










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkPerinatología y reproducción humana
On-line version ISSN 2524-1710Print version ISSN 0187-5337
Perinatol. Reprod. Hum. vol.27 n.3 Ciudad de México Jan. 2013
Original article
Ending Preventable Child and Maternal Deaths in Latin American and Caribbean Countries (LAC)
Fin a las muertes evitables maternas e infantiles en los países de Latinoamérica y del Caribe (LAC)
Ariel Pablos-Mendez,* Veronica Valdivieso,‡ Kelly Flynn-Saldaña§
* Assistant Administrator, Global Health Bureau, USAID.
‡ Deputy Health Team Leader, Regional Sustainable Development Office, Latin America and Caribbean Bureau, USAID.
§ Deputy Director, Office of Health, Infectious Disease and Nutrition, Global Health Bureau, USAID
Correspondence:
Ariel Pablos-Mendez, MD, MPH
Attn: Lindsey Kirn, MPH
U.S. Agency for International Development
Global Health Bureau/Office of the Assistant Administrator
1300 Pennsylvania Avenue, NW.
Washington, DC 20523
Ph: 202.712.5841.
E-mail: LKIRN@usaid.gov
Received: 15 de agosto de 2013
Accepted: 20 de agosto de 2013
ABSTRACT
Many countries in Latin America and the Caribbean (LAC) have reached or exceeded their Millennium Development Goal, despite this progress, significant work remains in order to end the millions of preventable child and maternal deaths that occur annually. This will require increasing coverage of high-impact interventions, strengthening the health systems that support these interventions, and addressing major equity gaps within and among countries. On June 14-15, 2012, in Washington, D.C., the Governments of Ethiopia, India and the United States, together with UNICEF, convened a global "Child Survival Call to Action" (CSCTA) to achieve an ambitious yet achievable goal: to end preventable child deaths. A central premise of the Call to Action is that we already know how to prevent most child deaths and can do so by scaling up existing, practical, affordable interventions. The CSCTA and the follow on activities under A Promise Renewed , led by UNICEF, emphasize the importance of developing country-led planning and marshaling of countries' own resources to improve child health. Under this vision, donor support is to be supplementary -not the primary force shaping developing countries' work to reduce child mortality. As a result of the meeting, 175 countries around the world have signed a pledge committing to address child survival, including 31 countries in the Latin American and Caribbean Region.
Key words: Maternal mortality, infant mortality, UNICEF, developing countries.
RESUMEN
La mayoría de países de Latinoamérica y del Caribe (LAC) han alcanzado las metas del milenio; no obstante estos progresos, aún es necesario efectuar un esfuerzo intenso para frenar los millares de muertes maternas e infantiles que ocurren anualmente y que son prevenibles. Este esfuerzo requiere de una serie de intervenciones de alto impacto, el fortalecimiento de los sistemas de salud nacionales y la disminución de las brechas de equidad entre los diferentes países de la región de LAC. En junio de 2012, los gobiernos de Etiopía, India y los Estados Unidos, en conjunto con la UNICEF, convinieron en efectuar un "llamado a la acción por la supervivencia de los niños" (CSCTA), proponiendo la meta de frenar las muertes infantiles prevenibles. La premisa central de este llamado es que ya se debe de saber cómo prevenir estas muertes, y poder llevar a cabo las intervenciones de manera asequible y práctica. El CSCTA, conforme las acciones subsecuentes a llevar a cabo, siguiendo a la UNICEF, enfatiza en la importancia de que cada país planifique y calcule los recursos propios que deberá invertir para reducir las muertes infantiles. Bajo esta visión, los soportes económicos de apoyo de organismos internacionales sólo deberán ser suplementarios, no el recurso principal de los países en desarrollo, para reducir la mortalidad infantil. Como resultado de la reunión de junio de 2012, 175 países alrededor del mundo han firmado los compromisos del CSCTA, incluyendo 31 países de la región de LAC.
Palabras clave: Mortalidad maternal, mortalidad infantil, UNICEF, países en desarrollo.
The world has witnessed an extraordinary 70 percent decline in child mortality over the last 50 years1 and a reduction in the burden of under-five deaths from nearly 12 million in 1990 to fewer than 7 million in 2011.2 There has also been a nearly 50 percent reduction in maternal deaths as the global maternal mortality ratio declined from 400 deaths per 100,000 live births to 210 at an average annual rate of reduction of 3.1 percent between 1990 and 2010.3 Despite this progress, significant work remains in order to end the millions of preventable child and maternal deaths that occur annually. This will require increasing coverage of high-impact interventions, strengthening the health systems that support these interventions, and addressing major equity gaps within and among countries. Ending preventable child and maternal deaths in the world is nonetheless achievable in our lifetime.
On June 14-15, 2012, in Washington, D.C., the Governments of Ethiopia, India and the United States, together with UNICEF, convened a global "Child Survival Call to Action" (CSCTA) to achieve an ambitious yet achievable goal: to end preventable child deaths. The Call to Action launched a world-wide movement called Committing to Child Survival: A Promise Renewed to save children's lives and bolster political commitment by governments to improve child and maternal health, under a common agreement and belief that every child should be given the opportunity to survive and thrive. Recognizing that every year, 6.9 million children die before their 5th birthday, more than 170 countries have committed to bring child mortality down from the current global level of 51 per 1,000 live births to 20 per 1,000.4 A central premise of the Call to Action is that we already know how to prevent most child deaths and can do so by scaling up existing, practical, affordable interventions. By doing this and focusing on the main killers of children under 5 -neonatal complications, pneumonia, diarrhea, malaria and malnutrition- we can reach our goal of reducing child mortality to 20 per 1,000 by 2035.5
The CSCTA and the follow on activities under A Promise Renewed , led by UNICEF, emphasize the importance of developing country-led planning and marshaling of countries' own resources to improve child health.6 Under this vision, donor support is to be supplementary -not the primary force shaping developing countries' work to reduce child mortality. As a result of the meeting, 175 countries around the world have signed a pledge committing to address child survival, including 31 countries in the Latin American and Caribbean Region.7
Many countries in Latin America and the Caribbean have reached or exceeded their Millennium Development Goal (MDG) 5, improving maternal health, and many have or will soon achieve the new global goal of ending preventable child deaths (defined as an under-5 mortality rate (U5MR) of 20 deaths per 1,000 live births). Currently, only Haiti (70), Bolivia (51) and Guyana (36) have an U5MR of greater than 30 and the remaining seven countries that have not achieved this goal remain close, with an U5MR between 20 and 30 per 1,000 live births.8 This success means that there are lessons to be learned from the region for the rest of the world.
However, nationally averaged numbers also mask great inequities within many of the region's countries, so its progress also tells a cautionary tale for other countries: adhering to the principle of equity endorsed at the Call to Action and re-enforced by USAID, UNICEF and other global partners committed to this cause will require looking beyond national child survival rates to variations among population sub-groups. In Latin America and the Caribbean, over 180,000 children under 5 years old9 and nearly 9,000 mothers10 still die annually, most of them among poor, indigenous, and marginalized groups (Table I).
USAID, in partnership with the Pan-American Health Organization, the Inter-American Development Bank, Salud Mesoamérica 2015, UNAIDS, UNFPA, UNICEF, and the World Bank, is sponsoring a meeting entitled " A Promise Renewed for the Americas : Reducing Inequities in Reproductive, Maternal and Child Health" in September in Panama City, Panama. This meeting is a regional follow-up to the June 2012 event in Washington, and it will be tailored to the current challenges throughout the region. It will call on the region's countries to commit to the goal of ending preventable child and maternal deaths, as well as promoting maternal and child health, across all socio-economic strata.
Advancing the goals of A Promise Renewed requires countries and the global community to undertake five strategic shifts. By applying these key ideas to the challenge of promoting equity in child and maternal health and survival, the countries of Latin America and the Caribbean will continue their global leadership in this area and accelerate the full realization of these goals for vulnerable sub-groups in the region.
Focus geographically
High-burden countries must assume leadership of child survival efforts and draw on the expertise and support of a range of actors including the private sector, civil society organizations, and faith-based organizations. These efforts can include setting goals and targets for child survival, targeting financing to child health, and developing explicit business plans for achieving success. In order to monitor progress and target resources, countries must improve national and sub-national data collection. Better data collection will help determine local priorities and adapt health interventions to local conditions and demands.
Increase efforts with high-burden populations
The child mortality burden can vary considerably within countries and can be high in pockets even when, on average, a nation is doing well. Countries should increasingly target their efforts to the highest burden areas at sub-national levels, e.g., rural and low-income populations, and other marginalized groups. Equity-based approaches should expand services and reduce disparities in access to essential services and in out-of-pocket expenditures.
LAC is the most inequitable region in the world. Although the region has achieved a great level of growth, average statistics of socioeconomic indicators for each country frequently hide significant variations between urban and rural territories.13
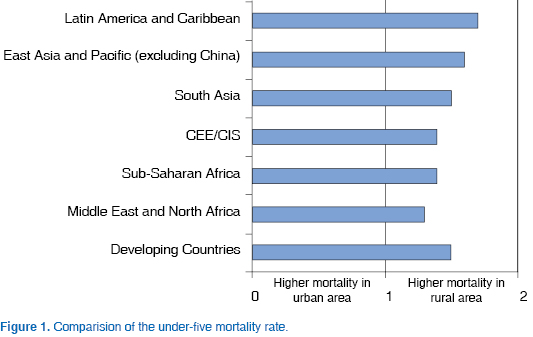
Under-five mortality is higher in rural than in urban areas across the world, but the largest gap is in Latin America. The figure 1 compares the under-five mortality rate between the poorest 20 percent and the richest 20 percent over time.14 The results show that overall, in developing countries, under-five mortality is 50 percent higher in rural areas, for Latin America under-five mortality is 70 percent higher in rural areas.
Similar gaps are observed in urban versus rural Infant Mortality Rates in LAC11 (Table II):
Significant poverty is also associated with undernutrition. According to estimates based on household income, 13 percent of LAC's population live in households with incomes insufficient to satisfy their basic nutritional needs. Given that the 2013 Lancet series on nutrition found that "undernutrition is responsible for 45 percent of deaths of children younger than 5 years", addressing these inequities with regard to basic needs is critical to reducing child mortality in the region.15 According to the Lancet, "the effect on maternal and child health outcomes and health-care provision is striking, regardless of the indicator used to measure inequity. For example, maternal mortality ratios are 10-44 times higher in the poorest provinces of several countries in Latin America. The poorest quintile of the population showed 3-10 times the prevalence of stunted children than the richest quintile in nine countries" (Figure 2).16

Apply cost-effective solutions to the most important causes of maternal mortality and under-five deaths
Countries should systematically identify as priorities the most important causes of under-five deaths and the cost-effective, evidence-based interventions and delivery strategies that have the largest potential for sustained impact. Scaling-up known, effective solutions will get countries most of the way to achieving their targets. Significant reductions in neonatal deaths require interventions that directly address the neonatal period as well as maternal health interventions that protect both the mother and child: expansion of facility-based care, better use of skilled frontline healthcare workers and regular access to life-saving commodities. Access to and effective use of commodities where and when they are needed is also a critical component of cost-effective interventions.
Maternal health, particularly among mothers between 10 and 15 years of age, has a direct impact on child health. The region has an average estimated maternal mortality ratio (MMR) of 81 per 100,000 live births.17 Fifteen of LAC's countries have estimated MMR figures above the regional average (Bolivia, Colombia, Dominican Republic, Ecuador, El Salvador, Guatemala, Guyana, Haiti, Honduras, Jamaica, Nicaragua, Panama, Paraguay, Suriname, and Venezuela). The majority of maternal deaths in the region occur during childbirth and in the first hours postpartum. Approximately 95 percent of maternal mortality in LAC can be prevented by using knowledge currently available in the countries. The most frequent causes of death are pregnancy induced hypertension (26 percent), hemorrhage (21 percent), complications of abortion in unsafe conditions (13 percent), obstructed labor (12 percent), sepsis (8 percent), and other direct causes (4 percent).18
In 2011, close to half of LAC's under-5 mortality occurred in the neonatal age group.19 The majority of neonatal are caused by preterm birth complications and congenital abnormalities, while major causes of death in the post-neonatal group include pneumonia and diarrheal diseases.20 The majority of these deaths are preventable. Selected high-impact, low-cost interventions could further reduce the number of deaths, but levels of coverage need to be adequate among populations with higher mortality.
Despite two decades of development gains and the recent economic growth in LAC countries, large health disparities remain among and within countries with regard to access and quality of reproductive health services. Investments in voluntary family planning dramatically improve maternal and child health, and more broadly can contribute to economic and social development and stability.
Family planning plays a critical role in ending preventable child and maternal deaths. As more women gain voluntary access to family planning, and as more unintended pregnancies are prevented, more children will survive and be healthy. Use of family planning for spacing and limiting the number of children according couples' desires helps women bear children at the healthiest times in their lives. Family planning has powerful life-saving impacts for mothers and infants. Findings of key studies on family planning's overall contribution to child and maternal survival globally include:
• Access to voluntary family planning could reduce maternal deaths by 25-40 percent and child deaths by as much as 20 percent.21
• If all birth-to-pregnancy intervals were increased to 3 years, 1.6 million under-five deaths could be prevented annually.
• In one year, family planning prevented more than 272,000 maternal deaths, a 44 percent reduction.22
• If all needs for family planning were met, an additional 104,000 maternal deaths could be prevented annually.
Family planning is a good investment, since every dollar invested in family planning may save up to (US)$31 in spending on health, education, housing, water and other public services.23 Research in LAC region also shows a strong return on investment; for example, Guatemala's Ministry of Health saves an estimated $14 Guatemalan Quetzales on maternal, child, and neonatal health care for each $1 Quetzal invested in family planning. Family planning interventions make vital contributions to preventing child and maternal deaths and helping women survive and prosper.
Fertility and contraceptive prevalence indicators have been slow to improve among poor, rural, or otherwise marginalized groups. In LAC, more than one-half of pregnancies are unintended, even though about 65 percent of married women of reproductive age use modern contraceptives.24 Although rates for the region overall are positive, large pockets of unmet need exist for family planning and reproductive health services, and ensuring uninterrupted contraceptive supplies and access to quality services for the neediest remains a challenge.
Address the broader context: education, empowerment, economy and environment
In addition to the focus on the health sector and medical interventions, greater coordination is needed with policies and programs that impact child survival more broadly and address the underlying causes of child mortality. These policies and programs include education, infrastructure development, water supply, sanitation, and income generation.
Progress toward reaching the MDGs has been inconsistent within and across countries, with frequent neglect of the poorest groups (often girls and indigenous populations) and those lacking access to education (often populations living in remote areas). Early childhood development programs have low coverage, and many child survival strategies still use a vertical approach that fails to consider the environmental situation and other social determinants of health. These constraints are major obstacles to meeting the needs of children, improving their living conditions, protecting their fundamental rights, and to achieving greater equality among different social sectors.
It is noteworthy that basic education and literacy remain major challenges in many LAC countries despite generally high levels of school enrollment. The education of girls in particular is closely correlated with improved child health and survival, bolstering the already strong case for improving primary and secondary education systems in the LAC region.
Ensure mutual accountability for ending preventable child deaths
Governments will lead the effort by sharpening their national action plans with costed strategies for maternal and child survival, and by setting and monitoring five-year milestones. Development partners can support the national targets by pledging to align their support with government-led action plans and priorities; private sector partners can spur innovation and help identify new resources for child survival; and, through action and advocacy, civil society and faith leaders can support the communities and families whose decisions profoundly influence prospects for maternal and child survival.
The " A Promise Renewed for the Americas : Reducing Inequities in Reproductive, Maternal and Child Health" event in Panama will provide countries the opportunity to formulate their own responses to the recommended strategic shifts described here. At the same time, the region should also take the opportunity to celebrate the tremendous successes already achieved by many countries and identify the lessons learned from those successes. Below are but a few examples that provide insight into the factors leading to the success seen to date in this region:
• Integrated Management of Childhood Illness (IMCI) : The LAC region was one of the first to adopt the IMCI strategy. It built on existing efforts to integrate child survival programing that the countries had already begun. Similarly, many of the LAC countries were the first to include integrated child survival programs at the community level. These strategies represent early successful efforts to apply cost-effective solutions to the major causes of under-five mortality.
• Conditional Cash Transfers (CCTs) : Starting in the late 1990s, Brazil and Mexico began experimenting with conditional cash transfer programs, which aimed to reduce poverty and improve health and other outcomes through provision of incentive payments for certain behaviors. The innovative approach spread throughout the region, so that by 2011 eighteen countries had a CCT program, with a total of 129 million beneficiaries. (27) Rigorous program evaluations have found CCTs to increase demand for health services and reduce poverty, although they should to be carefully targeted to the poor to reduce inequities and often require improvements in the quality of care to maximize health impact. (25) Conditional Cash Transfers are a successful example of the benefits that can be gained through consideration of the broader context to child mortality.
• Supply Chain Strengthening: Under USAID's leadership many of the countries of the region have been working together to strengthen supply chains. Periodic meetings enable the sharing of experiences and progress. Although the efforts started with a focus on contraceptive security in the face of graduation from USAID assistance - these commodity security committees often now support integrated supply chains that deliver a full range of medications and supplies for health care systems. Increased collaboration between USAID and the Inter-American Bank's Salud Mesoamerica 2015 initiative has ramped up efforts to strengthen supply chains in Central America in particular.
• Universal Health Coverage: In the past twenty years, a number of LAC countries have made strides toward greater access to health coverage for their populations. Significant health reforms have included the Unified Health System in Brazil, which includes a strong emphasis on primary care for all Brazilians; nearly universal coverage for Chileans through the Social Health Insurance program; a constitutional right to healthcare and subsidized national insurance system in Colombia; and coverage for 50 million Mexicans under the Popular Health Insurance program.26
Challenges remain in terms of quality of care and access for impoverished rural populations in many countries. However these examples exemplify a mindset to target resources toward underserved populations.
Conclusion
As Latin America and the Caribbean continue to develop, the role of international donor agencies will continue to evolve. Gains in the health status of the region have paralleled significant gains in economic development since 1990. The region has been growing even in during the recent global economic slowdown, with a 3.5 percent average GDP growth rate expected this year by the World Bank.27 Due to years of growth in the region, over the past ten years, the World Bank estimates that more than 70 million people have risen out of poverty and approximately 50 million have joined the middle class.28 In recent years, donors have reduced overall investment in the region, reduced grants for program implementation, and have shifted towards provision of technical assistance to support government priorities in most of the countries in the region. By fiscal year 2014, USAID will have just two remaining bilateral health programs: Haiti and Guatemala. However, USAID will continue to provide technical assistance through regional programs aimed at building country capacity on key issues in health systems, tuberculosis control, family planning, and maternal and child health. In the meantime, several countries, including Brazil and Mexico, have been reaching out with their own know-how and funding and have begun to forge their own approach to development assistance. As noted above there is great potential for continued region-wide collaboration and exchange to take the next steps toward full realization of "A Promise Renewed." The meeting in Panama, like the global Call to Action last June, is but a step in this important effort to further reduce unnecessary child and maternal death in the region and promote the right of each child to develop, thrive, and celebrate his/her 5th birthday. With the commitment of each country in the region we can end preventable child and maternal deaths.
REFERENCIAS
1. Child Survival Call to Action: Ending Preventable Child Deaths. June 2012, available at http://5thbday.usaid.gov/pages/responsesub/roadmap.pdf [ Links ]
2. WHO. Under-five mortality. available at http://www.who.int/gho/child_health/mortality/mortality under five text/en/index.html [ Links ]
3. WHO. Trends in Maternal Mortality: 1990 to 2010, 2012, available at http://www.unfpa.org/webdav/site/global/shared/documents/publications/2012/Trends in maternal mortality A4-1.pdf [ Links ]
4. WHO. Under-five mortality; Child Survival Call to Action: Ending Preventable Child Deaths; Government Signatories, available at http://apr.nationbuilder.com/government signatories [ Links ]
5. WHO. Children: reducing mortality. Fact Sheet No. 178, Sept. 2012, available at http://www.who.int/mediacentre/factsheets/fs178/en/ [ Links ]
6. It also initiated the use of public report cards to monitor progress and improve accountability. The website http://www.apromiserenewed.org/ provides data about the issue of child survival and information about the effort [ Links ]
7. Government Signatories, available at http://apr.nationbuilder.com/government_signatories [ Links ]
8. Levels and Trends in Child Mortality Report 2012. available at http://www.childinfo.org/files/Child_Mortality_Report_2012.pdf [ Links ]
9. Pan-American Health Organization. Health Situation in the Americas: Basic Indicators 2012. available at http://ais.paho.org/chi/brochures/2012/BI_2012_ENG.pdf [ Links ]
10. UN Maternal Mortality Estimation Inter-Agency Group. Maternal Mortality Estimates (2010). available at http://www.maternalmortalitydata.org/inner.html?country_selection=R [ Links ]
11. Economic Commission for Latin America and the Caribbean. Population, territory, and Sustainable Development Report. June 2012, available at http://www.eclac.org/publicaciones/xml/2/47342/Population.pdf [ Links ]
12. UNICEF, Statistics by country. available at http://www.childinfo.org/country_list.php [ Links ]
13. Latin American Center for Rural Development. Poverty and Inequality: Latin American Report 2011. available at http://www.ifad.org/pub/pl/informe_e.pdf [ Links ]
14. Demographic and Health Surveys (DHS), Multiple Indicator Cluster Surveys (MICS), Reproductive Health Surveys, mainly 2000-2008 (with further analysis by UNICEF, 2010); available at http://www.devinfo.info/pfc/mdg_4/3_mdg_4_u5mr.html [ Links ]
15. Black RE, Victora CG, Walker SP et al, and the Maternal and Child Nutrition Study Group. Maternal and child under nutrition and overweight in low income and middle-income countries. The Lancet. 2013, published online June 6, 2013; http://dx.doi.org/10.1016/S0140-6736(13)60937-X [ Links ]
16. Belizán JM, Cafferata M, Belizán M, Althabe F. Health inequality in Latin America. The Lancet. 2007;370: 1599-1600. [ Links ]
17. Pan American Health Organization. Health situation in the Americas: Basic Indicators 2012. available at http://ais.paho.org/chi/brochures/2012/BI_2012_ENG.pdf [ Links ]
18. WHO. Maternal and perinatal death. available at http://www.who.int/reproductivehealth/topics/maternal_perinatal/epidemiology/en/ [ Links ]
19. UNICEF, "Neonatal mortality," available at http://www.childinfo.org/mortality_neonatal.php [ Links ]
20. Child Health Epidemiology Research Group. Global Child Mortality: Estimates of Levels and Causes for 2000-2010. available at http://cherg.org/publications/Global-Child-Mortality-Estimates.pptx [ Links ]
21. World Bank, 2009. [ Links ]
22. Ahmed S, Qingfeng L, Liu L, Tsui A. Maternal deaths averted by contraceptive use: an analysis of 172 countries. The Lancet. July 12, 2012. [ Links ]
23. Bill and Melinda Gates Institute for Population and Reproductive Health. Family Planning Improving the Lives of Women and Their Families Around the World: 2011 Report. available at http://www.jhsph.edu/research/centers-and-institutes/bill-and-melinda-gates-institute-for-population-and-reproductive-health/_pdf/about/Gates%202011%20Report-110711.pdf [ Links ]
24. Guttmacher Institute and UNFPA. Latin America and the Caribbean: Facts on Investing in Family Planning and Maternal and Newborn Health. Dec. 2009, available at http://www.coe.ucsf.edu/coe/news/whe_pdf/FB-AIU-LAC.pdf [ Links ]
25. Stampini M, Tornarolli L. The growth of conditional cash transfers in Latin America and the Caribbean: did they go too far?. Inter-American Development Bank Policy Brief No. IDB-PB-185, Nov. 2012, available at http://idbdocs.iadb.org/wsdocs/getdocument.aspx?docnum=37306295 [ Links ]
26. The World Bank. Universal Healthcare on the rise in Latin America. Feb. 14, 2013. available at http://www.worldbank.org/en/news/feature/2013/02/14/universal-healthcare-latin-america [ Links ]
27. The World Bank. Latin America will grow in 2013 despite global crisis. Apr. 18, 2013. available at http://www.worldbank.org/en/news/feature/2013/04/18/economia-latinoamerica-2013 [ Links ]
28. The World Bank. Latin America and Caribbean Overview. available at http://www.worldbank.org/en/region/lac/overview [ Links ]
Nota
Este artículo puede ser consultado en versión completa en: http://www.medigraphic.com/inper

