










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkFrontera norte
versão On-line ISSN 2594-0260versão impressa ISSN 0187-7372
Frontera norte vol.34 México Jan./Dez. 2022 Epub 10-Fev-2023
https://doi.org/10.33679/rfn.v1i1.2300
Articles
City and COVID-19: Accessibility of the Older Adult Population to Medical Units in Chimalhuacán, State of Mexico

1El Colegio Mexiquense, México, krojas@cmq.edu.mx
2El Colegio Mexiquense, México, tchavez@cmq.edu.mx
3El Colegio Mexiquense, México, cfgarrocho@gmail.com
COVID-19 confronts healthcare systems with an enormous demand for services. A large part of the affected population is vulnerable due to their age, comorbidities, and socioeconomic status. The objectives of this research are: 1) to estimate accessibility to public primary care units for older adults in Chimalhuacán through walking transfers, and 2) to identify the locations that increase, to a greater extent, the accessibility of this population to new primary care units. The proposed methodology combines two methods to achieve a more accessible, efficient, and equitable socio-spatial distribution of the healthcare system for older adults in a dense urban Mexican municipality. The results reveal inequalities in the accessibility of this group to healthcare units, and a local solution is proposed by increasing the service with six new facilities. The conclusions synthesize the main findings and limitations of the work, suggesting lines of research.
Keywords: COVID-19; accessibility to health services; older adults; Chimalhuacán; State of Mexico
El COVID-19 enfrenta a los sistemas de salud a una enorme demanda de servicios. Gran parte de la población afectada es vulnerable por su edad, comorbilidades y condición socioeconómica. Los objetivos de esta investigación son: 1) estimar la accesibilidad a unidades públicas de atención primaria de los adultos mayores en Chimalhuacán mediante traslados caminando y 2) identificar las localizaciones que incrementan en mayor medida la accesibilidad de esta población a nuevas unidades de atención primaria. La metodología propuesta conjuga dos métodos para lograr una distribución socioespacial del sistema de salud más accesible, eficiente y equitativa para los adultos mayores en un municipio urbano y denso de México. Los resultados develan desigualdades de accesibilidad de este grupo a unidades de salud y se propone una solución locacional incrementando el servicio con seis nuevas instalaciones. Las conclusiones sintetizan los principales hallazgos y limitaciones del trabajo, sugiriendo líneas de investigación.
Palabras clave: COVID-19; accesibilidad a servicios de salud; adultos mayores; Chimalhuacán; Estado de México
INTRODUCTION
Older Adults: A Priority Group During a Pandemic
In Mexico, the damage caused by COVID-19 among the elderly population (60 years and over) evidenced the weakness of the healthcare system (Welti-Chan & Ramírez, 2021). This demographic group, the most vulnerable to the pandemic (Vega Rivero, Ruvalcaba, Hernández, Acuña, & López, 2020), frequently suffers from chronic diseases such as obesity, hypertension, and diabetes (Von Seidlein, Alabaster, Deen, & Knudsen, 2021), which increases their probability of becoming seriously ill and losing their lives if they contract the COVID-19 virus4 (González, Orozco, Samper, & Wong, 2021).
In addition to the comorbidities associated with age, older adults usually suffer a progressive decline in their physical functions, their daily space is compacted, their income decreases, their family and social networks are weakened (Montes De Oca, 2010). Low-income older adults,5 even those with pension funds, are not able to reach sufficient economic income and many continue to work informally (Inegi, 2018; Welti-Chan & Ramírez, 2021). All this affects their accessibility to health care services and their timely consumption (Garrocho Rangel & Campos Alanís, 2016).
When speaking about consumption, microeconomics shows that the higher the price of a good or service, the lower the quantity demanded (Karlan & Morduch, 2019). This vision is non-spatial and supposes homogeneous prices in the area. This changes when the spatial dimension is introduced, then consumption is directly related to accessibility and the concept of real price, which is the sum of the market price of the good or service at the point of supply plus the cost of transportation to access it (O’Sullivan, 2019). That is, even if the price of the service at the supply points is the same, the real price varies in the area, because the cost of transportation to the supply point is not the same for all, since it’s modified according to the location of suppliers and consumers. This is not covered by traditional microeconomics. When the cost of the service is free or close to zero, the only cost of the real price that the consumer faces is the cost of transportation (even if it is done on foot), which is one of the most important ones for the older adult population (Garrocho Rangel & Vilchis Mata, 2021).
The vulnerability and growth of older adults requires the city to rethink its territorial strategy of basic services and facilities (Bosch Meda, 2013). The purpose is to achieve inclusive, efficient and equitable spaces in the socio-spatial distribution of resources, including health (Garrocho Rangel & Vilchis Mata, 2021). In the year 2020, 11.3% of the total population of Mexico corresponded to the elderly population, and its growth trend is the fastest of all age groups (Inegi, 2020).
From a geographical perspective, the basic determinants of health care for low-income older adults are the availability and pedestrian accessibility of medical units6 (Mollenkopf, Hieber, & Wahl, 2011). This group is forced or prefers to get around on foot: many do not have a car, cannot afford the cost of using a taxi, and avoid the dangers of using public transport (Mattioli & Schneider, 2020). Walking generates autonomy, independence and it’s even a form of exercise (De Alba González, 2017). During the pandemic, various institutions recommended traveling on foot to avoid crowds on public transport, a risk factor for infections (Von Seidlein et al., 2021).
There is evidence that in Mexico the distribution of health care units does not adjust to the maximum average comfortable walking times for older adults (Garrocho Rangel & Campos Alanís, 2006). Research in Latin America and Mexico shows that the comfortable walking speed of a 60-year-old person in good health corresponds to:7 0.98 m/s +/- 0.78 m/s in Chile (Rybertt, Cuevas, Winkler, Lavados, & Martínez, 2015), 1.31 m/s +/- 1.03 m/s in Uruguay (Sgaravatti, Santos, Bermúdez, & Barboza, 2018), 0.92 m/s +/- 0.24 m/s in Peru (Varela, Ortiz, & Chávez, 2010) and 1.00+/-0.24. m/s in Monterrey, Mexico (Enríquez, Cruz, Celestino, Garza, & Salazar, 2013).
What Implications does Physical Accessibility have in Primary Health Care for the Prevention of Damage by COVID-19 in Older Adults?
Accessibility to health care units is particularly important for older adults living in poverty8 who usually make their daily trips on foot (Gutiérrez Robledo & Kershenobich Stalnikowitz, 2015). Usually, this group suffers loss of speed and endurance (Lenardt, Setlik, Pereira, Lourenço, Barbiero, Betiolli, & Rodríguez, 2021), and they are more affected by the poor condition of the streets, the lack of sidewalks, the poor quality of public transport and social isolation, which affects their quality of consumption (Garrocho Rangel & Ramos Pérez, 2019).
Quality of consumption of health care services refers to the adequate quantity, frequency, and opportunity of consumption, according to the conditions of the consumer (for example, age, weight, health status) and to the standards of the specialists (doctors). The quality of consumption allows giving nuance to the principle of microeconomics that says “at lower cost, higher consumption, and vice versa” and expresses it as: at lower cost, higher quality of consumption, and vice versa (Garrocho Rangel & Ramos Pérez, 2019).
Accessibility to primary health care impacts the health, care costs, and functioning of older adults (Guida & Carpentieri, 2021). In terms of health, it accelerates the prevention, detection, monitoring and treatment of diseases. During the COVID-19 pandemic, it has been seen that accessibility facilitates the opportunity for timely diagnoses, case detection, contact tracing, and hospital and home isolation (Rasanathan & Evans, 2020). Adequate accessibility reduces all kinds of costs borne by the patient and their relatives when traveling between their home and the health care unit (Álvarez, García, & Londoño, 2016).9 Socially, it favors the autonomy of older adults who don’t necessarily require accompaniment to medical appointments, considering that they often live alone (Huenchuan, 2020). In addition, it facilitates the participation of organized communities around the social determinants of health, generates equitable, safe and healthy areas, with an emphasis on vulnerable groups, such as the population aged 60 and over (Giovanella, Vega, Tejerina, Acosta-Ramirez, Parada, Ríos, Iturrieta, Fidelis de Almeida, & Feo, 2021).
For this demographic group in poverty, having health care services accessible on foot is a way to prevent and mitigate their exposure to pathogens associated with their daily activities and a key element to improve their well-being (González et al., 2021; Vega Rivero et al., 2020). Pedestrian access to the healthcare system on walkable routes is a way to guarantee care for all older users, even under pandemic conditions (Guida & Carpentieri, 2021). Achieving this requires urban planning and management methods and processes that contribute to avoiding areas with poor access to health care services (Galindo Pérez & Suárez Lastra, 2018; Garrocho Rangel, Chávez & Álvarez, 2020). From an inclusion, safety, and health perspective, these areas should be a priority in urban planning and in strengthening healthcare services to deal with pandemics (Nyadera, Onditi, Obimbo, & Muchina, 2021).
Measuring accessibility in the intra-urban space is not easy (Garrocho Rangel & Campos Alanís, 2006). There are no exact aggregation methods, what we have are approximate aggregation methods that are reliable for decision making (Hooper, Foster, Nathan, & Giles, 2012). The method of measuring accessibility to health care units used in this work is the Two-Step Floating Catchment Area (2SFCA) (Luo & Whippo, 2012). Due to its internal consistency, it is widely accepted in literature, an example of which is the work of Luo and Wang (2003). This method will make it easier to reveal socio-spatial differences in accessibility consistent with the pedestrian reach of older adults and discover areas that need to be better tended to (Guida & Carpentieri, 2021). Its supplies are simple and cheap to obtain (Tao, Cheng & Liu, 2020).
The 2SFCA method considers that the availability of services in health care units does not only depend on their location, but also on their size (Luo & Whippo, 2012). The most used indicator to dimension this factor is the number of doctors and nurses in contact with the patient (Rojas & Aguilar, 2021) and the number of beds (Pérez Valbuena, 2015). These indicators are in proportion to each other. Here the most useful data for this text was considered: number of physicians in contact with the patient.
Health Care Units: Strategic Element of Medical Care
The locational (or spatial) planning of healthcare systems (public and private) proposes to minimize the costs of interaction10 between supply and demand (Brizan & Juel, 2022). Achieving accessible health care services through walkable routes compensates, in part, the physiological and social losses of older adults and raises their quality of consumption (Álvarez, Trujillo, & Garrocho, 2018; De Alba González, 2017).
The inclusive location of health care units requires balanced location solutions in terms of efficiency and socio-spatial justice (Simmons, Garrocho, Kamikihara, & Campos, 2018). Given the complexity of the problem, planners often rely on location-allocation models.11 These mathematical models operationally translate principles and objectives of philosophy and public policy associated with the socio-spatial distribution of opportunities (Harvey, 2010).
The model applied in this text is the so-called P-Median with maximum travel distance restricted to health care units (Buzai & Baxendale, 2008). This model prioritizes care opportunities for the population with lower accessibility, combining efficiency and equity criteria. Its objective function is to reveal potential locations of health care units that minimize the total distance traveled by the population to access the service (efficiency criterion); ensuring that no one has to travel more than a certain distance to achieve it (socio-spatial justice criterion) (Harvey, 2010). Standardized mobility distances are commonly used (Buzai & Baxendale, 2008).
In what follows, the text is divided into five sections. The first two establish the basic conditions of the study: the research objectives and an analytical description of the study area. Then we proceed to detail the methodology that articulates two socio-spatial methods: one that allows measuring the levels of accessibility of older adults to health care units with walking transfers on a block scale-known as the Two-step Floating Catchment Area-, and another that assesses the locations of new units combining criteria of efficiency and equity―the so-called distance restricted P-Median Model―. Subsequently, the results are presented. The central elements are the levels of accessibility of older adults to health care units, the local solution proposing an increase of six new units to the system of the study area, and the benefits of this solution in terms of accessibility, covered population and transportation costs. The final section―conclusions―summarizes the main findings and limitations of the work and suggests lines of research. The article closes with a reference list.
OBJECTIVES
The objectives of this research are: i. to estimate accessibility to public primary care units for the older adults in Chimalhuacán through walking transfers and ii. identify the locations that most increase the accessibility of this population to new primary care units, ensuring that no one has to travel more than a certain distance to reach it.
Area of Study
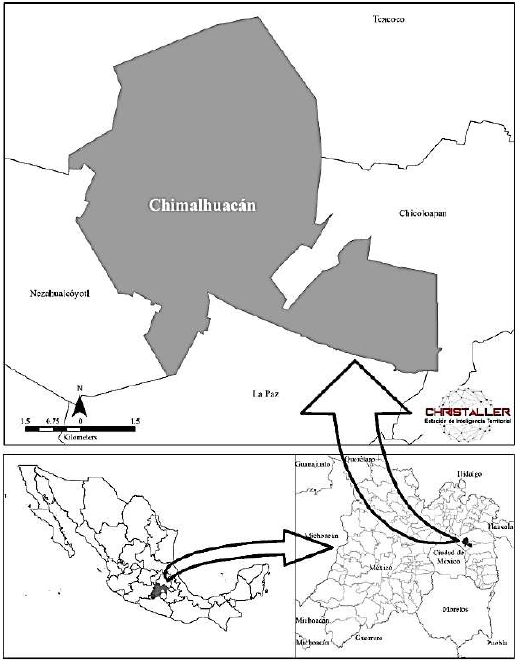
Chimalhuacán is a municipality that is part of the Metropolitan Area of the Valley of Mexico (MAVM), the most populated city in the country (Map 1). It has 705 193 inhabitants. It is the municipality with the largest population in the eastern region of the MAVM, and the one with the majority of older adults: 59 108 inhabitants, that is, 8.4% of the total population (Inegi, 2020). It has an extension of 5 413.6 hectares with a density of 130 inhabitants each (Welti-Chan & Ramírez, 2021).
The area of study is made up of the polygons of urban blocks of the municipality of Chimalhuacán. The target population is that of 60 years and over in each block. To quantify it, the geostatistical framework for the year 2020 was considered, to which the information on the results per block of the 2020 Population and Housing Census is linked. A population of 58 794 and 4 684 polygons were considered (Inegi, 2020).
Chimalhuacán is an urban and dense municipality that suffers from general conditions of poverty (Government of the State of Mexico & H. Ayuntamiento de Chimalhuacán, 2019; Coneval, 2015). It has high indicators of lack of healthcare services and is highly vulnerable to COVID-19 (Secretaría de Salud, 2021a, 2021b). As of April 15, 2021, 957 accumulated deaths had been registered in the municipality since the beginning of the pandemic (Secretaría de Salud, 2021b). Its impact rates by deaths and mortality due to positive cases of COVID-19 are higher than the national average, and are around the average calculated for the State of Mexico (Christaller, 2022b). The calculations were made within Christaller: Territorial Intelligence Station (Chávez Soto & Garrocho Rangel, 2018).
At the AGEB scale (Basic Geostatistical Area) the territorial homogeneity of poverty in the municipality is observed.12 According to data reported by the National Council for the Evaluation of Social Development Policy (Coneval): in 2015 123 of the 137 AGEBs in the municipality registered more than 50% of their population in conditions of social backwardness,13 and out of the 40 AGEBs, 70% of its population was identified under the same conditions (Coneval, 2015) (Map 2).

Source: Own elaboration based on Coneval (2015).
Map 2. Percentage of population with social backwardness in Chimalhuacán, State of Mexico by AGEB, 2015
The older adults in Chimalhuacán are considered highly vulnerable to the pandemic due to their density, but also due to the allocation and location of healthcare services. The municipality faces a high deficit of medical services: it has 12 universal health care clinics in which there are 72 offices and 113 doctors, that is, around 0.16 doctors for every 1 000 inhabitants in the municipality, while the WHO recommends three doctors for every 1 000 inhabitants (Senate Gazette, 2016) and the OECD registers 3.5 doctors for every 1 000 inhabitants (OECD & WB, 2020).
In Chimalhuacán, the Secretariat of Health (SH) is the most important public and universal access system that provides healthcare services. More than 30% of the inhabitants state that it is their main alternative for healthcare, followed by private clinics attached to commercial pharmacy chains (28.1%) (Inegi, 2020). Therefore, in the present investigation, the SH medical units were considered as the main supply points of the municipality. These medical units, in addition to offering medical care, generate statistics and monitor the health situation at the individual level with an emphasis on the older adults in nearby territorial microscales, something that private clinics do not do (Giovanella et al., 2021). In 2020―year of the last population census―, the SH website reported 12 medical units established in Chimalhuacán (Secretaría de Salud, 2021a).
METHODOLOGY
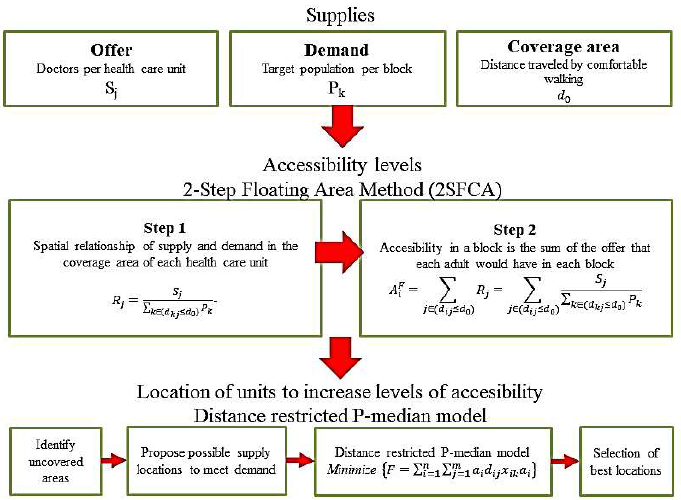
The calculation process is described next. Detailing both the calculation of the level of accessibility―through the Two-Step Floating Catchment Area Method (2SFCA)―to identify service coverage in the study area, as well as the application of the distance restricted P-Median Model to evaluate proposals for new medical units in uncovered areas (Figure 1).
Source: Own elaboration.
Figure 1. Process of locating service units through the calculation of accessibility levels
Two-Step Floating Catchment Area Method: Spatial Demand-Supply Relationship
The 2SFCA method considers demand mobility thresholds: the older adult population. The threshold we used here was a preferred walking speed of 1.05 m/s (see introduction). The debate is open about the advisability of trips to basic facilities in the city being around 15 minutes on foot (Descant, 2021; Sansão Fontes & Espósito Galarce, 2021). This might be recommended for older adults (Smith, 2020). Here the distance or radius of coverage of the health care units is:
This threshold is a guide. Its usefulness lies in the order of magnitude it establishes, not in its precise value. In practice it could be a little less or a little more: one must not fall into the mirage of accuracy. In this document, 945 meters is the approximate limit to consider for a person who moves on foot to access a health care unit.
Step 1
For each health care unit with a certain number of doctors (j), identify the population (k) that is within the threshold or radius of coverage (d0) of location (j) and calculate the ratio of doctors/target population (Rj) within the area of influence of (j) (Chen & Jia, 2019).
The result of this step is the supply/demand ratio (doctors per target population) in the areas of influence of the health units, taking into account the number of physicians and the magnitude of demand located in the blocks covered by each unit. In mathematical terms it is expressed as:
where Pk is the target population (PO) in block k, whose centroid is within the radius of influence d0, Sj is the number of doctors in health care unit j, and dkj is the distance (or transportation cost) between k and j.
Step 2
This phase is similar to step 1, but the calculations determine reach areas from the centroids of each block, taking as a parameter the radius of 945 meters. The result of step 2 is the proportion (target population attended by doctors) in the areas covered by each block, taking into account the magnitude of PO and the number of doctors in the health care units within a radius of 945 meters. In this step, the range areas move or float from block to block until they are all covered.
Step 2 is synthesized as follows: for each location of the target population (i : the centroid of each block), identify all physicians from health care units j who are within the coverage threshold or radius d0, from location i and add the physician/target population ratios Rj for all locations i (Chen & Jia, 2019; Luo & Wang, 2003):
The higher the AiF value, the greater the accessibility of each block where the target population lives.
Distance Restricted P-Median Model (Efficiency and Spatial Equity)
The distance restricted P-Median Model considers that given a limited number of facilities to be installed, the service locations that cover the largest population must be identified without users having to exceed a set maximum travel distance.
Thus, the objective function F of the model can be expressed as follows: identify the locations that minimize the total distance traveled by the older adult population from start (the centroids of the blocks) to the closest destinations (the potential health care units) di, ensuring that no one has to travel more than a certain maximum distance S to reach a destination.14 The demand is allocated to the closest unit, minimizing spatial inequalities.
In mathematical terms, the objective function is expressed as follows:
where ai is the weight associated with each point of demand (the 60-year-old population that inhabits those blocks), dij is the distance between the demand point i and the supply point j, x i is the allocation factor: 1 if supply point j is the closest to demand point i and 0 otherwise, n is the number of demand points and m the potential supply points and existing units.
In this research project, 68 properties that meet the specifications for a health care unit to be located in them were identified.
VARIABLE PROCESSING AND SOFTWARE
Transportation Costs
Transportation costs were estimated using Euclidean distances from the centroids of the blocks to primary care units. In other studies of accessibility to health care services, the estimates are made through the road network (Guida & Carpentieri, 2021; Rojas & Aguilar, 2021). However, Garrocho Rangel et al. (2020) have verified that it is not worth unnecessarily complicating the analysis in order to pursue the mirage of precision: the correlation between the Euclidean distances and the distances along the roads in various locations in Mexico is R2=0.934. In operational terms, it is practically the same to use Euclidean distances or distances along roads.
Software
For data processing and presentation of results we used Christaller: Territorial Intelligence Station (Chávez Soto & Garrocho Rangel, 2018). This platform allows integrating concepts, theories, methods and data in accessibility analysis studies. Christaller provides various models implemented in free software tools that operate with Geographic Information Systems on different platforms (for example, ArcGIS, Qgis) (Garrocho Rangel et al., 2020).
RESULTS
Current Distribution of Supply and Demand
The demand: older adults in Chimalhuacán, State of Mexico
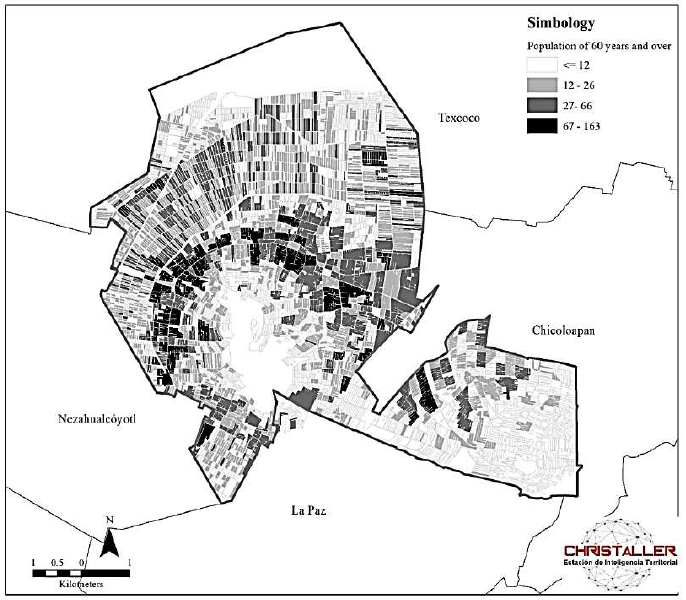
The spatial distribution of the population of people aged 60 and over in Chimalhuacán is similar to that of other Mexican localities: it is concentrated in the oldest and most consolidated areas of the municipality and is reduced in the periphery (Álvarez et al., 2018). This is confirmed if the study area is observed at a block scale (Map 3). The blocks with the highest number of older adults (67 to 163 older adults per block) are located in the foundational areas of Chimalhuacán.
Source: Own elaboration based on Inegi (2020).
Map 3. Total population aged 60 and over per block in Chimalhuacán, State of Mexico, 2020
On the contrary, the areas with a low concentration of the older adult population (and a high concentration of the young population) are located in areas of recent expansion, where land is less expensive (Garrocho Rangel & Campos Alanís, 2016). In the lower part of the Chimalhuache hill, average values of between 12 and 66 older adults per block are identified, while, to the north of the municipality, at the top of the hill and in the area of Ejido Santa María, which are recent human settlements, the lowest number of older adults per block is observed: four older adults on average (Map 3).
The Supply: Distribution of Primary Care Units
According to international standards, in Chimalhuacán the supply is insufficient to meet the demand. What happens to its location in relation to demand? Only three health care units correspond to the spatial distribution of demand: the San Lorenzo Municipal Health and Community Welfare Center, the San Pedro Health Care Center, and the Acuitlapilco Specialized Center for Primary Health Care. Meaning, only a quarter of the health care units in the municipality are located in a way that is consistent with the territorial distribution of demand. The damage caused by the COVID-19 pandemic shows that this situation must be corrected, especially if a premise of the federal government is to prioritize healthcare to the most disadvantaged population.
The pattern of urban expansion in Chimalhuacán is very complex: accelerated, discontinuous, in high risk areas, largely irregular, and with widespread poverty. This makes it highly vulnerable to mass spread diseases that could be prevented and reduced from primary care medical units. The existing healthcare resources in the municipality are insufficient in size and deficient in their location. Its correct planning is quite a challenge, as we will see below.
Pedestrian Accessibility of the Older Adults to Primary care Medical Units
Let us remember that the values of the Accessibility Indexes (AiF) are valuable due to their order of magnitude and allow comparisons to be made between areas over time and are used to measure the impact of policy actions. It is difficult to compare AiF with different studies, because the specific services and target populations vary. To facilitate comparisons, in the present investigation, the Accessibility Indexes (AiF) were multiplied by 1 000.
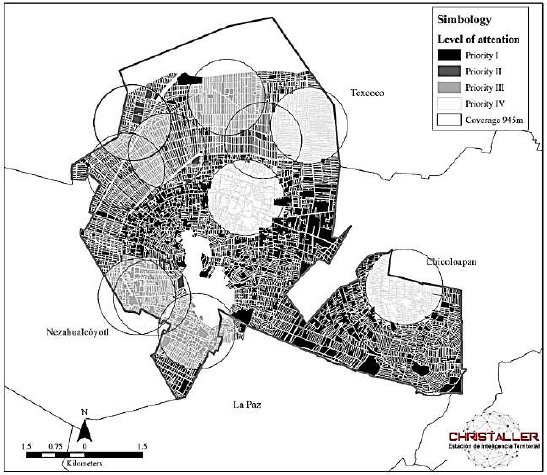
The minimum and maximum values of the Accessibility Indexes were 0.0 (healthcare deserts) and 13.04 associated with areas with very high healthcare. The accessibility average was 2.2 and the standard deviation 3.5. These values indicate huge inequalities of access; with them, the blocks of Chimalhuacán were classified into four levels of attention priority, and the population at each level was quantified (Maps 4 and 5).
Priority I. Healthcare deserts15 (AiF = 0.0): 2 392 blocks, 22 973 older adults, 39% of the total number of older adults in the municipality.
Priority III. Blocks above the municipal accessibility average (AiF > 2.2) up to the upper standard deviation (AiF = 5.7): 971 blocks, 16 267 older adults, 27.7% of the total number of older adults in the municipality.
Priority IV. Above the upper standard deviation (AiF > 5.7): 650 blocks, 8 227 older adults, 14% of the total number of older adults in the municipality.

Source: Own elaboration based on Inegi (2020) and Ministry of Health (2021a).
Map 4. Accessibility index to primary care units in Chimalhuacán, State of Mexico
Source: Own elaboration based on Inegi (2020) and Ministry of Health (2021a).
Map 5. Blocks by level of attention priority in Chimalhuacán, State of Mexico
Proposal for the Location of new Primary care Medical Units: Application of the Restricted P-Median Model
This section presents a planning scenario elaborated with the results of the two models described in the methodology. The opening of six new health care units is considered from the 68 properties that meet the specifications.16
Therefore, the challenge is to reveal the six properties that minimize the total distance traveled by the 58 794 older adults from where they reside (the centroids of the 4 684 blocks) to the closest destinations (the 12 existing health care units, plus the six that would be installed) (dij), ensuring that no one has to travel more than 945 meters (S) to reach a health care unit. The demand is allocated to the closest unit, minimizing spatial inequalities. The proposal was discussed with state and municipal officials, it is realistic in financial and operational terms.
Properties that Best Meet the Objective Function: Locational Solution
The six locations that fulfill the objective function are the properties shown in Map 6. We present them in descending order, by the magnitude of the older adult population they would cover. The first (property A), we call it San Agustín, is located to the south-west of the municipality between Avenida el Puerto Street and two lots above Piedra Paloma Street. According to the Municipal Urban Development Plan (Government of the State of Mexico & H. Ayuntamiento de Chimalhuacán, 2019), it is planned to locate a specialized hospital on this property that would include primary care services. This health care unit would serve older adults who suffer from spatial segregation by age and high-risk living areas of slopes and landslides (see section The Demand).
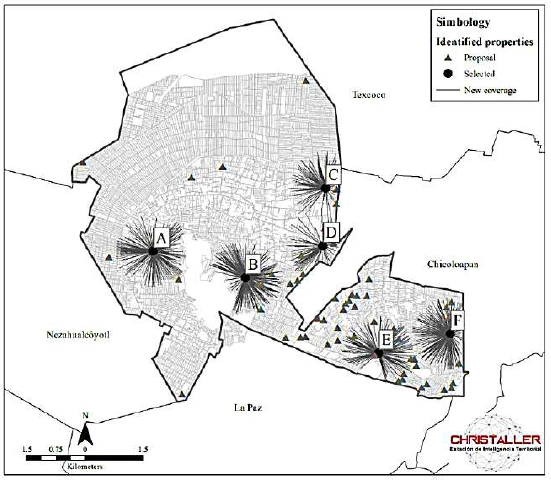
Source: Own elaboration based on Inegi (2020) and Ministry of Health (2021a).
Map 6. Properties identified and selected for possible locations of new health care units in Chimalhuacán, State of Mexico
The third location (property C) is in the Acuitlapilco neighborhood, on Melchor Ocampo Street. It is a location in the process of urban consolidation and the new unit located here would cover older adults concentrated to the north and south of this property (see the Demand section).
The fourth location (property D), on Nezahualcóyotl Avenue, in front of Plaza Chimalhuacán, complements, above all, the coverage to the east of the municipality of the unit located in property
C. There are concentrated multi-family housing complexes and various economic activities and services that make the population move to this location.
The fifth and sixth locations (property E) are proposed in the Ejido Santa María, on Pirul and Camino a la Mina Street and on Claveles Street, next to the Yautlalli tank (property F). This zone is of recent formation and was hardly incorporated into the municipal urban planning.
Locational Solution Discussion
These six new health care units would tend to the population in the Very High Attention Priority situation (Graph 1). In addition, older adults with access to health care units would increase from 35 378 in the current situation to 47 411: an absolute increase of 12 033 people, equivalent to 34% more coverage (Table 1). It’s worth mentioning that the coverage benefits of the units are decreasing: each additional unit increases a smaller number of older adults covered. This is normal if demand remains constant.17
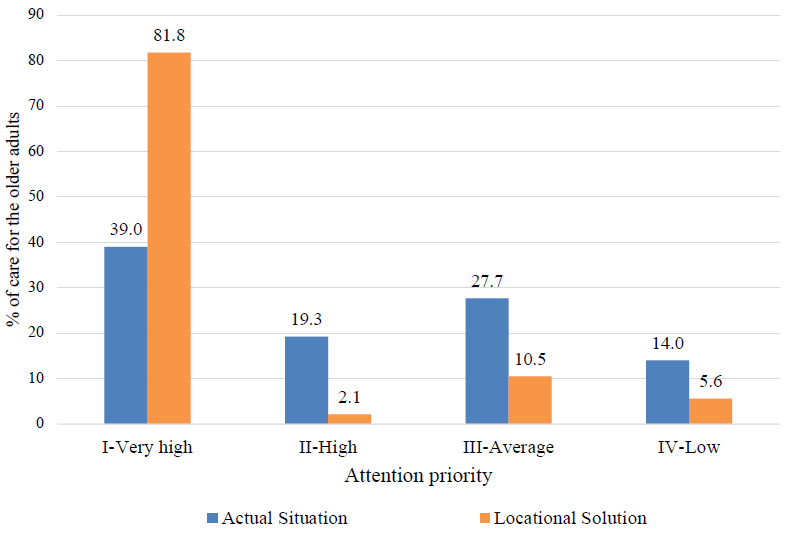
Source: Own elaboration.
Graph 1. Elderly population by attention priority: comparison of Current Situation versus Locational Solution
Table 1. Current situation, planned scenario with six new health care units and key differences: unit by unit as they are added to the health system
| Current situation, new units and planned scenaio |
Older adults with accessibility |
Difference with the current situation |
Total distance traveled by all older adults to access a health unit*(km) |
Average distance traveled per older adult (m) |
Standard deviatio (m) |
Difference with the current situation | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Absolute | Percentage in respect to the current situation |
Total absolute distance traveled (km) |
Porcentage of total distance traveled |
Average per older adult (m) |
Standard deviation (m) |
|||||
| Current situation | 35,378 | N. A. | N. A. | 56,042.8 | 1,584.1 | 615.6 | N. A. | N. A. | N. A. | N. A. |
| New unist accumulated** |
||||||||||
| A | 39,680 | 4,302 | 12.2 | 53,243.0 | 957.7 | 585.0 | -2,799.7 | -39.5 | 626.4 | -30.6 |
| B | 41,983 | 6,605 | 18.7 | 51,684.5 | 937.8 | 573.5 | -4,38.3 | -40.8 | 646.3 | -42.1 |
| C | 44,189 | 8,811 | 24.9 | 50,322.5 | 927.4 | 569.1 | -5,720.3 | -41.5 | 656.7 | -46.5 |
| D | 45,614 | 10,236 | 28.9 | 49,491.7 | 922.2 | 566.4 | -6551.0 | -41.8 | 661.9 | -49.2 |
| E | 46,584 | 11,206 | 31.7 | 48,863.4 | 911.0 | 558.6 | -7,179.4 | -42.5 | 673.1 | -57.0 |
| F | 47,411 | 12,033 | 34.0 | 48,332.3 | 896.5 | 551.7 | -7,710.5 | -43.4 | 687.6 | -63.9 |
| Total planned scenario |
47,41 | 12,033 | 34.0 | 48,332.3 | 896.5 | 551.7 | -7,710.5 | -43.4 | 687.6 | -63.9 |
Source: Own elaboration.
*It is sum of the routes of all adults to access a health care unit.
**The units are added to the healthcare system in Chimalhuacán due to the magnitude of the population they cover.
The six new health care units located in the properties revealed by the P-Median Model would reduce the total cost for older adults to access a health care unit in terms of aggregate distance traveled. In the current situation, the collective cost of accessing a health unit is 56 000 kilometers traveled, the local solution would lower the cost by 7.7 kilometers (43.4%): the benefit would be substantial. The average distance traveled by an older adult to access a supply point would be reduced from 1 584 meters to 896 meters, which means a decrease of 687 meters (Map 7).

Source: Own elaboration based on Inegi (2020), Ministry of Health (2021a) and Christaller (2022a).
Map 7. Current situation and planned scenario with six new health units in Chimalhuacán, State of Mexico
When reviewing the standard deviation of the routes, it is observed that the proposed scenario would not only be more efficient (it would reduce transportation costs and expand coverage of older adults), it would also be more egalitarian: the standard deviation would drop from 615 meters in the current situation at 551 meters in the planned scenario. Plus, it is guaranteeing not to exclude this population from health services; no older adult would be beyond a coverage radius of 15 minutes of comfortable walking (945 meters) to the nearest health unit.
CONCLUSIONS, SCOPE, AND LIMITATIONS
As already mentioned, the COVID-19 pandemic exponentially increased the demand for medical services and put healthcare systems around the world to the test. In Mexico, a large part of those affected are vulnerable urban populations due to age, comorbidities and poor socioeconomic status. In these circumstances, primary health care in the intra-urban space takes on a fundamental role in facing and overcoming current and future health challenges. There’s agreement that this will not be the last global pandemic, the difference lies in how we prepare ourselves to face similar situations in posterity.
Additionally, the pandemic showed that it is necessary to rethink urban needs in all its axes: health, education, employment, transportation, sustainability, to name a few. This implies considering the intra-urban space at its micro-territorial scale (for example, a block), the closest to the population.
Various studies show that accessibility to primary health care impacts health, care costs, and quality of life of the older adults. For this population in poverty, having health care services that are accessible on foot is a way to prevent and mitigate their exposure to pathogens associated with their daily activities and it becomes a key element for improving their well-being. The higher the cost of a good or service, the lower the quality of consumption of health care services and vice versa. Corollary: for urban policy, accessibility to primary health care services is a priority issue of inclusion, human rights, safety and health.
Scope
Let us remember that the objectives of this research were: i. to estimate accessibility to public primary health care units for the older adults in Chimalhuacán through walking transfers and ii. identify the locations that most increase the accessibility of this group to new primary health care units, ensuring that no one has to travel more than a certain distance.
To reach them, two methods focused on achieving a more accessible, efficient and equitable socio-spatial distribution of health resources for older adults were linked. The study area was a metropolitan municipality in general conditions of poverty, with a high population density, which integrates the Metropolitan Zone of the Valley of Mexico (one of the most populated cities in the world).
The first method―two step Floating Catchment Area―allowed estimating the levels of accessibility of the older adult population to the 12 existing health care units through walking transfers. The second―distance restricted P-Median Model―revealed the most convenient locations for six new units, among 68 potential properties, combining criteria of efficiency and equity. The expected benefits of the locational solution would be notable, except in terms of inequality of distance traveled. In the following phases of growth of the healthcare system, the balance between efficiency and equity must be reassessed.
Limitations and Research Agenda
This research has several limitations, all of which can be overcome. On the supply side, health care services were implicitly considered to meet a certain acceptable standard of quality. This is not always true. The quality of healthcare services is heterogeneous, and even if they offer quality, it remains to be seen if they provide warmth, a key aspect for patients without family, a condition present in several older adults in Mexico. There are several methods that measure the quality and warmth of health care services that could be applied in larger scope work.
On the demand side, this article considers average users: those who register a certain comfortable walking speed, for a certain number of minutes, in certain health conditions. The total number of infections is taken, without considering a specific group. This is debatable, even if aggregate planning usually relies on average users. To reduce this limitation, a conservative walking time of 15 minutes was considered here in order to include a higher number of older adults who can travel on foot. It is worth mentioning that the present work is focused on a preventive and primary care scenario, for which one of the limitations is that the care of seriously ill patients who need to move more quickly is not considered. However, in such a case it’s pointed out that a solution may be the use of ambulances, but that would be the subject of another study.
A more important limitation perhaps is that while the supply was considered variable (increased by six health care units), the demand remained constant in terms of magnitude and location. There would be several alternatives to deal with this. The issue of magnitude is not a big problem, Mexico has good projections of population growth at the municipal level. The difficulty lies in projecting the spatial distribution of the demand (older adults) within the municipality. A solution based on models of urban expansion with cellular automata could be tested.
Although the trips around the study area made it possible to appreciate the diversity of topographic features, they were not operationally incorporated into the model. It would be necessary to develop a methodology that affects the speed and comfortable times of walking on slopes or rough terrain (streets without sidewalks, sidewalks in poor condition, the width of roads, etc.) and reflect weather situations such as rainy days, extreme heat or cold, for example. This is a major research topic. Remember that accessibility measures are valuable by their approximate order of magnitude. Complexifying the method to try to make them an exact science could lead to the mirage of precision.
The supplies that are required to run the model and that allow calculating the accessibility index include the data (population and health care units) that is found within the municipality of Chimalhuacán. However, in reality, health care units tend not only to residents of the area, but can also provide medical care to people who have a different municipality as their residence, meaning that although the study area is delimited in the model, there are requests for care that cross the administrative borders inside and outside the municipality.
The methods and models of urban analysis are approximations to reality. These can be applied to simulate and experiment with various scenarios by evaluating certain conditions of accessibility to health care services, modifying the supply (medical units in number and/or size) or the demand (population of older adults growing over a period of time), and, with this variety of scenarios (decision makers and executors of public policies), having information to achieve an optimal distribution of health care services that older adults require to satisfy one of their most immediate needs: health.
REFERENCES
Álvarez Lobato, J. A., Trujillo Herrada, A. y Garrocho Rangel, C. (2018). Urban multifunctionality and the elderly in the Mexico City Metropolitan Area. Investigaciones Geograficas, 96, 1-18. https://doi.org/10.14350/rig.59611 [ Links ]
Álvarez Salazar, G. J., García Gallego, M. y Londoño Usme, M. (2016). Crisis de la salud en Colombia: limitantes del acceso al derecho fundamental a la salud de los adultos mayores. Revsista CES Derecho, 7(2), 106-125. https://doi.org/10.21615/CESDER.7.2.8 [ Links ]
Bosch Meda, J. (2013). Ciudad y envejecimiento: bases para un nuevo urbanismo: V Premio Nacional de Urbanismo Ricardo Santos Diez. Práctica urbansitica. Revista Mensual de Urbanismo, 120, 36-51. Recuperado de https://dialnet.unirioja.es/servlet/articulo?codigo=4116091 [ Links ]
Brizan St Martin, R. y Juel, P. (2022). Evaluating the performance of GIS methodologies for quantifying spatial accessibility to healthcare in Multi-Island Micro States (MIMS). Health Policy and Planning. https://doi.org/10.1093/heapol/czac001 [ Links ]
Buzai, G. y Baxendale, C. (2008). Modelos de localización-asignación aplicados a servicios públicos urbanos: Análisis espacial de escuelas EGB en la ciudad de Luján. Revista Universitaria de Geografía, 17, 233-254. Recuperado de http://www.redalyc.org/articulo.oa?id=383239098009 [ Links ]
Chávez Soto, T. y Garrocho Rangel, C. (2018). Christaller®: Estación de Inteligencia Territorial. Revista Geografía y Sistemas de Información Geográfica (GeoSig), 10, 29-50. Recuperado de http://www.revistageosig.wixsite.com./geosig [ Links ]
Chen, X. y Jia, P. (2019). A comparative analysis of accessibility measures by the two-step floating catchment area (2SFCA) method. International Journal of Geographical Information Science, 33(9), 1739-1758. https://doi.org/10.1080/13658816.2019.1591415 [ Links ]
Christaller. (2022a). Modelos de interacción espacial (1.0) [Software]. Recuperado de http://www.christaller.org.mx/index.php/gallery/tools/102-art-mie-descripcion-general [ Links ]
Christaller. (2022b). Análisis de casos positivos a la prueba COVID-19 [Conjunto de datos interactivos]. Recuperado de http://www.christaller.org.mx/#:~:text=CHRISTALLER%20es%20un%20conjunto%20de,de%20servicios%20p%C3%BAblicos%20y%20privados [ Links ]
Consejo Nacional de Evaluación de la Política de Desarrollo Social (Coneval). (2015). Rezago social a nivel zonas urbanas (AGEB urbanas). Presentación de resultados. Consejo Nacional de Evaluación de la Política de Desarrollo Social. Recuperado de https://www.coneval.org.mx/Medicion/IRS/Paginas/Indice_Rezago_Social_2015.aspx [ Links ]
Consejo Nacional de Evaluación de la Política de Desarrollo Social (Coneval). (2018). Medición de la pobreza. Consejo Nacional de Evaluación de la Política de Desarrollo Social. Recuperado de https://www.coneval.org.mx/Medicion/Paginas/Glosario.aspx [ Links ]
De Alba González, M. (2017). Representaciones sociales y experiencias de vida cotidiana de los ancianos en la Ciudad de México. Estudios Demográficos y Urbanos, 32(1), 9-36. https://doi.org/10.24201/EDU.V32I1.1616 [ Links ]
Descant, S. (2021). Equitable Urban Planning May Mean Ditching the 15-Minute City. Future Structure. Recuperado de https://www.govtech.com/fs/equitable-urban-planning-may-mean-ditching-the-15-minute-city.html [ Links ]
Diario Oficial de la Federación (DOF). (30 de noviembre de 2012). Norma Oficial Mexicana. NOM-035-SSA3-2012, en materia de información en salud. Diario Oficial de la Federación. Recuperado de https://dof.gob.mx/nota_detalle.php?codigo=5280848&fecha=30/11/2012-gsc.tab=0 [ Links ]
Enríquez Reyna, M. C., Cruz Quevedo, J. E., Celestino Soto, M. I., Garza Elizondo, M. E. y Salazar González, B. C. (2013). Función ejecutiva, velocidad de marcha y tarea doble en adultos mayores mexicanos. Revista Iberoamericana de Psicología del Ejercicio y el Deporte, 8(2), 345-357. Recuperado de https://www.redalyc.org/articulo.oa?id=311128824006 [ Links ]
Gaceta del Senado. (2016). Gaceta del Senado. Recuperado de https://www.senado.gob.mx/64/gaceta_del_senado/documento/66725 [ Links ]
Galindo Pérez, C. y Suárez Lastra, M. (2018). Servicios de salud del ISSSTE en la Zona Metropolitana de la Ciudad de México. ¿Qué pasaría si nos enfermáramos todos? Gestión y Política Pública, 27 (2), 475-499. Recuperado de http://www.scielo.org.mx/scielo.php?script=sci_abstract&pid=S1405-10792018000200475&lng=es&nrm=iso&tlng=es [ Links ]
Garrocho Rangel, C. y Campos Alanís, J. (2006). Un indicador de accesibilidad a unidades de servicios clave para ciudades mexicanas: fundamentos, diseño y aplicación. Economía Sociedad y Territorio, VI(22), 349-397. https://doi.org/10.22136/EST002006262 [ Links ]
Garrocho Rangel, C. y Campos Alanís, J. (2016). Segregación socioespacial de la población mayor. La dimensión desconocida del envejecimiento. Ciudad de México: El Colegio Mexiquense. [ Links ]
Garrocho Rangel, C. y Ramos Pérez, D. (2019). La importancia de la accesibilidad de la población mayor vulnerable a servicios de salud [Documento de trabajo]. [ Links ]
Garrocho Rangel, C. y Vilchis Mata, I. (2021). Las Age-Friendly cities facilitan la movilidad de los adultos mayores. Korpus 21, 1(2), 295-316. https://doi.org/https://doi.org/10.22136/korpus21202135 [ Links ]
Garrocho Rangel, C., Chávez Soto, T. y Álvarez Lobato, J. A. (2020). Accesibilidad de la población mayor a farmacias en el espacio intraurbano: desplazamientos caminando y el método de área de cobertura flotante. En O. Figueroa y L. M. Valenzuela (Eds.), Desafíos del desarrollo urbano sostenible en el transporte y la movilidad (pp. 415-442). Ciudad de México: El Colegio Mexiquense. [ Links ]
Giovanella, L., Vega, R., Tejerina Silva, H., Acosta-Ramirez, N., Parada Lezcano, M., Ríos, G., Iturrieta, D., Fidelis de Almeida, P. y Feo, O. (2021). ¿Es la atención primaria de salud integral parte de la respuesta a la pandemia de Covid-19 en Latinoamérica? Trabalho, Educação e Saúde, 19, 1-28. https://doi.org/https://doi.org/10.1590/1981-7746-sol00310 [ Links ]
Gobierno del Estado de México y H. Ayuntamiento de Chimalhuacán. (2019). Plan Municipal de Desarrollo Urbano de Chimalhuacán. Planes Municipales de Desarrollo Urbano. Recuperado de http://seduv.edomexico.gob.mx/planes_municipales/chimalhuacan/E-2.pdf [ Links ]
González González, C. A., Orozco Rocha, K., Samper Ternent, R. y Wong Luna, R. (2021). Adultos mayores en riesgo de Covid-19 y sus vulnerabilidades socioeconómicas y familiares: un análisis con el ENASEM. Papeles de Población, 27(107), 141-165. https://doi.org/10.22185/24487147.2021.107.06 [ Links ]
Guida, C. y Carpentieri, G. (2021). Quality of life in the urban environment and primary health services for the elderly during the Covid-19 pandemic: An application to the city of Milan (Italy). Cities, 110, 1-15. https://doi.org/10.1016/J.CITIES.2020.103038 [ Links ]
Gutiérrez Robledo, L. M. y Kershenobich Stalnikowitz, D. (2015). Envejecimiento y salud: una propuesta para un plan de acción. México: UNAM, Academia Nacional de Medicina de México, Academia Mexicana de Cirugía, Instituto Nacional de Geriatría. Recuperado de http://www.geriatria.salud.gob.mx/descargas/publicaciones/Envejecimiento_y_salud_3a_edicion.pdf [ Links ]
Harvey, D. (2010). Social justice and the city. Georgia: University of Georgia Press. [ Links ]
Hooper, P., Foster, S., Nathan, R. y Giles Corti, B. (2012). Built environmental supports for walking. En B. Ainsworth y C. A. Macera (Eds.), Physical activity and public health practice (pp. 257-276). CRC Press. [ Links ]
Huenchuan, S. (2020). COVID-19: Recomendaciones generales para la atención a personas mayores desde una perspectiva de derechos humanos (Documento de trabajo LC/MEX/TS.2020/6/Rev.1). Comisión Económica para América Latina y el Caribe (CEPAL). Recuperado de https://repositorio.cepal.org/bitstream/handle/11362/45316/4/S2000271_es.pdf [ Links ]
Instituto Nacional de Estadística y Geografía (Inegi). (2018). Encuesta Nacional de la dinámica demográfica ENADID 2018. Presentación de resultados [Gráficos]. Instituto Nacional de Estadística, Geografía e Informática. Recuperado de https://www.inegi.org.mx/programas/enadid/2018/ [ Links ]
Instituto Nacional de Estadística y Geografía (Inegi). (2020). Censo de Población y Vivienda 2020. Microdatos [Conjunto de datos]. Instituto Nacional de Estadística, Geografía e Informática. Recuperado de https://www.inegi.org.mx/programas/ccpv/2020/default.html#Microdatos [ Links ]
Karlan, D. y Morduch, J. (2019). Microeconomics. McGraw-Hill. [ Links ]
Lenardt, M. H., Setlik, C. M., Pereira, A. P., Lourenço, T. M., Barbiero, M. M. A., Betiolli, S. E. y Rodríguez Martínez, M. del C. (2021). Velocidad de la marcha y cognición en adultos mayores en atención secundaria de salud. Avances en Enfermería, 39(1), 84-92. https://doi.org/10.15446/AV.ENFERM.V39N1.88364 [ Links ]
Luo, W. y Wang, F. (2003). Measures of Spatial Accessibility to Healthcare in a GIS Environment: Synthesis and a Case Study in Chicago Region. Environment and planning. B, Planning & design, 30(6), 865-884. https://doi.org/10.1068/b29120 [ Links ]
Luo, W. y Whippo, T. (2012). Variable catchment sizes for the two-step floating catchment area (2SFCA) method. Health & Place, 18(4), 789-795. https://doi.org/10.1016/J.HEALTHPLACE.2012.04.002 [ Links ]
Mattioli, L. y Schneider, M. (2020). Redefiniendo nuestro futuro: La transformación de nuestras ciudades frente a la crisis COVID-19. En G. C. Delgado Ramos y D. Lopez Garcia (Eds.), Las ciudades ante el COVID-19: nuevas direcciones para la investigación urbana y las políticas públicas (pp. 340-345). International Network for Government Science Advice. https://doi.org/10.5281/ZENODO.3894075 [ Links ]
Mollenkopf, H., Hieber, A. y Wahl, H. W. (2011). Continuity and change in older adults perceptions of out-of-home mobility over ten years: a qualitative-quantitative approach. Ageing & Society, 31(5), 782-802. https://doi.org/10.1017/S0144686X10000644 [ Links ]
Montes de Oca, V. (2010). Pensar la vejez y el envejecimiento en el México contemporáneo. Revista Renglones, 62, 159-181. Recuperado de https://rei.iteso.mx/handle/11117/235?show=full [ Links ]
Nyadera, I. N., Onditi, F., Obimbo, M. M. y Muchina, S. K. (2021). Policy and research frame of the coronavirus disease 2019 (COVID-19) pandemic: reflections on urban informality. Global Health Journal, 5(1), 12-17. https://doi.org/10.1016/J.GLOHJ.2021.02.007 [ Links ]
Organización para la Cooperación y el Desarrollo Económico (OCDE) y The World Bank (WB). (2020). Panorama de la Salud: Latinoamérica y el Caribe 2020. En Panorama de la Salud: Latinoamérica y el Caribe 2020. OCDE/WB. https://doi.org/10.1787/740f9640-es [ Links ]
O’Sullivan, A. (2019). Urban Economics. McGraw Hill. [ Links ]
Pérez Valbuena, G. J. (2015). Accesibilidad geográfica a los servicios de salud: un estudio de caso para Barranquilla. Sociedad y Economía, 28, 181-208. https://doi.org/10.25100/sye.v0i28.3935 [ Links ]
Rasanathan, K. y Evans, T. G. (2020). Primary health care, the declaration of astana and COVID-19. Bulletin of the World Health Organization, 98(11), 801-808. https://doi.org/10.2471/BLT.20.252932 [ Links ]
Rojas Moreno, K. T. y Aguilar Martínez, A. G. (2021). Probabilidad de atención médica para los pobres en la Zona Metropolitana de Cuernavaca, Morelos, en 2018. Economía Sociedad y Territorio, 21(67), 835-864. https://doi.org/10.22136/EST20211761 [ Links ]
Rybertt, C., Cuevas, S., Winkler, X., Lavados, P. y Martínez, S. F. (2015). Parámetros funcionales y su relación con la velocidad de marcha en adultos mayores chilenos residentes en la comunidad. Biomédica, 35(2), 212-218. https://doi.org/10.7705/BIOMEDICA.V35I2.2571 [ Links ]
Sansão Fontes, A. y Espósito Galarce, F. (2021). Urbanismo de proximidad en Barcelona. Una ciudad saludable a 15 minutos del hogar. Planeo, 93, 1-13. Recuperado de http://revistaplaneo.cl/2021/01/20/urbanismo-de-proximidad-en-barcelona-una-ciudad-saludable-a-15-minutos-del-hogar/ [ Links ]
Secretaría de Salud (2021b). Datos abiertos. Dirección General de Epidemiología. Recuperado de https://www.gob.mx/salud/documentos/datos-abiertos-152127 [ Links ]
Secretaría de Salud (2021a). Recursos en Salud. Datos Abiertos [Conjunto de datos]. Catálogo CLUES. Recuperado de http://www.dgis.salud.gob.mx/contenidos/intercambio/clues_gobmx.html [ Links ]
Sgaravatti, A., Santos, D., Bermúdez, G. y Barboza, A. (2018). Velocidad de marcha del adulto mayor funcionalmente saludable. Anales de la Facultad de Medicina, 5(2), 93-101. https://doi.org/10.25184/ANFAMED2018V5N2A8 [ Links ]
Simmons, J., Garrocho Rangel, C., Kamikihara, S. y Campos Alanís, J. (2018). The evolving retail structure of Mexico City. Papers in Applied Geography, 4(3), 305-325. https://doi.org/10.1080/23754931.2018.1486731 [ Links ]
Smith, M. (2020). The fifteen minute vision: Future proofing our cities. ARUP. Recuperado de https://www.arup.com/perspectives/the-fifteen-minute-vision-future-proofing-our-cities [ Links ]
Tao, Z., Cheng, Y. y Liu, J. (2020). Hierarchical two-step floating catchment area (2SFCA) method: Measuring the spatial accessibility to hierarchical healthcare facilities in Shenzhen, China. International Journal for Equity in Health, 19(164), 1-16. https://doi.org/10.1186/S12939-020-01280-7/FIGURES/8 [ Links ]
Varela Pinedo, L., Ortiz Saavedra, P. J. y Chávez Jimeno, H. (2010). Velocidad de la marcha como indicador de fragilidad en adultos mayores de la comunidad en Lima, Perú. Revista Española de Geriatría y Gerontología, 45(1), 22-25. https://doi.org/10.1016/J.REGG.2009.07.011 [ Links ]
Vega Rivero, J. A., Ruvalcaba Ledezma, J. C., Hernández Pacheco, I., Acuña Gurrola, M. D. R. y López Pontigo, L. (2020). La salud de las personas adultas mayores durante la Pandemia de COVID-19. Journal of Negative and No Positive Results, 5(7), 726-739. https://doi.org/10.19230/JONNPR.3772 [ Links ]
Von Seidlein, L., Alabaster, G., Deen, J. y Knudsen, J. (2021). Crowding has consequences: Prevention and management of COVID-19 in informal urban settlements. Building and Environment, 188(107472), 1-9. https://doi.org/10.1016/j.buildenv.2020.107472 [ Links ]
Welti-Chan, C. Ramírez Penagos, A. C. (2021). Conocimiento sociodemográfico y respuesta institucional a una pandemia. El caso de méxico. Papeles de Poblacion, 27(107), 103-163. https://doi.org/10.22185/24487147.2021.107.04 [ Links ]
6Public establishment, social or private, whichever its denomination, whose purpose is to care for patients, whether or not they are hospitalized for consultation, diagnosis, treatment and/or rehabilitation (DOF, 2012).
8A person is in a situation of poverty when they have at least one social deprivation (in the six indicators of educational lag, access to health care services, access to public safety, housing quality and spaces, basic housing services and access to food) and their income is insufficient to acquire the goods and services they require to meet their food and non-food needs (Coneval, 2018).
10For example, transportation. Although the transfer is done on foot, it involves certain important costs: time, effort, risk.
11Location, because it locates the health care units in the territory; allocation, because it allocates the demand to each health care unit.
12An AGEB is defined as a set of blocks bounded by streets, avenues, walkways or any other feature of easy identification in the field and whose land use is primarily residential, industrial, services, commercial, etc. They can be classified into two types: urban and rural. The urban AGEBs are assigned to geographic areas of localities with a population equal to or greater than 2,500 inhabitants or to municipal seats.
13The social backwardness index is a weighted measure that includes four indicators of social deprivation: education, access to health care services, basic housing services, and housing quality and spaces.
15The healthcare deserts include neighborhoods such as Ladera, Barrio de Xochiaca, El Olivar and those located in the Ejido Santa María. In addition to the low accessibility, the topographic factor of the area must be included, which requires traveling steep slopes.
16Vacant lots with land suitable for placing public infrastructure with minimum dimensions to house a health care unit with at least one office.
17Dynamizing the spatial and demographic expansion of the demand would be the subject of another study (see, for example, Garrocho et al., 2021).
Received: March 25, 2022; Accepted: May 31, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative
Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative
Commons
