











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
Sleep disturbances have been linked in a bi-directional way to impaired development, behavioral alterations, cognitive deficit and emotional alterations in children.1 The prevalence of sleep disturbances in children fall within a wide range, between 6 to 43%, depending on the parameters used to determine sleep disorders in some studies.2-5 However, complaints can be higher according to the National Sleep Foundation Poll, since 69% of parents reported that their children showed some sleep problems in the course of the week previous to the interview.6
Common sleep disturbances in children include the difficulty to initiate and maintain sleep, present between the 10 and 40%,7,8 daytime sleepiness, which has been reported to occur between 10 and 65%.9,10 Parasomnias also represent an important complaint, between 6.2 and 14.4%,the more frequent of them being night terrors, somniloquy, enuresis and bruxism.11-13 Respiratory problems during sleep can occur up to 7.5%,14 while sleep movement disorders, such as restless legs syndrome and periodic limb movement, occur between 2 and 23%.15,16 Overall, sleep disorders could affect more than 40% of children.7,17
The consequences of sleep disturbances in children include a decrease in academic performance and behavioral disorders.18-20 Likewise, daytime sleepiness increases the risk of suffering accidents.21,22 When sleep problems are not identified and treated in time, they have a negative impact on physical and mental performance and, more importantly, they represent a trigger factor for mood disorders.23,24
In general, sleep instruments for children mainly measure specific aspects like sleep breathing disorders, sleep habits or daytime sleepiness. Thus, the Pediatric Sleep Questionnaire (PSQ),25 is designed primarily for the detection of respiratory problems and the Pediatric Daytime Sleepiness Scale (PDSS) to detect somnolence.26 On the other hand, existing questionnaires that measure multiple domains are usually for parents. As an example, the Children’s Sleep Habits Questionnaire (CSHQ),27 which mainly measures: bedtime resistance, difficulty falling asleep, sleep duration, anxiety, waking up after initiating sleep, parasomnias, respiratory disorders and excessive daytime sleepiness, and the Sleep Behavior Questionnaire (SBQ),28 which includes factors like parasomnias, enuresis, fatigue, sounds while sleeping (teeth grinding or talking) and insomnia.
Self-report sleep instruments for children are scarce,29 yet they have a better correlation to objective measures of sleep, as shown by actigraphic techniques.30,31 Examples of questionnaires on which children have to inform about their sleep are the Sleep Self-Report (SSR),32 designed to measure similar domains as the CSHQ and the Children’s report of sleep patterns.33
On the other hand, as far as we know, there are not any available children sleep disturbances questionnaires or scales originally validated in the Mexican Spanish-speaking population. Existing instruments in Spanish are adapted versions of the Pediatric Sleep Questionnaire (PSQ),34,35 Sleep Self report (SSR)32 and the Children's Sleep Habits Questionnaire (CSHQ-SP).36
The high worldwide prevalence of sleep disturbances, their impact on school-age children,28,37-39, and the lack of valid scales for the Mexican children, justifies the need to design tools for sleep disturbances detection in this population. Under this framework, our goal was to get factorial validation of a scale for the screening of sleep disturbances in school-age children.
METHODS
Participants
Participants were children between the third and sixth grades of elementary school, recruited by convenience sampling. Schools were selected randomly from a list registered in the Secretariat of Public Education (SEP) of Yucatán, México. Participants were divided in two groups. The first group took part in the initial phase of the scale development and the second group comprised children to whom the final version of the instrument was applied.
Procedure
The study was approved by the Bioethics Committee of our research center. Afterward, the school authorities received an invitation to participate in the study. Both parents and children were informed about the purpose of the study and those who accepted, signed their consent and voluntary participation. The participants were also informed about the confidentiality of their responses. Administration of the scale was made by psychology students registered in their final year, who were previously trained by the main researchers. The children answered the instrument in their classrooms and during class schedules (7:00 am to 12:00 pm). Instructions were read aloud, and the answers were reviewed to avoid missing data. A researcher remained in each classroom to solve any questions. No participants had more than 5% of missing values; therefore, no case was excluded from the analysis. This process was the same for both groups.
Instrument
Sleep Disturbances Scale for School-age Children (EASE, for spanish acronym).
The methodology used for developing and validating the Sleep Disturbances Scale for School-age Children was based on that proposed by Nunnally, et al.40 and Streiner et al.41 The instrument was developed in two phases. The first one included the design and application of the pilot test. During the second phase the factorial structure of the scale was obtained as well as the prevalence of sleep disturbances of the sample.
The first version of the instrument consisted of 48 self-administered questions, aimed at identifying sleep disturbances according to those previously reported in the field, (CSHQ,27 PSQ,25 SBQ,28 PDSS,26 SSR,32. In the answer format the children indicated the number of days that each sleep disturbance occurred during the last week: 0 = 0 days, 1 = 1-2 days, 2 = 3-4 days, 3 = 5-6 days, and 4 = 7 days. To obtain the prevalence of sleep disturbances the following classification was used: without disturbance = 0 days, minor disturbance = 1-2 days, with disturbance ≥ 3 days a week. The instrument included a section of general data (gender, age, and grade), sleeping habitual place (bed or hammock) and other concerning sleep habits and schedules, where the children reported their typical bedtime and wake time in hours and minutes on both weekdays and weekends.
After statistical analysis of the pilot test, the EASE was re-designed, including 35 items (see below). Taking as reference the International Classification of Sleep Disorders (ICSD-2), nine factors were proposed: 1 insomnia, 2 daytime sleepiness, 3 sleep breathing problems, 4 nightmares, 5 night terrors, 6 somnambulism, 7 narcolepsy, 8 circadian rhythm disturbances and 9 parasomnia not specific.
Statistical analysis
For both pilot test and the final proposal of the EASE, the following analyses were made, according to classical psychometric methodology.40-42 Initially, a discrimination index of each item using the item-scale correlation was obtained. The criteria for approval for each item was a value of ≥ 0.25.
For the pilot test a factor analysis using principal components with orthogonal rotation (Varimax) was performed with all items of the scale. This analysis was attained to select the questions that would remain in the second version of the scale, for which four criteria were considered: 1 the items that were grouped within each factor had a conceptual relationship to each other, 2 a minimum factorial weight for each item ≥ 0.35, 3 an eigenvalue > 1 for the factor where the item was grouped and 4 Commonalities ≥ .040.
In the second phase, a principal components analysis with orthogonal rotation (Varimax) was performed with all items of the scale to determine the factorial structure of the EASE. The suitability and viability of the factorial analysis was established using the Kaiser-Meyer-Olkin (KMO) and Bartlett's test of sphericity. A factor analysis would be appropriate if the KMO test reached values above 0.5, and the Bartlett's test obtained values lower than 0.05. For the selection of factors that would constitute the final version of the EASE, four criteria were used: 1 eigenvalue greater than 1, 2) Commonalities ≥ .040, 3) factorial weight ≥ 0.35 and 4) Cronbach’s alpha coefficient ≥ 0.65. Reliability was examined using the internal consistency of the scale, which was analyzed using Cronbach’s alpha coefficient for the total scale and for each subscale. All statistical analyses were performed using SPSS statistical software version 19.0 (SPSS Inc., Chicago). A p-value of less than 0.05 (two-sided) was considered statistically significant.
RESULTS
Participants
We included 838 children between the third and sixth grades of elementary school. The first group took part in the initial phase of the scale development and included 314 children (30.1% were from rural areas, 69.9% from an urban regions), with an average age of 11.4 ± 2.0 years, 50.6% of them were girls. The second group comprised 524 children to whom the final version of the instrument was applied. This group was equally distributed by gender (51.1 % female, χ2 = 0.275, p = 0.60), with a mean age of 10.39 ± 1.3 years and range between 8 to 13 years old (35.7% were from rural areas, 64.3 % from urban areas). The distribution by grade (25.9% third, 22.6% fourth, 28.8% fifth and 22.6% sixth) was not statistically significant (p = 0.14). The percentage of children sleeping in a hammock was higher than those sleeping in bed (62% vs 38%, respectively, χ2 = 28.10, p= 0.001). All children were proficient in reading and writing, without difficulties in hearing and vision.
Pilot test analysis
All of the original 48 questions of the pilot scale were included for the factorial analysis, since all items approved the discrimination index criterion (≥0.25). After the factorial analysis of the 48 items only 29 were grouped in 7 factors, since they reached the 3 criteria established. The factors obtained from this first analysis were: nightmares and night terrors (α = 0.79), difficulty maintaining sleep due to organic symptoms (α = 0.69), insomnia environment (α = 0.72), sleep quality (α = 0.68), late insomnia (α = 0.69), daytime sleepiness (α = 0.61), insomnia stress (α = 0.67). As a result of this analysis, the scale was re-structured due to the fact that 19 items were not grouped in any factor and most of the sleep disturbances were related to insomnia. In order to obtain a better structure according to the ICSD-2 for the second version of the scale, 6 different questions were added. Thus, 35 items were assembled in the following nine factors: 1 insomnia, 2 daytime sleepiness, 3 sleep breathing problems, 4 nightmares, 5 night terrors, 6 sleepwalking, 7 narcolepsy, 8 circadian rhythm disturbances and 9 parasomnia not specific.
Factorial Structure and Reliability of the EASE
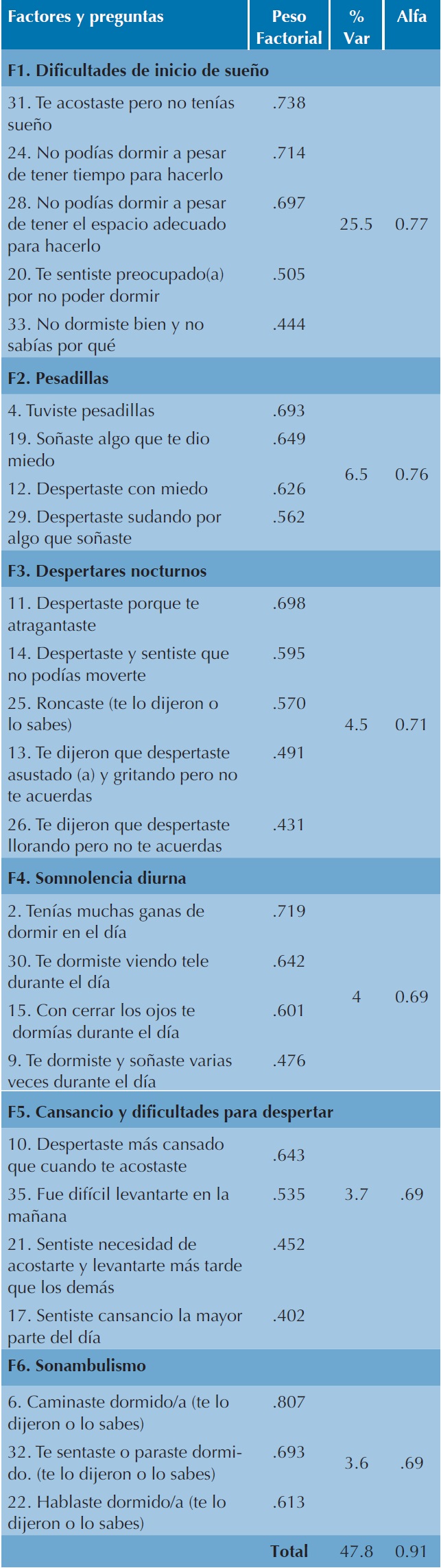
After application of the second version of the scale, all items approved the discrimination index criterion. Kaiser-Meyer-Olkin (KMO = 0.894) and Bartlett's tests (p = 0.001) results were adequate to continue with the factor analysis using principal components with orthogonal rotation. Items commonalities were in the range of 0.48 and 0.74 except for "You felt afraid of falling asleep during daytime", with a value of 0.34. Factorial Structure generated 9 factors from which 3 had to be eliminated because they did not approve the selection criterion and were not conceptually clear and did not include at least three questions. Removed factors were: narcolepsy, circadian rhythm disturbances and not specific parasomnia. In addition, “sleep breathing problems” and “night terrors” were united in a single factor renamed "nocturnal awakenings." As a result of the factorial analysis 10 questions were eliminated, and the final scale was integrated by 25 questions, with a structure of six factors: 1 difficulty initiating sleep, 2 nightmares, 3) nocturnal awakenings, 4) daytime sleepiness, 5 tiredness and difficulty waking up and 6) somnambulism. Appendix 1 shows the final version of the EASE.
The total percentage of the explained variance for the EASE was 47.8 %, being the first factor “difficulty initiating sleep” the one that obtained slightly over half of this percentage (25.5 %), whereas each one of the five remaining factors contributed between 6.5 and 3.6 % to the total variance. The factor that added the lowest variance was somnambulism. Likewise, the reliability level of the total scale obtained by the Cronbach’s alpha method was 0.91. The internal consistency by factors fluctuated between 0.77 and 0.69. The factor with the highest reliability was “difficulty initiating sleep” and the lowest was “somnambulism” Table 1).
Table 1 Factor Analysis and internal consistency (Cronbach´sα) of the EASE.
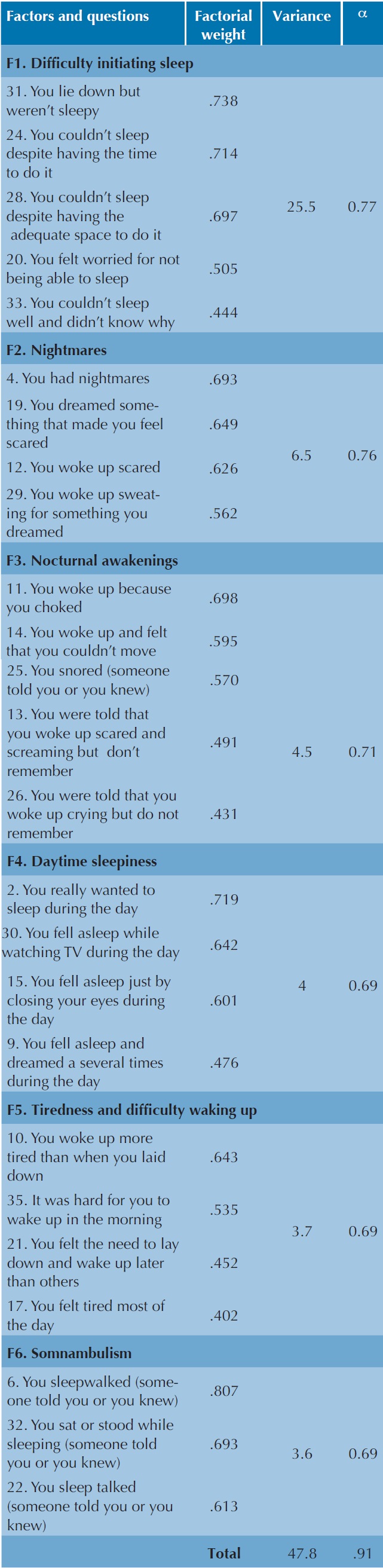
Note: Table 1 version in English is for informative value, since the development of the original instrument was is Spanish.
Cuadro 1. Análisis factorial y consistencia interna (α deCronbach) del EASE.
Prevalence of sleep disturbances
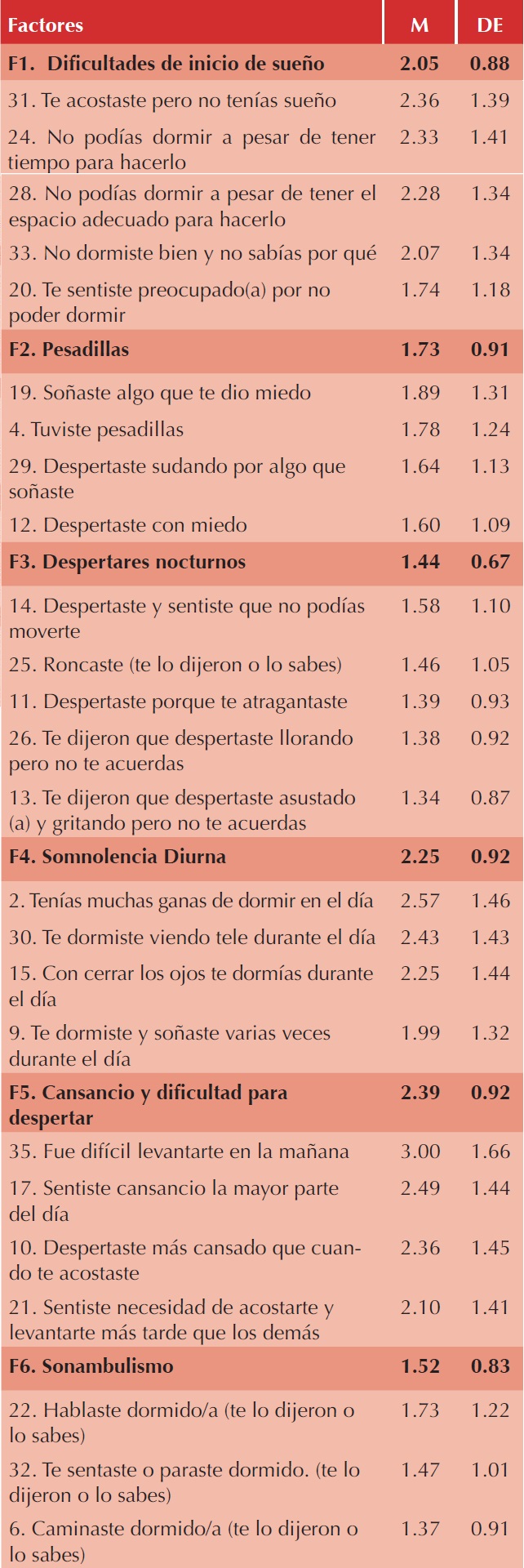
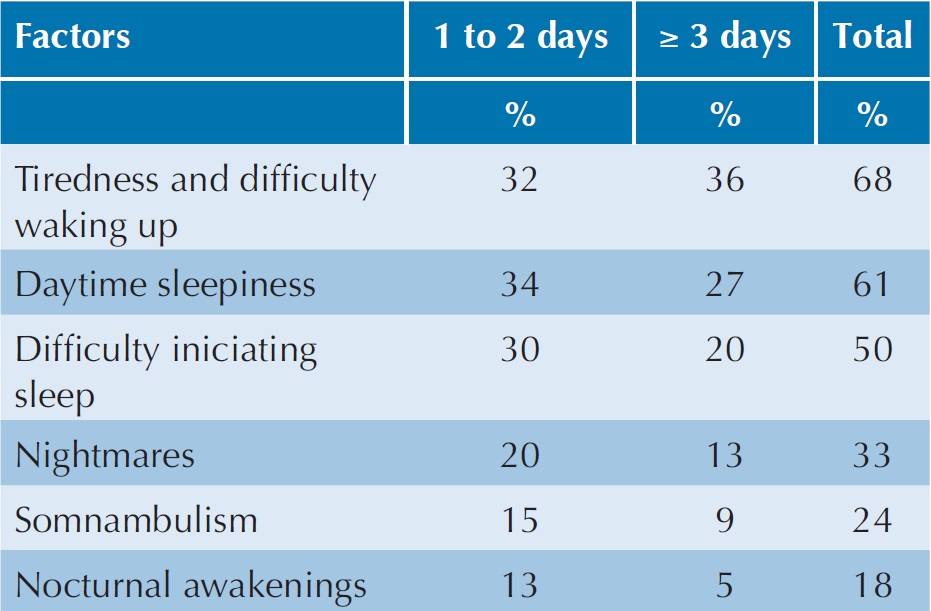
Descriptive data of each factor and corresponding questions are shown in Table 2. In general, factors were comprised within one standard deviation around the theoretical mean (2, in a scale from 0-4). On the other hand, general prevalence of sleep disturbances are depicted in Table 3. The sleep disturbance with the highest percentage of complaints was“tiredness and difficulty waking up”, present in 68% of cases, of which one third (32%) occurred between one to two days and 36% during 3 or more days a week. The second disturbance was “daytime sleepiness”, present in 61% of the sample. Furthermore, the disturbance with the lowest percentage of complaints was “nocturnal awakenings”, only present in 18%.
Table 2 Descriptive data of factors and questions of the EASE.
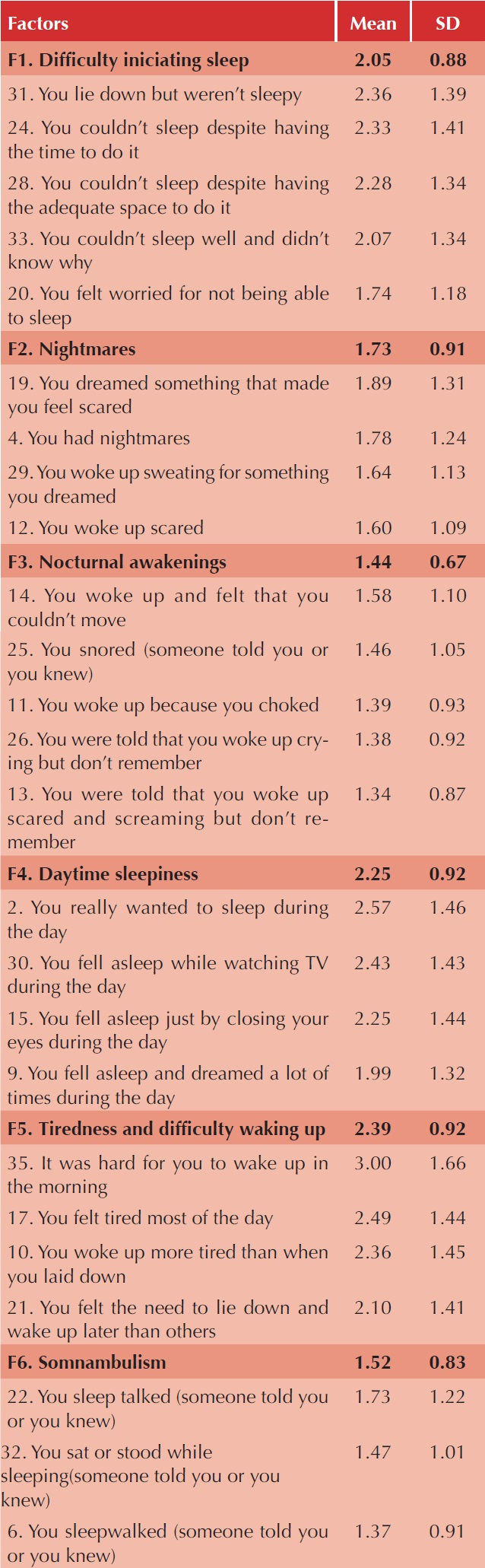
Note: Table 2 version in English is for informative value, sincethe development of the original instrument was is Spanish
Prevalence of sleep disturbances according to sociodemographic features in those children presenting sleep disturbances during ≥3 days a week are shown in Table 4. Thus, comparisons by sex revealed that “somnambulism” (χ2= 7.72, p = 0.005) and “nightmares” (χ2= 8.62, p = 0.003) were more prevalent in boys than in girls. Regarding age, there were significant differences in five factors, those who obtained the higher prevalence were the youngest children (p<0.05). Likewise, children living in urban regions presented more sleep disturbances than those from rural areas, in two factors: “difficulty initiating sleep” (25% vs 12.8%, χ2= 10.85, p= 0.001), and “somnambulism” (11.3% vs 4.8%, χ2= 6.20, p= 0.013). There were not significant differences in any factor between those sleeping in a hammock or bed.

DISCUSSION
The goal of this study was to obtain the factorial validation of a scale for the screening of sleep disturbances in Mexican, Spanish-speaking children. Results indicate that the EASE is a reliable and valid instrument for the detection of sleep disturbances in school-age children. Thus, the final version of the EASE includes six factors with a satisfactory variance percentage that is very similar to the Spanish versions of the SSR (46%), the PDSS (44%) and the SBQ (58.7%). Likewise, reliability of the scale had an alpha of 0.91, considered as a good measure of internal consistency,41 and was above the alpha value previously reported for the PSQ,35 CSHQ-SP,36 SSR,32 and PDSS.26
On the other hand, from the nine factors proposed for the theorist design of the scale, only six reached the statistical stablished criteria. However, those factors that were included correspond to the sleep disturbances comprised in the main existing questionnaires reported in the literature. For this reason, our scale could be a useful screening instrument for Spanish-speaking children, based on standard international criteria. Furthermore, in the current literature review we did not find self-report sleep instruments originally designed for Mexican children, thus the proposed scale could fulfill the need of instruments for our population.
Prevalence of the sleep disturbances showed that factors “tiredness and difficulty waking up” and “daytime sleepiness” were the children´s main complaints, with a high frequency, close to that (65%) previously reported in the literature.10.27,43 These disturbances are regularly found in children, and could be the result of other sleep problems occurring during the night, like breathing disorders, insomnia or parasomnias, which can alter both the quality and quantity of sleeping time.14,44-46 Sleep habits and sleep hygiene have been also related to daytime sleepiness and tiredness.47,48 On the other hand, “nocturnal awakenings” was the factor with the lowest percentage of complaints. This factor is composed by a section of questions related to breathing disorders during sleep, and parasomnias (night terrors and sleep paralysis), which had a similar prevalence to that reported in the literature.14,28
Differences related to both sex and age were found in our study. Boys presented more parasomnias than girls, and younger children had more disturbances compared to older kids, both situations had been previously reported in other cultures. 9,49 Our findings also showed differences between children from urban and rural areas. In particular, children living in Merida city showed increased levels of factors associated to sleep initiation difficulties and somnambulism. This situation could be related to the global increase in use of media devices such as computers, internet and mobile telephones by children with better socioeconomic status than those living in rural places.50-53 Nonetheless, it is important to consider that our sampled children from rural areas still showed a high prevalence of difficulties initiating sleep, situation which needs further studies. We also found differences in somnambulism prevalence between children from both areas, being lower in those living in rural places. A possible explanation could be that, though somnambulism is considered a common parasomnia, it is also increased by stress situations or influenced by sociocultural activities that are more frequently found in urban areas.54-56
In summary, the EASE is a self-report scale of sleep disturbances, with acceptable reliability and factorial validity in school-age children from southeast of Mexico. The EASE measures six factors proposed for research and clinical practice: 1) difficulty initiating sleep, 2) nightmares, 3) nocturnal awakenings, 4) somnambulism, 5) tiredness and difficulty waking up and 6) daytime sleepiness. The prevalence of sleep alterations obtained with the EASE was within the range found by other studies from different countries.

