










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkContaduría y administración
Print version ISSN 0186-1042
Contad. Adm vol.63 n.2 Ciudad de México Apr./Jun. 2018
https://doi.org/10.1016/j.cya.2016.07.003
Articles
Assessing the effect of service quality over user satisfaction in public health institutions in Mexico
1Tecnológico de Monterrey, EGADE Business School, México
The objective of this study is to offer an explanation of how service quality in public health institutions affects the beneficiary’s satisfaction with those institutions. Thirty-two quality attributes were identified in the service through an study and by analyzing the care received by the beneficiary in a primary care clinic. A structured scale was designed to measure the beneficiary’s perception of the performance of these attributes, as well as satisfaction indicators. A sample of 600 beneficiaries equitably divided between three institutions was collected. These were the Secretary of Health, the Mexican Social Security Institute (IMSS), and the Institute for Social Security and Services for State Workers (ISSSTE). Through a confirmatory factorial analysis, the attributes were grouped into seven service quality dimensions. In order to analyze the impact of these dimensions on satisfaction, six regression models and two structural models were carried out. These analyses showed that the quality of service provided by physicians and the quality of medication delivery services tend to be the factors with the greatest impact on beneficiary satisfaction. The quality of service provided by clinical analysis staff and the quality of the facilities also had a significant impact. However, factors such as quality of nursing services, quality of service provided by pharmacy staff, and quality of front desk service (assigning turns), did not have a statistically significant impact.
Keywords: Service quality; customer satisfaction; health care institutions
JEL Classification: M31; M39; I11; I18
El objetivo de este trabajo es ofrecer una explicación de los factores que tienen impacto en la percepción de satisfacción del derechohabiente del sistema público de salud. Mediante un estudio exploratorio y analizando el proceso de atención que recibe un derechohabiente en una clínica de primer nivel, se detectaron 32 atributos de calidad en el servicio. Se diseñó un cuestionario estructurado para medir la percepción sobre el cumplimiento de estos atributos, así como indicadores de satisfacción. Se integró una muestra de 600 derechohabientes dividida de forma equitativa entre tres instituciones: Secretaría de Salud, Instituto Mexicano del Seguro Social e Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado. Los atributos se integraron en siete dimensiones de calidad del servicio mediante un análisis factorial confirmatorio. Para analizar el impacto de estas dimensiones en la satisfacción se llevaron a cabo tanto seis modelos de regresión como dos modelos estructurales. Estos análisis arrojaron que la calidad del servicio proporcionado por los médicos, así como la calidad del servicio de la entrega de medicamentos, tienden a ser los factores de mayor impacto en la satisfacción del derechohabiente. Calidad del servicio del personal de análisis clínicos y la calidad de las instalaciones también tuvieron impactos significativos. Sin embargo, factores como calidad del servicio de los enfermeros(as), calidad del servicio del personal de farmacia, y calidad en la recepción (turnos), no tuvieron un impacto estadísticamente significativo.
Palabras clave: calidad en el servicio; satisfacción; instituciones de salud
Clasificación JEL: M31; M39; I11; I18
Introduction
The measurement of service quality has been a widely addressed topic in the marketing research literature. Although the context in which it is usually utilized involves service evaluation in service and product businesses including some form of customer service, it can also be used in the context of services that the State and the government provide to the general population, as observed in Scott and Shieff (1993), Donnelly et al. (1995), Andaleeb (2001), and Olin et al. (2014), among others.
Service quality has been established previously as a group of factors that tend to have a significant effect on satisfaction and client/user retention (Taylor and Baker, 1994; Spreng and Mackoy, 1996; Zeithaml et al., 1996). Thus, it has been widely documented that when a user perceives that the attributes being offered are adequately performed, this helps create the perception of his expectations being met, as well as a general feeling of satisfaction. Consequently, this study is theoretically contextualized in the relationship between service quality and customer satisfaction.
According to Gomez et al. (2011), the Mexican health system is composed of two large sectors: public and private. In turn, the public sector is composed of two types of institutions, social security institutions on the one hand, to which employees of established companies are entitled, and on the other, the organizations and programs that treat the population lacking access to social security. Within the social security group, there is the Mexican Social Security Institute (Spanish acronym, IMS), which assists approximately 80% of this type of beneficiaries, the Institute for Social Security and Services for State Workers (Spanish acronym, ISSSTE), Petróleos Mexicanos (PEMEX), the Secretary of National Defense (Spanish acronym, SEDENA), and the Secretary of the Navy (Spanish acronym, SEMAR) among others. In organizations for the population lacking access to social security (people who do not have a “recognized” economic activity), there is the Secretary of Health (Spanish acronym, SSA), the state health services (Spanish acronym, SESA), the IMSS-Oportunidades program (Spanish acronym, IMSS-O), and the Seguro Popular de Salud (Spanish acronym, SPS).
The aim of this study was to focus on the primary care2 clinics of the three main public health institutions: IMSS and ISSSTE in the social security subsector, and SSA (from the group assisting the population lacking access to social security). This study offers an approach to identifying the service quality attributes present in the process of providing care to the beneficiary in these types of State institutions. Therefore, the purpose of this study is to determine and explain the effect of the quality dimensions of the service provided in this type of institutions concerning the satisfaction of the beneficiary, in addition to differentiating the dimensions that have the biggest impact on said satisfaction. Thus, this work contributes to the understanding of user satisfaction regarding this type of services, and to the identification of the aspects of the service that can be improved to increase the perception of satisfaction of the beneficiaries.
Service quality
To improve the quality of a service it is necessary to know what it is and how to measure it. Quality in service tends to be more difficult to establish and measure than the quality of a product (Parasuraman, Zeithaml and Berry, 1985), mainly due to the intangibility and heterogeneity of services. Service quality began to receive greater attention in the 1980s. It was then that some of the primary authors on service quality proposed definitions and began introducing ways to measure it (Oliver, 1980; Parasuraman et al., 1985; Gronroos, 1984). As a general tendency, service quality is not measured with regard to the standards established by the company, but rather from the perspective of the clients or users (Asubonteng, Mc Vleary and Swan, 1996).
One of the most widely used definitions in the literature is by Parasuraman et al. (1988, p. 16), who propose that quality in service is “a judgement or attitude in relation to the general excellence or superiority of the global service”. Consistently with this, Dagger et al. (2007) propose that the measurement of service quality in health organizations could be done using four statements: the general service quality provided by the clinic is excellent; the service quality provided in the clinic is impressive; the service offered by the clinic is of a high level; the clinic offers a service that is superior in every respect.
Measuring service quality
For measurement purposes, the quality of a service has been proposed as a multidimensional construct, that is, the clients do not only evaluate the result they obtain from an organization; in their evaluation, they also consider a series of dimensions that they perceive throughout the entire process of the service (Parasuraman et al., 1985). The first instrument proposed in the literature to measure the quality of a service in a generalized manner is SERVQUAL, designed by Parasuraman et al. (1988). This instrument proposes to measure the compliance and significance of 22 attributes grouped into five dimensions: tangibles, assurance, response, empathy, and trust. Asubonteng et al. (1996) report numerous applications of the SERVQUAL instrument in health services within less than ten years after having been published. However, considerable criticism has been received on how adequate it is to use this same instrument for all different types of services. In other words, some authors state that not all services have the same basic characteristics and, therefore, specific instruments have been developed that focus on different industries (See: Babakus and Boller, 1992; Van Dyke et al., 1997; Jabnoun and Khalifa, 2005; Akbaba, 2006; Caro and García, 2007; Vázquez, 2015).
Taylor and Cronin (1994) note that in the marketing of health services one must be extremely careful in the application of general scales used for other services, such as SERVQUAL and SERVPERF, because there is a high risk of these being erroneously translated into the context of health care. There are studies in the literature that have adapted the SERVQUAL instrument to this sector (Taylor and Cronin, 1994; Kesuma et al., 2013) but there are also authors, within the health sector, that propose specific dimensions (Woodside et al., 1989; Hill and McCrory, 1997; Dagger et al., 2007; Lis et al., 2011; Haque et al., 2012; Kumaraswamy, 2012; Amin and Siti, 2013). The specific dimensions for the service quality of health centers mentioned above are summarized in Table 1.
Table 1 Studies that address service quality in health institutions and its impact on the behavior of the user
| Author | Service quality dimensions | Dependent variable |
| Woodside et al.,1989 | Admission. Nursing care. Meal service. Cleaning and maintenance. Technical service. Discharge from the hospital. | Satisfaction Intent to return |
| Taylor and Cronin,1994 | SERVQUAL dimensions adapted to hospitals. | Satisfaction |
| Hill and McCroy, 1997 | Clinical factors: Safety. Hygiene. Communication. Pain relief. Non-clinical factors: Bathroom availability. Comfort of the beds. Quality of the sheets. Availability of public phones. Quality of the food. | n/a |
| Dagger et al., (2007) | Interpersonal quality: Interaction. Relations. Technical quality: Results. Experience. Environmental quality: Atmosphere. Tangibles. Administrative quality: Opportune moment. Operation. Support. | Satisfaction Intent to return |
| Lis et al., (2011) | Operations and services. Multidisciplinary team for patient care. | Recommendation to others |
| Atta (2012) | SERVQUAL dimensions adapted to hospitals. | Satisfaction |
| Haque et al., (2012) | Support personnel. Hospital facilities. Customer service. | Satisfaction |
| Kumaraswamy (2012) | Behavior of the physician. Support personnel. Atmosphere. Operative performance. | Satisfaction |
| Amin and Siti (2013) | Admission. Medical service. General service. Medical discharge. Social responsibility. | Satisfaction Intent to return |
| Kesuma et al., (2013) | SERVQUAL dimensions adapted to hospitals. | Loyalty CRM |
In this study, the measurement of service quality is done following the proposal of Cronin and Taylor (1994), in which they note that it is more appropriate to measure service quality by asking solely about the performance of each attribute than by also incorporating the measurement of the expectations of the client concerning each attribute, as proposed by Parasuraman et al. (1988). According to Parasuraman et al. (1988) service quality is the discrepancy between the performance of the attribute and the expectations that are held of it. However, Cronin and Taylor (1994) find evidence that this form of measurement generates stability and reliability problems, and obtain better measurement indicators by assessing performance alone.
The effect of service quality on dependent variables
As has already been mentioned, service quality has been proposed as an antecedent to client satisfaction and loyalty to a brand or organization (Knutson et al., 1991; Taylor and Baker, 1994; Stevens et al., 1995; Spreng and Mackoy, 1996; Dabholkar et al., 1996; Zeithaml et al., 1996; Chi-Cui et al., 2003; Gounaris, 2005; Tsoukatos and Rand, 2007; Ryu and Han, 2010; Ryu et al., 2012; Orel and Kara, 2014; Bruwer, 2014; Bansal and Taylor, 2015; De Oña et al., 2015). The case of health centers is no exception. In recent years, studies have been carried out to empirically corroborate the relationship of service quality with the satisfaction and loyalty of the user in this sector (Babakus and Mangold, 1992; Taylor and Baker, 1994; Atta, 2012; Haque et al., 2012; Kumaraswamy, 2012; Amin and Siti, 2013; Kesuma et al., 2013).
Often, the concepts of service quality and satisfaction are confused, or may overlap. In the area of health services, Woodside et al. (1989) presents the satisfaction of the patient as a type of attitude, since it is the reflection of how much a patient likes or dislikes the service after an experience in hospital. They find that satisfaction is given based on the perceived service quality. Nevertheless, service quality and satisfaction are understood as different constructs. John (1992) explains the difference between both constructs by noting that to measure satisfaction it is recommended to do so with a single general dimension, whereas service quality is better measured with a scale such as SERVQUAL, which operates by splitting service up into various attributes. In the health services sector, when determining the effect of service quality on the loyalty or attachment of the user to the institution, in most cases, an acceptable indicator of loyalty has been the intent to return to the institution (Dagger et al., 2007; Amin and Siti, 2013), and not necessarily the observed action of returning.
Table 1 shows chronologically the service quality dimensions that have been previously proposed in studies that address the measurement of service quality in health care institutions. The first column of this table shows the authors and publication date, the second lists the dimensions proposed, and the third shows the behavior dependent variables on which the service quality dimensions would have an effect.
Table 1 shows that the service quality dimensions previously utilized vary significantly from the service quality dimensions implemented in this study (as will be seen below). This is because most previous works focus on the service quality of private health centers, where the care process varies considerably from that observed in public health institutions. One of the new elements provided by this study is that it was carried out in the latter type of institution.
Approach
A preliminary study was carried out to identify the relevant service quality attributes for the beneficiaries of the public health sector in primary care clinics. As part of this preliminary study, we reviewed the complete process through which a beneficiary goes on a normal day when receiving medical attention. Following this process, the attributes that the beneficiaries expected to meet were investigated. Thus, it was determined that, in general terms, user care in the three institutions addressed in this work (IMSS, ISSSTE, SSa) comprises the following seven elements divided according to waiting times: reception and turn request (numbered ticket), initial contact with a nurse for the collection of information, care from the physician, service provided by the pharmacy staff, quality aspects in the delivery of medication, service provided by the clinical analysis staff, and quality of the facilities. Specific service quality attributes were identified for each of these aspects through thirty-six in-depth interviews with beneficiaries who regularly go to these institutions for medical attention. These attributes are shown in Table 2.
Table 2 Confirmatory factorial analysis of the dimensions of the model. Oblique rotation (non-orthogonal). Factorial loads (standard matrix)
| Service quality attributes | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| Experience of the nurses who cared for you | .84 | |||||||
| Level of care provided to you today by the nurse | .79 | |||||||
| Courtesy of the nurses who cared for you | .77 | |||||||
| Clarity of the explanations provided by the nurses | .75 | |||||||
| Level of knowledge of the nurse(s) | .75 | |||||||
| Knowledgeability of the physician who cared for you today | .80 | |||||||
| Experience of the physician who cared for you today | .75 | |||||||
| Level of care provided to you today by the physician | .70 | |||||||
| Courtesy of the physician who cared for you today | .70 | |||||||
| Clarity of the explanations given by the physician | .69 | |||||||
| Delivery at the pharmacy of the complete dose of the prescribed medication | .83 | |||||||
| Delivery at the pharmacy of all the medication prescribed by the physician | .82 | |||||||
| Good state of the medication delivered | .78 | |||||||
| Knowledgeability of the staff performing clinical analyses | -.87 | |||||||
| Experience of the staff performing clinical analyses | -.79 | |||||||
| Clarity of explanations provided by staff performing clinical analyses | -.70 | |||||||
| Courtesy of staff performing clinical analyses | -.68 | |||||||
| Level of care of staff performing clinical analyses | -.66 | |||||||
| Clarity of explanations provided by staff assigning turns/appointments | .83 | |||||||
| Level of care of staff assigning turns/appointments | .81 | |||||||
| Level of care provided by receptionists | .73 | |||||||
| Clarity of the explanations provided by the receptionists | .72 | |||||||
| Service quality received vs. the ideal | -.81 | |||||||
| General satisfaction with the service received today | -.80 | |||||||
| Service quality received vs. expectations | -.78 | |||||||
| Quality of the facilities | .68 | |||||||
| Image of the facilities | .64 | |||||||
| Cleanliness of the facilities | .63 | |||||||
| Comfort level of the facilities | .60 | |||||||
| Cleanliness of the medical equipment | .59 | |||||||
| Functionality of the medical equipment | .56 | |||||||
| Treatment by the security guards | ||||||||
| Courtesy of the person who assisted you in the pharmacy | .83 | |||||||
| Care provided by the pharmacy staff who assisted you today | .80 | |||||||
| Knowledgeability of the person who assisted you in the pharmacy | .71 |
Solution of 35 variables on 8 components with eigenvalues greater than 1 that explain the 70.3% of the original variability. Extraction method: Analysis of main components. Rotation method: Oblimin with Kaiser standarization. Rotation converged in 16 iterations.
Based on the above, it was surmised that these aspects of service quality may have a direct positive effect on the satisfaction of the beneficiary. As mentioned above, it has been previously established that service quality can be an important antecedent of user satisfaction (Knutson et al., 1991; Taylor and Baker, 1994; Stevens et al., 1995; Spreng and Mackoy, 1996; Dabholkar et al., 1996; Zeithaml et al., 1996; Chi-Cui et al., 2003; Gounaris, 2005; Tsoukatos and Rand, 2007; Ryu and Han, 2010; Ryu et al., 2012; Orel and Kara, 2014; Bruwer, 2014; Bansal and Taylor, 2015; de Oña et al., 2015). Similarly, the relationship between service quality as an antecedent of patient satisfaction has been proven concretely in health services (Babakus and Mangold, 1992; Taylor and Baker, 1994; Atta, 2012; Haque et al., 2012; Kumaraswamy, 2012; Amin and Siti, 2013; Kesuma et al., 2013), although not specifically in state primary clinics and institutions. Therefore, seven hypotheses were posed, in accordance with which each of these seven service quality dimensions is expected to have a positive effect on beneficiary satisfaction. The seven hypotheses are outlined in Figure 1.
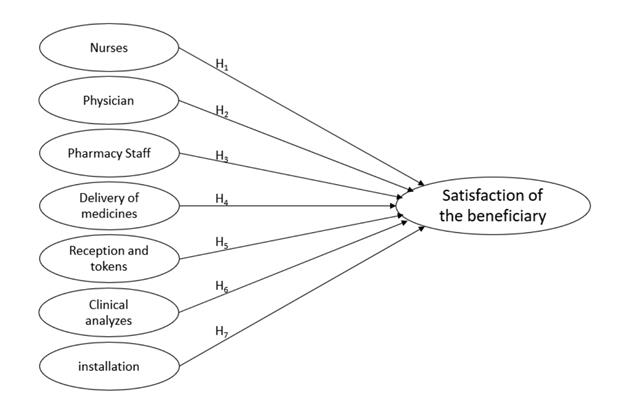
Although these types of studies typically present satisfaction as a mediating factor between service quality and customer loyalty, in this case the relationship is only posed between service quality (as independent variables) and satisfaction as a final dependent variable. This is due to the fact that in the health sector institutions of the State, the beneficiary has little opportunity to choose the institution that will meet his health needs. In Mexico, a state worker is obligatorily registered in the ISSSTE, while a private sector worker is registered in the IMSS. Hence, those citizens who do not have access to social security are left with the SSa or the Seguro Popular as their only state-provided options. Therefore, we did not implement any variables related to the preferences and intentions of the beneficiary. However, although the beneficiary has limited choices, the position here is that it should be the obligation of the state, and of these institutions, to provide the best possible service to the affiliates.
Methodology
Given that part of the purpose of the study was to evaluate the service being offered to beneficiaries, a study with a non-experimental post hoc casual design was carried out (cf.,Kerlinger, 1979). To this end, structured interviews were conducted through a questionnaire. The design of this questionnaire was made possible by means of thirty-six in-depth interviews carried out with beneficiaries, as mentioned above. The purpose of these first interviews was to identify relevant service quality attributes that people expect to be met in the service they receive from the primary care clinic they regularly attend. A total of thirty-two attributes were identified. The list of these attributes can be observed in Table 2. The items used to measure the compliance with each of these attributes, as they appear in the survey, can be observed in Table 3. These items were associated to six-point Likert scales (excellent, very good, good, poor, very poor, terrible). The questionnaire was designed for use in a face-to-face interview using graphic supports to show the respondent the response options for each item.
Table 3 Items (observable variables) per component (latent variables) and reliability of the measurements
| Dimension (latent variable) | Indicator (observed variable) | Alpha (α) |
| Nurses | How do you consider the attention given by the nurse who cared for you today? How do you perceive the level of knowledge of the nurses who cared for your today? How do you perceive the level of experience of the nurses caring for you? How do you perceive the courtesy of the nurses caring for you? How do you consider the clarity of the explanations given by the nurses caring for you? | .92 |
| Physicians | How do you consider the attention given by the physician who cared for you today? How do you perceive the level of knowledge of the physician who cared for you today? How do you perceive the level of experience of the physician who cared for you today? How do you perceive the courtesy of the physician who cared for you today? How do you consider the clarity of the explanations given by the physician who cared for you today? | .93 |
| Pharmacy staff | How do you consider the attention given by the pharmacy staff that served you today? How do you perceive the level of knowledge of the person who served you in the pharmacy? How do you perceive the courtesy of the person who served you in the pharmacy? | .92 |
| Delivery of medicaments | I found all the medicaments prescribed by the physician in the pharmacy today. When they delivered my medicaments, I received the complete dose. The medicament I received at the end of my appointment is in good state. | .81 |
| Receipt and delivery of turns | How do you consider the attention of the personnel in charge of turns/appointments? How do you consider the clarity of the indications given by the personnel in charge of turns/appointments? How do you consider the attention given by the receptionists? (people who let you in, weight and measure you) How do you consider the clarity of the indications given by the receptionists? | .89 |
| Clinical analyses | How do you consider the attention given by the personnel who carried out your clinical analyses today? How do you perceive the level of knowledge of the personnel who carry out the clinical analyses? How do you perceive the level of experience of the personnel who carry out the clinical analyses? How do you perceive the courtesy of the personnel who carry out the clinical analyses? How do you consider the clarity of the explanations given by the personnel who carry out the clinical analyses? | .89 |
| Facilities | Do you consider that the facilities (offices, waiting room, bathrooms, cafeteria) are...? Do you consider that the cleanliness of the Institution is...? Do you consider that the image of the Institution is...? Do you consider that the comfort of the Institution is...? How do you consider the functionality of the medical equipment? (beds, scales, stethoscope, chairs) Do you consider that the cleanliness of the medical equipment is...? | .87 |
| Satisfaction (Y) | In general, I feel satisfied with the service I received today. The service I received today met my expectations. The service I received today was ideal. | .93 |
Alpha (α) Cronbach’s alpha internal reliability coefficient
A sample of n=600 beneficiaries was established. These beneficiaries were selected according to suitability and divided in an equitable manner between the three institutions utilized in this study (IMSS, ISSSTE and SSa). The manner in which the clinics for the interviews were selected was meant to ensure a territorial coverage throughout the entire Mexico City. The interviews were carried out in primary care clinics of these three institutions. Since it was requested that the respondents evaluate the complete service received on the day in question, the interviewers had to ask the beneficiaries to respond to the interview once the care process was finished (reception-turn-information/nurse-waiting-physician-waiting-delivery/ medication). The beneficiaries who responded were selected by interception inside the clinic or as they were leaving. The clinics selected for carrying out the interviews are distributed throughout different areas of the Mexico City. Efforts were made to choose clinics within each of the municipalities that compose this city.
Preliminary data analysis
For the data analysis, we first carried out a confirmatory factorial analysis to corroborate a coherent separation of the attributes, including the satisfaction measurements. In this manner, seven service quality components (dimensions) were generated along with a satisfaction dimension that subsequently functioned as the latent dependent variable in the structural analysis. The integration of these components, the product of a factorial analysis, can be observed in Table 2. This coherent separation tends to confirm the items’ measurement validity and the existence of the resulting dimensions (latent variables).
For this factorial analysis, and to achieve the separation of components, an oblique rotation that does not ensure orthogonality (zero correlation between components) was used. This rotation method was selected because the satisfaction component had to be subsequently used as a dependent variable, such that a zero correlation with the rest of the components was not wanted. Nevertheless, the structural analysis is well supported, and in some cases a certain correlation between latent independent variables as a common phenomenon is assumed. Thus, when interpreting the content of the components with regard to the factorial loadings of each of the attributes, it was determined that the components obtained are the following:
Service quality provided by the nurses (X1)
Service quality provided by the physicians (X2)
Service quality provided by the pharmacy staff (X3)
Service quality in the delivery of medicaments (X4)
Service quality in the receipt and delivery of turns (X5)
Service quality regarding clinical analyses (X6)
Perceived quality of the facilities (X7)
Satisfaction of the beneficiaries (Y)
Of these eight components, seven correspond to the service quality dimensions mentioned in the “approach” section above. These seven service quality dimensions are used here as latent independent variables in each of the seven previously established hypotheses. The eighth dimension (satisfaction) would correspond to the latent dependent variable in these hypotheses. The items grouped in these eight dimensions (latent variables) can be observed in Table 3.
Measurements
To confirm the reliability of the measurements, reliability analyses were carried out using Cronbach’s alpha. For these analyses, the reliability index was obtained for the items (attributes) that comprise each of the dimensions obtained in the factorial analysis in Table 2, which are subsequently used as observed variables in the structural analysis. Cronbach’s alpha is a highly reliable statistic to determine the internal consistency of unidimensional multiple item components (Gliem and Gliem, 2003), as done in this study. Table 3 shows that, in the items associated to each dimension (latent variables), values in the alpha coefficient were obtained, suggesting high levels of internal consistency in the measurement according to Darren and Mallery (2003, p. 231), and Gliem and Gliem (2003).
The items utilized here to measure satisfaction are consistent with those in previous studies, as can be observed in Zeithaml et al. (1996), Oliver (1999), Baumann et al. (2007), and Ryu et al. (2012), as well as many others. Although different models have been proposed to measure satisfaction, the items utilized in this study are consistent with the approach proposed by Westbrook (1980) in which satisfaction is considered a global affective response to the service provided. This affective response is the result of the comparison between what is obtained from a service and previous expectations (Halstead, Hartman and Schmidt, 1994).
Results: descriptive analysis and regression models
Table 4 shows the descriptive results of the study. It can be observed that there were significant differences between institutions in most of the measured attributes. The highest values were obtained between two of the three institutions used in this work. To confirm the differences between the institutions, difference tests were used for independent samples. Each independent sample corresponds to the beneficiaries of each of the institutions. To this end, two different tests were used. On the one hand, a parametric test, a one-way ANOVA for testing differences. To confirm the differences, and to preclude the need for discussion on the level of measurement and the normality of the data due to it coming from attitude scales, a non- parametric test was also used, the Kruskal-Wallis test for distribution differences. As can be observed in Table 4, the results of both tests confirm each other in every case except for one of the satisfaction measurements.
Table 4 Results by institution per item. Averages, standard deviations, and difference tests between institutions
| Institution | |||||||||||
| IMSS | ISSSTE | SSA | |||||||||
| Item (observed variable) | ẋ | s | ẋ | s | ẋ | s | auf | kw | |||
| Overall quality of this facility | 4.13 | .88 | 4.02 | .73 | 4.08 | .99 | - | - | |||
| Cleanliness of this facility | 4.08 | .93 | 3.85 | .71 | 4.23 | .87 | *** | *** | |||
| Image of this facility | 4.08 | .94 | 3.87 | .75 | 4.08 | .88 | * | ** | |||
| Comfort of the facilities | 4.00 | .86 | 3.77 | .80 | 3.90 | 1.10 | * | * | |||
| Functionality of the medical equipment | 4.13 | .88 | 3.92 | .79 | 4.45 | .87 | *** | *** | |||
| Cleanliness of the medical equipment | 4.27 | .77 | 3.97 | .72 | 4.55 | .73 | *** | *** | |||
| Care provided by the physician who saw you today | 4.59 | .86 | 4.25 | .78 | 4.80 | .82 | *** | *** | |||
| Knowledgeability of the physician who saw you today | 4.67 | .83 | 4.19 | .84 | 4.92 | .80 | *** | *** | |||
| Experience of the physician | 4.67 | .90 | 4.19 | .88 | 4.92 | .83 | *** | *** | |||
| Courtesy of the physician | 4.60 | 1.01 | 4.18 | .92 | 4.78 | .83 | *** | *** | |||
| Clarity of the explanations given by the physician | 4.57 | .96 | 4.15 | .90 | 4.72 | .84 | *** | *** | |||
| Care provided by staff in charge of assigning turns/appointments | 4.06 | 1.02 | 3.67 | .92 | 4.08 | .78 | *** | *** | |||
| Clarity of the explanations provided by staff in charge of assigning turns/appointments | 4.18 | .91 | 3.74 | .82 | 4.08 | .81 | *** | *** | |||
| Care provided by the receptionists | 4.23 | .88 | 3.78 | .86 | 4.05 | .73 | *** | *** | |||
| Clarity of explanations provided by the receptionists | 4.20 | .90 | 3.83 | .82 | 4.05 | .69 | *** | *** | |||
| Care provided by the nurse who tended to you | 4.33 | .81 | 4.18 | .81 | 4.49 | .77 | ** | ** | |||
| Knowledgeability of the nurses who tended to you | 4.33 | .83 | 4.17 | .69 | 4.59 | .73 | *** | *** | |||
| Experience of the nurses | 4.33 | .83 | 4.18 | .69 | 4.57 | .73 | *** | *** | |||
| Courtesy of the nurses | 4.28 | 1.07 | 4.17 | .79 | 4.47 | .77 | ** | ** | |||
| Clarity of the explanations provided by the nurses | 4.32 | .93 | 4.10 | .77 | 4.46 | .71 | *** | *** | |||
| Treatment by the security guards | 4.28 | .82 | 4.12 | .74 | 3.84 | 1.00 | *** | *** | |||
| Assistance provided by the pharmacy staff | 4.09 | .96 | 3.84 | .82 | 4.33 | .62 | *** | *** | |||
| Knowledgeability of the pharmacy employee | 4.09 | .95 | 3.89 | .79 | 4.26 | .72 | *** | *** | |||
| Courtesy of the pharmacy employee | 3.94 | 1.10 | 3.84 | .87 | 4.39 | .61 | *** | *** | |||
| Assistance provided by the staff performing clinical analyses | 4.40 | .86 | 3.96 | .76 | 4.36 | .65 | *** | *** | |||
| Knowledgeability of the staff performing clinical analyses | 4.57 | .78 | 4.06 | .68 | 4.37 | .61 | *** | *** | |||
| Experience of the staff performing clinical analyses | 4.67 | .74 | 4.02 | .75 | 4.39 | .60 | *** | *** | |||
| Courtesy of the staff performing clinical analyses | 4.38 | .75 | 4.05 | .76 | 4.35 | .59 | ** | ** | |||
| Clarity of the explanations provided by the staff performing clinical analyses | 4.52 | .68 | 4.07 | .79 | 4.38 | .67 | *** | *** | |||
| I found the medication prescribed by the physician in the pharmacy | 4.43 | 1.67 | 4.26 | 1.50 | 4.37 | 1.38 | - | - | |||
| I received the complete prescribed dose of medication | 4.77 | 1.52 | 4.42 | 1.41 | 4.73 | 1.20 | * | ** | |||
| The medication I received is in good condition | 5.37 | 1.01 | 4.86 | 1.05 | 5.15 | .93 | *** | *** | |||
| I am satisfied with the service I received today | 4.69 | 1.21 | 4.50 | 1.24 | 4.91 | .83 | ** | ** | |||
| The service met my expectations | 4.65 | 1.24 | 4.42 | 1.28 | 4.70 | .96 | * | - | |||
| The service I received was ideal | 4.40 | 1.29 | 4.11 | 1.29 | 4.62 | .99 | *** | *** | |||
ẋ average (averages in bold indicate the highest value per variable)
s: standard deviation The averages correspond to possible scores between 1 and 6, where 1 refers to the lowest value and 6 to the highest.
auf: Difference test of Anova averages of a factor. Significant differences *at .05, **at .01, ***at .001
kw: Kruskal-Wallis test for various independent samples. Significant differences * at .05, **at .01, ***at .001
In order to obtain a first approximation of a causality analysis, three models were generated using the analysis of multiple regression. For these models, the dependent variables used were the three satisfaction measurements. The seven service quality dimensions were used as independent variables, synthetized through the factorial analysis with oblique rotation. These can be observed in Tables 2 and 3.
The results of these regression analyses can be observed in Table 5. Of the seven independent variables, four were significant (physicians, pharmacy, medication and facilities) for two of the satisfaction measurements (general satisfaction and expectations met). For the third satisfaction measurement (ideal) only two independent variables were significant (medication and assignment of turns).
Table 5 Linear regression analysis. Satisfaction measurements as dependent variables. Standardized coefficients.
| Model 1 Y1 I feel satisfied | Model 2 Y2 Met the expectations | Model 3 Y3 The service was ideal | Z | |
| R | .62 | .63 | .50 | |
| R2 adjusted | .37 | .37 | .22 | |
| F | 17.47*** | 17.65*** | 9.06*** | |
| X1 Nurses | .06 | .12 | .07 | 1.56* |
| X2 Physicians | .22** | .13* | .12 | 1.19 |
| X3 Pharmacy | .17** | .14* | .11 | 1.48* |
| X4 Medicaments | .34*** | .31*** | .20** | 0.96 |
| X5 Reception/turns | .04 | -.03 | -.16* | 1.01 |
| X6 Clinical analyses | .08 | .09 | .12 | 1.71* |
| X7 Facilities | .25*** | .27*** | .08 | 1.37 |
*Significant at .05, **Significant at .01, ***Significant at .001
Z: Kolmogorov-Smirnov normality test. H null: The distribution is normal
Table 5 also shows normality indicators of the independent variables used in the linear regression models. These indicators show that not all of the independent variables comply with the normality criteria (though the difference is not much). This could generate suspicions as to the validity of these linear regression analyses, since normality of the variables is one of the basic assumptions associated with the regression analysis. Although this is debatable, some may consider it an indispensable requirement. To handle this possible conflict, the decision was made to offer in addition an ordinal logistic regression analysis, which assumes neither linearity nor normality. Table 6 shows the results of three ordinal regression models, each of which corresponds to the dependent variables used in the linear regression models in Table 5. Generally, the three ordinal regression models show adequate indicators to intercept them. Thus, it is confirmed that the independent variables tend to have an effect on the dependent ones, and it can be observed that the data fit the model well. Only with respect to the parallel lines test did Model 6 fail to meet this criterion.
Table 6 Ordinal logistic regression analysis. Satisfaction measurements as dependent variables. Model indicators. Pseudo-R2 coefficients of determination. Estimator parameters of the independent variables.
| Model 4 Y1 I feel satisfied | Model 5 Y2 Met the expectations | Model 6 Y3 The service was ideal | |
| Model fit | 101.2*** | 99.1*** | 52.5*** |
| Pearson’s goodness of fit | 785.8 | 996.4 | 867.8 |
| Deviance goodness of fit | 455.9 | 468.7 | 524.8 |
| Parallel | 31.06 | 16.5 | 48.9** |
| R2 Cox and Snell | .40 | .39 | .23 |
| R2 Nagelkerke | .42 | .41 | .24 |
| R2 McFadden | .18 | .18 | .09 |
| X1 Nurses | .17 | .38* | .20 |
| X2 Physicians | .59*** | .28 | .24 |
| X3 Pharmacy | .46** | .41** | .27* |
| X4 Medicaments | .87*** | .81*** | .45** |
| X5 Reception/turns | .17 | -.00 | -.34* |
| X6 Clinical analyses | .15 | .21 | .22 |
| X7 Facilities | .66*** | .66*** | .12 |
Model fit: Test ji2 to determine that there is an effect caused by the independent variables (must be significant)
Pearson goodness of fit: test to determine if the data fits the model (must not be significant)
Deviance goodness of fit: test to determine if the data fits the model (must not be significant)
Parallel: parallel lines test to determine equality of explanation on the dependent variable (must not be significant)
R2 C&S: R2 Cox and Snell coefficient to determine the degree of explanation on the dependent variable (0 to 1; .5 ≈ 50%)
R2 N: R2 Nagelkerke coefficient to determine the degree of explanation on the dependent variable (0 to 1; .5 ≈ 50%)
R2 Mc: R2 McFadden coefficient to determine the degree of explanation on the dependent variable (0 to 1; .5 ≈ 50%)
Estimators of the independent variables must be significant to conclude effect on the dependent variable *significant at 0.05 / **significant at 0.01 /
***Significant at 0.001
In general terms, the results of the ordinal regression models confirm those of the linear regression models. The determination coefficients tend to be similar in both types of model. Furthermore, the independent variables that have a significant effect on the dependent ones tend to be the same in both types of regressions. This could suggest that when the distancing from the assumption of normality is not severe in a large sample-even though the value of the Z test is significant-, the linear regression can function.
Results of the structural analysis
Two structural models (modeling of structural equations) were made using Amos software. Initially, the complete model was programmed considering the seven hypotheses in which the seven latent variables for service quality were associated with the satisfaction latent variable (see Figure 1). The data used was obtained from the application of surveys as observed variables. These observed variables were associated with each of their respective eight latent variables according to the factorial analysis shown in Table 1. Subsequently, the independent latent variables that have a significant impact on satisfaction were identified, as well as the ones that do not. With this, the second structural model, called the final model, was generated.
It is important to mention that when the normality test was performed on all the observed variables used in the structural models, none of them complied with the normality criterion (with the Kolmogorov-Smirnov test). It is assumed that the normality criterion is a required factor in the structural analysis. However, there is evidence that suggests that in the case of large samples (n=100 or greater), as is the case here, the non-normality of the observed variables does not usually affect the precision of the structural model (Jannoo, Auchoybur and Lazim, 2014).
Table 7 shows that except for the chi-square criterion, the structural models satisfactorily comply with all of the adjustment indicators required to consider them acceptable models. Reality adjustment coefficients (NFI, IFI, TLI and CFI) are considered acceptable above 0.90, and good above 0.95 (Bentler and Bonett, 1980). Values of 0.08 or lower in the RMSEA are considered reasonable error approximations (acceptable) and values of 0.05 or lower indicate a good fit; the recommendation is therefore to not accept values greater than 0.1 (Browne and Cudeck, 1993; MacCallum et al., 1996). In the CMIN/DF (chi-square divided by the degrees of freedom) indicator, values lower than 5.0 can be considered acceptable (Wheaton et al., 1977; Marsh and Hocevar, 1985). The RMSEA and CMI/DF are alternative fit measurements that can make the model acceptable when the chi-square is too large, as is the case here (Browne and Cudeck, 1993; MacCallum et al., 1996; Kenny, 2011).
Table 7 Structural models. Adjustment indicators.
| Initial model | Final model | |
| Chi2 | 1340.5*** | 680.6*** |
| CMIN/DF | 2.69 | 3.42 |
| NFI | .90 | .91 |
| IFI | .94 | .94 |
| TLI | .92 | .92 |
| CFI | .94 | .94 |
| RMSEA | .053 | .064 |
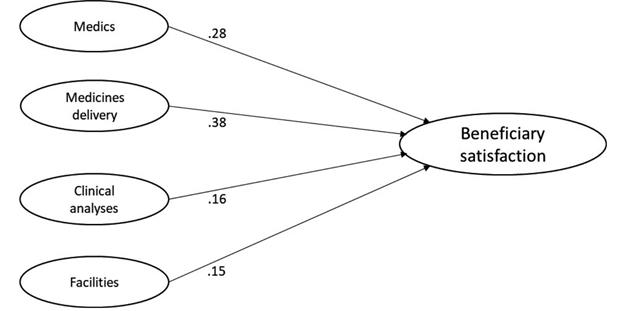
Table 8 shows the results of the regression weights between the latent variables in the structural models. In the first model, all of the independent latent variables (service quality dimensions) were introduced to determine if there is an effect on the satisfaction latent variable. Here, only three independent latent variables showed regression weights statistically significant with respect to satisfaction: care from the physician, delivery of medication, and facilities. The delivery of medication had the highest regression weight.
Table 8 Structural analyses. Standardized regression weights and R2 determination coefficients for the dependent variable (satisfaction)
| Parameters | Initial model | Final model |
| Nurses → Satisfaction | -.003 | - |
| Physicians → Satisfaction | .283*** | .279** |
| Pharmacy staff → Satisfaction | .013 | - |
| Medicaments → Satisfaction | .383*** | .379** |
| Reception/turns → Satisfaction | .034 | - |
| Clinical analyses → Satisfaction | .133 | .157* |
| Facilities → Satisfaction | .130* | .145** |
| R2 for Satisfaction | .50 | .49 |
*Significant at .05, **Significant at .01, ***Significant at .001
R2 = square of the multiple correlation for the dependent variable
Non-significant latent independent variables were progressively eliminated for the final structural model starting with the one with the lowest regression weight. In the end, a latent independent variable that had not been significant in the initial model proved to be significant in the final model. In this manner, a refined (more parsimonious) final model is obtained without non-significant regression weights and with four significant latent independent variables: care from the physician, delivery of medication, clinical analyses, and quality of the facilities. The attribute “delivery of medication” once more is seen to have the highest regression weight. Table 9 shows a comparison between the determination coefficients and the regression coefficients (parameters or estimators) of all the analyses performed.
Table 9 Determination coefficients and regression coefficients
| I feel satisfied | Met the expectations | The service was ideal | Satisfaction (latent) | ||
| Linear regression | R2 | .37 | .37 | .22 | |
| X1 Nurses | .06 | .12 | .07 | ||
| X2 Physicians | .22** | .13* | .12 | ||
| X3 Pharmacy | .17** | .14* | .11 | ||
| X4 Medicaments | .34*** | .31*** | .20** | ||
| X5 Reception/turns | .04 | -.03 | -.16* | ||
| X6 Clinical analyses | .08 | .09 | .12 | ||
| X7 Facilities | .25*** | .27*** | .08 | ||
| Ordinal regression | R2 Cox and Snell | .40 | .39 | .23 | |
| R2 Nagelkerke | .42 | .41 | .24 | ||
| R2 McFadden | .18 | .18 | .09 | ||
| X1 Nurses | .17 | .38* | .20 | ||
| X2 Physicians | .59*** | .28 | .24 | ||
| X3 Pharmacy | .46** | .41** | .27* | ||
| X4 Medicaments | .87*** | .81*** | .45** | ||
| X5 Reception/turns | .17 | -.00 | -.34* | ||
| X6 Clinical analyses | .15 | .21 | .22 | ||
| X7 Facilities | .66*** | .66*** | .12 | ||
| Structural analysis (final model) | R2 | .50 | |||
| X1 Nurses | - | ||||
| X2 Physicians | .28** | ||||
| X3 Pharmacy | - | ||||
| X4 Medicaments | .38** | ||||
| X5 Reception/turns | - | ||||
| X6 Clinical analyses | .16* | ||||
| X7 Facilities | .15** |
*Significant at .05, **Significant at .01, ***Significant at .001
Note: the R2 determination coefficients do not have a significance test associated with them
Discussion and conclusions
Unlike previous studies of the measurement of service quality in health centers, this study departed from an investigation in which a detailed identification of attributes was carried out. Consequently, we worked with 32 highly specific service quality attributes in the primary care clinics sector of state institutions (see Table 2). Previous approaches (Babakus and Mangold, 1992; Murti et al., 2013) have used the SERVQUAL instrument (Parasuraman et al., 1985), adapting its items to the service of health centers. This instrument measures dimensions that are applicable to any type of service, such as tangibles, reliability, response, assurance, and empathy. Although the use of SERVQUAL allows for a greater generalization of the conclusions due to its standard nature, we concluded that it also offers a less comprehensive explanation of the specific phenomenon studied here. Having identified highly specific attributes based on the analysis of the service process to which a beneficiary is subjected makes it possible to offer a more detailed explanation of user-satisfaction generators.
In contrast with this study, previous studies of the measurement of service quality in health centers have focused on private centers. No service quality studies carried out in public clinics were found in the review literature, or at least not in the academic research literature. In this manner, this study could contribute with an initial overview, at this level of publication, of service quality in these types of institutions.
Of the seven hypotheses proposed in this study no evidence was found to support hypotheses H1, H3 and H5, implying that factors such as nursing care, services provided by pharmacy staff, reception service and delivery of turns may carry secondary weight in the determination of the perception of general satisfaction of the beneficiary. However, it should be noted that according to previous studies, although only some attributes are greatly significant in producing high satisfaction, poor performance of the attributes of secondary importance could cause an even greater decrease in satisfaction than when the performance of the main attributes fails (Myers and Alpert, 1968; Anderson and Sullivan, 2000). In other words, these secondary attributes help mitigate the feeling of dissatisfaction when the main attributes fail. Consequently, these attributes of secondary importance should not be discarded, neither from the analyses nor from decision-making in public health centers.
Based on the results obtained, it can be argued that there is evidence to support hypotheses H2, H4, H6 and H7. Therefore, it can be said that service provided by physicians, service in the delivery of medication, service provided in the clinical analyses area, and quality of the facilities are probably the strongest factors in producing feelings of satisfaction in the beneficiary (see Table 9). Among these, service in the delivery of medication apparently plays a more significant role than the others, even above service provided by physicians. The delivery of medication was a facvcdtor carrying greater statistical weight in both the regression models and the structural models (see Table 9). At the beginning of this study, it was thought that service provided by the physicians would carry the most weight. However, trust in medication tends to be the main element providing the user with the feeling that he will be cured. The user’s perception of the institution’s value will thus be mainly concentrated in this element. Nevertheless, the service provided by the physician, though it did not occupy the first place, did rank second. Murti et al. (2013) proposed that quality of delivery of medication be interpreted as an attribute of secondary relevance in health services. However, they did not offer empirical evidence for this. The results of this study appear to provide empirical confirmation of the contrary.
The results of this study reveal two contradictions between the two types of analyses that were performed (regression versus structural). One of the contradictions is that the variable “service provided by the pharmacy staff” was significant in two of the three regression models, but not so in either of the two structural models. The other incongruence is that the variable “service provided by the clinical analysis staff” was not significant in any of the regression models, but was significant in both of the structural models. As the analysis of structural equations is generally a much more robust multivariate statistical method than regression analysis, it was decided to accept the results of the former over those of the latter. In any case, it is interesting to note how the results of the two different statistical methods do not necessarily coincide, thus driving up the number of possible interpretations.
A clear limitation of this study lies in the fact that it was carried out with beneficiaries visiting primary care clinics in Mexico City. In subsequent work, service quality studies could be carried out in clinics of State health institutions in other regions of the country to allow for the examination of geographical differences. Furthermore, studies of this type could be done in secondary and tertiary care centers. Another limitation worth noting is that this study did not include other public health institutions, such as SEDENNA, PEMEX, ‘Seguro Popular’, or ISSEMYM.
This study provides a first approximation of the direct relationship between service quality dimensions and the satisfaction of beneficiaries of the public health sector in Mexico. Future works could thus address the search for moderating variables for this relationship. The identification of moderating variables would make it possible to achieve a broader understanding of the phenomenon of beneficiary satisfaction. These new moderating variables would thus make it possible to increase the explanatory power of the dependent variable (beneficiary satisfaction). Possible hypotheses about variables moderating this relationship could be based on variables related to the involvement construct. In the involvement construct, the variables measured are those related to the beneficiary’s perception of elements such as importance of the service, its symbolic value, and the perceived risk associated with it (Laurent and Kapferer, 1985; Kapferer and Laurent, 1993). In the past, studies have been published (in sectors other than health institutions) of satisfaction and its relationship with other constructs, showing that involvement can have a moderating effect (Sivakumar and Raj, 1997). Thus, the risk a beneficiary perceives when treated in a state clinic can affect his feelings of satisfaction even when the service has been adequately fulfilled. Furthermore, it has been previously postulated that the perceived risk can have a mediating effect on the relationship between the perceived quality the service or product and the perception of value of the user (Snoj et al., 2004). In this manner, future studies could address the relationship between the satisfaction of the beneficiary and his value perception of this type of institution, as contrasted with the possibility of treatment in private clinics.
The variables used in this study focus closely on the care, disposition, and knowledge of the staff of the different areas, since these were the dimensions identified in the qualitative study. However, in future work it may be worth including attributes relating to the procedures themselves, for example, response time to a request or waiting time for assistance, as well as trust in results of laboratory analyses, among other things.
REFERENCES
Akbaba, A. (2006). Measuring Service Quality in the Hotel Industry: A Study in a Business Hotel in Turkey. International Journal of Hospitality Management, 25(2): 170-192. [ Links ]
Amin, M. y Siti, Z. N. (2013). Hospital service quality and its effects on patient satisfaction and behavioral intention. Clinical Governance, 18(3): 238-254. DOI: CGIJ-05-2012-0016 [ Links ]
Andaleeb, S. S. (2001). Service quality perceptions and patient satisfaction: a study of hospitals in a developing country. Social science & medicine, 52(9): 1359-1370. http://dx.doi.org/10.1016/S0277-9536(00)00235-5 [ Links ]
Anderson, E.W. y Sullivan, M. (2000). The impact of critical incidents on customer satisfaction in business-to-business relationships. Journal of Business-to-Business Marketing, 8(1): 25-54. [ Links ]
Asubonteng, P., Mc Cleary, K. J. and Swan, J. E. (1996). SERVQUAL Revisited: A Critical Review of Service Quality. The Journal of Services Marketing, 10(6): 62-81. http://dx.doi.org/10.1108/08876049610148602 [ Links ]
Atta, O. E. G. (2012). The efficacy of applying the quality measure of health service on the external patient satisfaction. Management Review: An International Journal, 7(2): 81-110. [ Links ]
Babakus, E. y Boller, G.W. (1992). An empirical assessment of the SERVQUAL scale. Journal of Business Research, 24(3): 253-268. http://dx.doi.org/10.1016/0148-2963(92)90022-4 [ Links ]
Babakus, E. y Mangold, W. G. (1992). Adapting the SERVQUAL scale to hospital services: an empirical investigation. Health Services Research, 26(6): 767-786. [ Links ]
Bansal, H. S. y Taylor, S. (2015). Investigating the relationship between service quality, satisfaction and switching intentions. Proceedings of the 1997 Academy of Marketing Science (AMS) Annual Conference: 304-313. Springer International Publishing. http://dx.doi.org/10.1007/978-3-319-13141-2_107 [ Links ]
Baumann, C., Burton, S., Elliott, G. y Kehr, H.M. (2007). Prediction of attitude and behavioural intentions in retail banking. International Journal of Bank Marketing, 25(2): 102-116. http://dx.doi.org/10.1108/02652320710728438 [ Links ]
Bentler, P.M. y Bonett, D.G. (1980). Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin, 88(1): 588-606. http://dx.doi.org/10.1037/0033-2909.88.3.588 [ Links ]
Browne, M.W. y Cudeck, R. (1993). Alternative ways of assessing model fit. In Bollen, K.A. & Long, J.S. [Eds.] Testing structural equation models. Newbury Park, CA: Sage: 136-162. [ Links ]
Bruwer, J. (2014). Service quality perception and satisfaction: Buying behaviour prediction in an Australian Festivalscape. International Journal of Tourism Research, 16(1): 76-86. http://dx.doi.org/10.1002/jtr.1901 [ Links ]
Caro, L. y García, J.A. (2007). Cognitive-affective model of consumer satisfaction. An exploratory study within the framework of a sporting event. Journal of Business Research, 60(2): 108-114. [ Links ]
Chi Cui, C., Lewis, B. R., y Park, W. (2003). Service quality measurement in the banking sector in South Korea. The International Journal of Bank Marketing, 21(4/5), 191-201. http://dx.doi.org/10.1108/02652320310479187 [ Links ]
Cronin, J.J. y Taylor, S.A. (1994). SERVPERF versus SERVQUAL; reconciling performance-based. Journal of Marketing, 58(1), 125-131. [ Links ]
Dabholkar, P. A., Thorpe, D. I. y Rentz, J. O. (1996). A measure of service quality for retail stores: scale development y validation. Journal of the Academy of Marketing Science, 24(1): 3-16. http://dx.doi.org/10.1007/BF02893933 [ Links ]
Dagger, T. S., Sweeney, J. C., Johnson, L. W., (2007). A hierarchical model of health service quality: Scale development and investigation of an integrated model. Journal of Service Research, 10(2): 123-142. http://dx.doi.org/10.1177/1094670507309594 [ Links ]
De Oña, R., Machado, J. L. y De Oña, J. (2015). Perceived Service Quality, Customer Satisfaction, and Behavioral Intentions: A Structural Equation Model for the Metro of Seville, Spain. In Transportation Research Board 94th Annual Meeting, No. 15-0897. [ Links ]
Donnelly, M., Wisniewski, M., Dalrymple, J. F. y Curry, A. C. (1995). Measuring service quality in local government: the SERVQUAL approach. International Journal of Public Sector Management, 8(7): 15-20. http://dx.doi.org/10.1108/09513559510103157 [ Links ]
George, D. y Mallery, P. (2003). SPSS for Windows step by step: A simple guide and reference. 11.0 update. 4th ed., Boston: Allyn & Bacon. [ Links ]
Gliem, J. A. y Gliem, R. R. (2003). Calculating, interpreting, and reporting Cronbach’s alpha reliability coefficient for Likert-type scales. Midwest Research-to-Practice Conference in Adult, Continuing, and Community Education, Columbus, OH: 82-88. [ Links ]
Gómez, O., Sesma, S., Becerril, V. M., Knaul, F. M., Arreola, H., y Frenk, J. (2011). Sistema de salud de México. Salud pública de México, 53(1): 220-232. [ Links ]
Gounaris, S. (2005). An alternative measure for assessing perceived quality of software house services. The Service Industries Journal, 25(6): 803-823. DOI: 10.1080/02642060500103373 [ Links ]
Grönroos, C. (1984). A service quality model and its marketing implications. European Journal of Marketing, 18(4): 36-44. DOI: 10.1108/EUM0000000004784 [ Links ]
Halstead, D., Hartman, D. y Schmidt, S. L. (1994). Multisource effects on the satisfaction formation process. Academy of Marketing Science Journal, 22(2): 114-129. http://dx.doi.org/10.1177/0092070394222002 [ Links ]
Haque, A., Sarwar, A. A. M., Yasmin, F., Anwar, A., y Nuruzzaman. (2012). The impact of customer perceived service quality on customer satisfaction for private health centre in malaysia: A structural equation modeling approach. Information Management and Business Review, 4(5): 257-267. [ Links ]
Hill, F. M. y McCrory, M. L. (1997). An attempt to measure service quality at a belfast maternity hospital: Some methodological issues and some results. Total Quality Management, 8(5): 229-242. http://dx.doi.org/10.1080/0954412979488 [ Links ]
Jabnoun, N. y Khalifa, A. (2005). A customized measure of service quality in the UAE. Managing Service Quality, 15(4): 374-388. DOI: 10.1108/09604520510606844 [ Links ]
Jannoo, Z., Yap, B. W., Auchoybur, N., y Lazim, M. A. (2014). The Effect of Nonnormality on CB-SEM and PLS-SEM Path Estimates. International Journal of Mathematical, Computational, Natural and Physical Engineering, 8(2): 285-291. [ Links ]
John, J. (1992). Patient satisfaction: The impact of past experience. Journal of Health Care Marketing, 12(3): 56-64 [ Links ]
Kapferer, J. N. y Laurent, G. (1993). Further evidence on the consumer involvement profile: five antecedents of involvement. Psychology & Marketing, 10(4): 347-355. http://dx.doi.org/10.1002/mar.4220100408 [ Links ]
Kesuma, I. A. W., Hadiwidjojo, D., Wiagustini, N. L. P. y Rohman, F. (2013). Service quality influence on patient loyalty: Customer relationship management as mediation variable (study on private hospital industry in denpasar). International Journal of Business and Commerce, 2(12): 1-14. [ Links ]
Kenny, D. A. (2011). Measuring model fit. Obtenido el 19 de febrero de 2015. Disponible en: Disponible en: http://davidakenny.net/cm/fit.htm [ Links ]
Kerlinger, F. N. (1979). Behavioral research: A conceptual approach. New York: Holt, Rinehart, and Winston. [ Links ]
Knutson, B., Stevens, P., Wullaert, C. y Yokoyama, F. (1991). Lodgserv: a service quality index for the lodging industry. Hospitality Research Journal, 14(3): 277-84. [ Links ]
Kumaraswamy, S. (2012). Service quality in health care centers: An empirical study. International Journal of Business and Social Science, special issue, 3(16): 141-150. [ Links ]
Laurent, G. y Kapferer, J. N. (1985). Measuring consumer involvement profiles. Journal of Marketing, 22(1): 41-53. http://dx.doi.org/10.2307/3151549 [ Links ]
Lis, C. G., Rodeghier, M. y Gupta, D. (2011). The relationship between perceived service quality and patient willingness to recommend at a national oncology hospital network. BMC Health Services Research, 11(1): 1-8. http://dx.doi.org/10.1186/1472-6963-11-46 [ Links ]
MacCallum, R. C., Browne, M. W. y Sugawara, H. M. (1996). Power analysis and determination of sample size for co-variance structure modeling. Psychological methods, 1(2): 130-149. http://dx.doi.org/10.1037/1082-989X.1.2.130 [ Links ]
Marsh, H.W. y Hocevar, D. (1985). Application of confirmatory factor analysis to the study of self-concept: First- and higher-order factor models and their invariance across groups. Psychological Bulletin, 97(1): 562-582. http://dx.doi.org/10.1037/0033-2909.97.3.562 [ Links ]
Murti, A., Deshpande, A. y Srivastava, N. (2013). Service Quality, Customer (Patient) Satisfaction and Behavioural Intention in Health Care Services: Exploring the Indian Perspective. Journal of Health Management, 15(1): 29-44. http://dx.doi.org/10.1177/0972063413486035 [ Links ]
Myers, J.H. y Alpert, M.I. (1968). Determinant Attributes: Meaning and Measurement. Journal of Marketing, 32(4): 13-20. [ Links ]
Olin, S. S., Williams, N., Pollock, M., Armusewicz, K., Kutash, K., Glisson, C. y Hoagwood, K. E. (2014). Quality indicators for family support services and their relationship to organizational social context. Administration and policy in mental health and mental health services research, 41(1): 43-54. http://dx.doi.org/10.1007/s10488-013- 0499-z [ Links ]
Oliver, R. (1980). A Cognitive Model of the Antecedents and Consequences of Satisfaction Decisions. Journal of Marketing Research, 17(4): 460-469. http://dx.doi.org/10.2307/3150499 [ Links ]
Oliver, R. (1999). Whence customer loyalty?. Journal of Marketing, 63(special issue): 33-44. [ Links ]
Orel, F. D. y Kara, A. (2014). Supermarket self-checkout service quality, customer satisfaction, and loyalty: Empirical evidence from an emerging market. Journal of Retailing and Consumer Services, 21(2): 118-129. [ Links ]
Parasuraman, A., Zeithaml, V. A. y Berry, L. L. (1985). A conceptual model of service quality and its implications for future research. Journal of Marketing, 49(1): 41-50. http://dx.doi.org/10.2307/1251430 [ Links ]
Parasuraman, A., Zeithaml, V. A. y Berry, L. L. (1988). SERVQUAL: a multiple item scale for measuring consumer perceptions of service quality. Journal of Retailing, 64(1): 12-40. [ Links ]
Ryu, K., y Han, H. (2010). Influence of the quality of food, service, and physical environment on customer satisfaction and behavioral intention in quick-casual restaurants: Moderating role of perceived price. Journal of Hospitality & Tourism Research, 34(2/3): 310-329. http://dx.doi.org/10.1177/1096348009350624 [ Links ]
Ryu, K., Lee, H. y Kim, W. (2012). The influence of the quality of the physical environment, food, and service on restaurant image, customer perceived value, customer satisfaction, and behavioral intentions. International Journal of Contemporary Hospitality Management, 24(2): 200-223. http://dx.doi.org/10.1108/09596111211206141 [ Links ]
Scott, D. y Shieff, D. (1993). Service quality components and group criteria in local government. International Journal of Service Industry Management, 4(4): 42-53. http://dx.doi.org/10.1108/09564239310044280 [ Links ]
Sivakumar, K. y Raj, S. P. (1997). Quality tier competition: How price change influences brand choice and category choice. The Journal of Marketing, 61(3): 71-84. http://dx.doi.org/10.2307/1251790 [ Links ]
Snoj, B., Korda, A. P. y Mumel, D. (2004). The relationships among perceived quality, perceived risk and perceived product value. Journal of Product & Brand Management, 13(3): 156-167. http://dx.doi.org/10.1108/10610420410538050 [ Links ]
Spreng, R. y R. Mackoy (1996). An empirical examination of a model of perceived service quality and satisfaction. Journal of Retailing, 72(2): 201-214. http://dx.doi.org/10.1016/S0022-4359(96)90014-7 [ Links ]
Stevens, P., Knutson, B. y Patton, M. (1995). Dineserv: a tool for measuring service quality in restaurant. CQ Restaurant Administration Quarterly, 36(2): 56-60. http://dx.doi.org/10.1177/001088049503600226 [ Links ]
Taylor, S. A. y Baker, T. L. (1994). An assessment of the relationship between service quality and customer satisfaction in the formation of consumers’ purchase intentions. Journal of retailing, 70(2): 163-178. http://dx.doi.org/10.1016/0022-4359(94)90013-2 [ Links ]
Taylor, S. A. y Cronin Jr, J. J. (1994). Modeling patient satisfaction and service quality. Journal of Health Care Marketing, 14(1): 34-44. [ Links ]
Tsoukatos, E. y G. Rand (2007). Cultural influences on service quality and customer satisfaction: evidence from Greek insurance. Managing Service Quality, 17(4): 467-485. http://dx.doi.org/10.1108/09604520710760571 [ Links ]
Westbrook, R. (1980). Intrapersonal affective influences on consumer satisfaction with products. Journal of Consumer Research, 7(1): 49-54. http://dx.doi.org/10.1086/208792 [ Links ]
Wheaton, B., Muthén, B., Alwin, D.F. y Summers, G.F. (1977). Assessing reliability and stability in panel models. In Heise, D.R. [Ed.] Sociological methodology. San Francisco: Jossey-Bass: 84-136. [ Links ]
Woodside, A.G., Frey, L.L. y Daly, R.T. (1989). Linking service quality, customer satisfaction. Journal of Health Care Marketing, December: 5-17. [ Links ]
Van Dyke, T. P., Kappelman, L. A. y Prybutok, V. R. (1997). Measuring information systems service quality: concerns on the use of the SERVQUAL questionnaire. MIS Quarterly, 21(2): 195-208. http://dx.doi.org/10.2307/249419 [ Links ]
Vignolo, J., Vacarezza, M., Álvarez, C. y Sosa, A. (2011). Niveles de atención, de prevención y atención primaria de la salud. Archivos de Medicina Interna, 33(1): 7-11. [ Links ]
Zeithaml, V. A., Berry, L.L. y Parasuraman, A. (1996). The Behavioral Consequences of Service Quality. Journal of Marketing, 60(2): 31-46. http://dx.doi.org/10.2307/1251929 [ Links ]
Received: May 06, 2015; Accepted: July 13, 2015
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
