers in health issues, it can be used as an exclusive surveillance system in important public health problems as the chronical diseases are, also as a demonstration of the qualities and risks of having a record, for example it was able to prove the existence of a sub record of pathologies, because there were more pathologies found in the medical units than in the ones registered in the system. With this is possible to maintain a quality in the data. The other advantage is that it can be consulted by anyone because is an open system, it gives transparency and it is easy to be monitored by the health staff. This will help to the responsible managing the chronic disease patients that are being checked based on the quality care model defined by the number of consultations and basic measurements in the last consultation that are at least five in the chronic diseases plus HbA1C in diabetes patients and the drug treatment offered to the patient (Scheme2). These measurements have been reported as indicators of an adequate technical quality of the attention and good control of the chronic diseases.(9)
The second strength that involves the health care professionals is the evaluation of the quality care using as an indicator the number of consultations a patient had. This is key, because one of the criteria of quality was established by the number of consultations the patient had and the quality of them based on the basic measurements that the doctor or the health staff took from the patient. Moreover, is one of the essential indicators because the periodic consultation is a bilateral interest, major control and above all a bigger chance of offering education, motivation and support which will allow having a better control of the disease, also its prevention. It will gradually change from more consultations to have more control to fewer consultations with the controlled patient. This will be an indicator not only of the quality care but also in the medical care costs (staff working hours, supplies, drugs, etc). In this sense, previous analysis claim that the total of consultations has been reported as an indicator of the technological efficiency of the patient care, it was even reported that together with a patient from the metropolitan area the efficiency in service provision was favored regardless the patients attributes or the age of the doctor.(10)
The third strength in the patients management is that it helps indirectly to improve the treatment adherence understanding by it, the active collaboration between the healthcare professional and the patient in the decision making that affects his own health and which is based on patients consent. Based on this definition the agreed recommendations with the health care professional in this system were the basic measurements taken and reported like weight, waist circumference, BP, glucose, foot examination and glycated hemoglobin. To evaluate more precisely the adherence it is required to record more indicators of an active collaboration of the patient in the management like the follow up of the diet and the changes in his life style; as well as the evaluation of other essential factors of the adherence that are related to the patient, to the drug, to the disease itself and to the health care professionals. It is worth pointing out, that in this review only one element of the adherence promotion is addressed, but there are many other factors that determine the adherence like educational, behavioural, technical, of social and family support as it has been cited previously.(11) In this same way it will give us elements to evaluate the service quality through a patient satisfaction measurement, because if a patient is satisfied with the service he will be more willing to follow the medical recommendations and to improve his health, as it has been previously proved. Specific perception and assessment indicators are already reported in the satisfaction elements such as the facilities, organization and health staff and medical performance.(12) On the other hand and very importantly are the economical implications that the adherence can generate, especially in the chronic diseases, for example, it has been reported that the diabetes and hypertension are the diseases with a higher rates of non compliance.(13)
All the reflections agree that considering the healthcare quality as a strategic practice, specifically focused on actions and achievements, where the medical practice could be benefited facing the challenges that emerge in the daily tasks in the treatment adherence of chronic diseases non communicable, which is a serious worldwide problem that has two direct consequences: a decreasing in the healthcare results and an increase of the healthcare costs. To be clear, if we want the patient to have a good perception of the healthcare attention, it is important to give the appropriate treatment, and even if this is not possible for any other reason, make the patient feel properly taken care of, he will leave the healthcare center satisfied and consequently his treatment adherence will improve.
A last operational strength is that in the country the system already has a regulation for the electronic record of health data,(14),(15) which immediately gives a legal framework and allows it to be established as an official program that all states can follow and it also ensures its application. A part from the regulation this program has veracity, quality and excellence indicators that are given automatically and are shown immediately and comparatively.
There were several constraints in the study. In the operational aspect, there were some difficulties with the speed of the updates and selection of the information registered electronically which had been slower than the Health Information System (HIS), previously established. This has depended on the electronic system and the updates of their operational versions. The other constrain was generated by the complexity and the link that it exist with the presence of the chronic diseases, because many of them can be present in one single patient and in the system was registered as co morbidities, and that can affect the diseases record and its relation with the number of files. This happen because in this stage the pathology record is limited to only five pathologies (metabolic syndrome is not included)and it are convenient that this existent and significant combination of the chronic diseases could be registered.
As any implementation process it has its regulations, in the future e will have to regulate and evaluate the constraints that we found in the starting point. Experiences in other countries with the electronic information access has been analyzed, like the one in Brazil with their National Policy of Health Data and Information Technology (PNIIS) and from a qualitative analysis perspective report that the implementation of a national policy of health data and information technology requires to consider the constrain factors like a poor infrastructure, few human resources and a technological gap.(16)
As learning lessons we can conclude that:
An electronic health record system facilitates the organization of the population and patients medical data in order to promote an efficient and effective attention, making easy the planning and identification of sub population with special needs and the attention management of a comprehensive medical care.
We propose that in order to have a more complete record more variables be included like vaccination, medical care profile, life style management, case conference among other aspects that are necessary to be included like in other countries has happened,(17),(18) but without the risk of having too much information in the system. If we do this the data and the records will have a better quality. This process is a unique opportunity to assess systematically and with valid indicators the control and management of the chronic diseases.
As any other electronic information system it has been changing to improve the health care with quality that the patients need. To obtain that objective we propose to finish with the homologation of the medical care and healthcare services, in order to answer appropriately and efficiently the needs in the treatment adherence of the chronic diseases non communicable. The quality must be shown in each diagnosis and treatment that are carried out in each health care.
In the social management of the Secretariat of Heath there is the creation of the public value of the information system on chronic diseases SIC by the management that proposes to optimize the performance of all this efforts. The information system on chronic diseases is the answer of a provider to his user to the problem of the chronic diseases and the big challenge consequently is to improve the treatment adherence by improving the perception of the patient in the first level care.
It is necessary a continuous performance evaluation of all the system of the electronic record system to have a better impact in the management of the chronic disease, as well as in attention quality indicators like the costs in the health care, especially in the complications of the diabetes and hypertension costs.

