











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Before the COVID-19 pandemic, in Mexico and Colombia, between 9 to 10% of the general population suffered from an affective disorder at some point in their lives (Berenzon, Lara, Robles, & Medina-Mora, 2013; Ministerio de Salud y Protección Social, 2017). In Mexico, it was shown that around 14% of the population presented with depression symptoms, affecting more women (Valencia, 2022), and 31% had some level of anxiety (INEGI, 2021). On the other hand, in Colombia, about 80% of the general population claimed to present with one to three symptoms of depression and 53% suffer from anxiety (Ministerio de Salud y Protección Social, 2017). Interestingly, as shown in Mexico, most mental disorders appear in individuals that are young adults, before the age of 21 (Berenzon et al., 2013; Martínez-Martínez, Muñoz-Zurita, Rojas-Valderrama, & Sánchez-Hernández, 2016), which is similar to Colombia, in which most present in women aged 18-44 years old, some of which attend university. This would suggest that university students are more prevalent to present with a mental disorder.
During university life, students are subjected to various stress-inducing factors that can threaten mental health, such as academic demands, excessive workload, personal life events, and the learning environment (Fares, Al Tabosh, Saadeddin, El Mouhayyar, & Aridi, 2016).
Cheung and collaborators demonstrated that age, gender, study load, and academic performance were factors associated with mental health conditions, such as depression and anxiety (Cheung, Tam, Tsang, Zhang, & Lit, 2020). Moreover, many studies have shown that medical students at the start of their careers presented a greater burden of psychiatric morbidity when compared to students of other disciplines as well as the general population (Fares et al., 2016; Suárez & Fernández, 2020). Indeed, in Mexico and Colombia, medical students were shown to have significant levels of depression (25-50%), anxiety (50-60%), and stress (60-70%; Granados Cosme et al., 2020; Saldaña Orozco, De Loera Soto, & Madrigal Torres, 2017; Pabón, Espinosa, Correa, Ríos, & Gutiérrez, 2018; Suárez & Fernández, 2020). Recently, increased time spent in front of electronic devices and social networks, which can lead to less social interaction, can augment depression and unhappiness among younger generations (Berryman, Ferguson, & Negy, 2018).
On January 30, 2020, the World Health Organization declared COVID-19 as a pandemic (World Health Organization, 2020). Since then, numerous outlets have suggested that the measures taken during this period could affect mental health (Brooks et al., 2020). There was a worldwide increase in the use of social media during the quarantine (Tsao et al., 2021), which is postulated to affect mental health (Karim, Oyewande, Abdalla, Ehsanullah, & Khan, 2020). Previous studies have highlighted the harmful influence of quarantines linked to viral epidemics/pandemics on mental health. For example, in Australia, approximately 34% of horse owners quarantined for several weeks because of an equine influenza outbreak, reported higher psychological distress, compared with around 12% in the general population (Taylor, Agho, Stevens, & Raphael, 2008). Moreover, Brooks and collaborators reported a positive association between the length of the quarantine and post-traumatic stress disorder symptoms, avoidance behaviors, and anger. Furthermore, they pointed out that among hospital staff, being quarantined is a predictor of acute stress disorder and depressive symptoms (Brooks et al., 2020). This is similar to medical students, in which students from a private medical university during the SARS outbreak in 2003 demonstrated that they presented with elevated degrees of anxiety (Loh, Ali, Ang, & Chelliah, 2006). Additionally, medical students presented with higher levels of anxiety during the MERS (Al-Rabiaah et al., 2020) and H1N1 (Swine) flu pandemic (Wheaton, Abramowitz, Berman, Fabricant, & Olatunji, 2012). Therefore, it is expected that the rate of these disorders should increase with the COVID-19 pandemic.
With the worsening of mental health associated with the medical school format, coupled with the cessation of fundamental face-to-face activities and social distancing due to the COVID-19 pandemic, it was postulated that levels of depression, anxiety, and stress could be augmented among medical students. The objective of this study was to determine levels of depression, anxiety, and stress in medical students from Mexico and Colombia during the COVID-19 pandemic. Furthermore, levels of depression, anxiety, and stress were compared by gender, educational level, and country (Mexico versus Colombia).
METHOD
Subjects / description of the sample
The sample population was recruited by using a cluster, volunteer sampling method. The project was first conceived at BUAP, in which other institutions were available via the DELFIN program. The DELFIN program allows students within Mexico as well as Colombia, Costa Rica, Nicaragua, and Peru to participate in research. The project was published within the program, in which potential students contacted the corresponding author. After a virtual meeting, the students were explained to contact only students within their medical school, in which the students were asked to post a general invitation to participate on the university’s message board, by e-mail, and by snowball sampling contact. They were to explain that the participant anonymity would be maintained, only known to the corresponding author and selected personnel.
To be included in the study, the participants had to be current, active students, between the ages of 18 to 25 years old, belonging to a medical school, and who were taking their course material in a virtual format during the pandemic. Those exclude were students who did not belong to the medical school (full-time) or those who were taking classes as well as practices in a face-to-face or semi-face-to-face format, taking or started taking any medication that could alter moods, had a traumatic family or personal event that could affect the results other than due to the pandemic, partially or early terminated questionnaires, or a previous diagnosis of a psychopathological disorder.
Places
The participant pool consisted of medical students from different universities in Mexico (Puebla, Chihuahua, State of Mexico, Veracruz, Guerrero, Morelos, Nuevo Leon, Tlaxcala, Oaxaca, Durango, Coahuila, Jalisco, Baja California, Tamaulipas, Sinaloa) and Cartagena, Colombia.
Measurements
The online instrument collected demographic and specific data. The demographic data collected were gender (biological sex), age, country, residency (urban or rural), mask type and usage, school year, and type of work. Problems with work, school, and other (serious) problems, the participants were asked to identify. Lastly, concepts about academic achievement, physical activity, and internet access were also collected.
Developed by Lovibond & Lovibond, the Depression Anxiety Stress Scales-21 (DASS-21) questionnaire proved to be a reliable and consistent instrument that was validated for Spanish-speaking populations (Ruiz, Martín, Falcón, & González, 2017; Yohannes, Dryden, & Hanania, 2019). This instrument, comparable with the Likert technique, measured the states of depression, anxiety, and stress using three different scales containing seven items each with four possible answers: 0. did not apply to me at all, 1. applied to me to some degree or some of the time, 2. applied to me to a considerable degree or a good part of the time, and 3. applied to me very much or most of the time. Items corresponding to depression were questions 3, 5, 10, 13, 16, 17, and 21, for anxiety were questions 2, 4, 7, 9, 15, 19, and 20, and for stress were questions 1, 6, 8, 11, 12, 14, and 18. For specific wording of the DASS-21 questionnaire, see Supplement Table 1.
Procedure
This study carried out between July 2020 and January 2022 using an online questionnaire through health-survey platform (https://health-survey-2021.vercel.app/). The online instrument that used to evaluate the participants divided into five different sections that corresponded to 1. invitation to participate, 2. informed consent (identification data and signed photographic consent), 3. general/demographic data, 4. learning difficulties, and 5. the DASS-21 questionnaire. The data and information obtained during this study handled according to Article 14.1 of the Federal Law on Protection of Personal Data. Lastly, study conducted by the CHERRIES guidelines (Eysenbach, 2004; Supplement Table 2).
Statistical analysis
All analyses were carried out with the Statistical Package for the Social Sciences software (SPSS v26.0, Chicago, IL USA) or with R software (Ripley, 2001). The normality of the data assessed by the Shapiro–Wilk test. Differences between groups were determined using the chi-squared test for categorical data whereas, depending on the normality of the data, either Student’s T-test or the Mann U test used for continuous data. Due to zero values in the referent group, Firth Logistic Regression was used to determine the odds ratio (OR) and 95% confidence interval (95% CI), to evaluate the level of risk for depression, anxiety, and stress when stratified by gender and school year (basic: school years 1-3 and advanced: school years 4-6). Firth Logistic Regression was performed with R using the logit package. p-values < .05 (two-tailed) were considered statistically significant.
The sample size calculated using: n = (NZ2p [1-p]) / (e2 [N-1] + Z2p [1-p]), where n = sample size, N = population of medical students in participating countries, p = probability of occurrence, Z = confidence level critical value and e = maximum estimate error. Note, the number of medical students/graduates is similar for Mexico (11.6 per 100,000 inhabitants) and (11.7 per 100,000 inhabitants) Colombia (OECD, 2022). The population of students enrolled in medical school in Mexico and Colombia is around 15,000 and 6,000, respectively, totaling 21,000. The prevalence rates for depression, anxiety, and stress in medical students can range between 50-60%; therefore, a probability of .5 was used for the largest sample size. A sample size of at least 378 was determined using the following assumptions: N = 21,000, 95% confidence interval (Z = 1.96), e = 5%, and p = .5.
Ethical considerations
All who agreed to participate gave signed photographic consent, by the Declaration of Helsinki. This study was approved by the Ethics Committee of the Vice-Rector's Office for Research and Postgraduate Studies at the Benemérita Universidad Autónoma de Puebla (approval number: Registry number 910, book 2, sheet 156 [SIEP/C.I/136/2022]).
RESULTS
Selection of participants
Of the 566 participants that agreed to participate and completed the survey, 140 were excluded for being < 18 or > 25 years old or did not have photographic-signed consent. Which resulted in 426 students from Mexico and Colombia being assessed (Supplement Table 3). When stratified by school year, 69.5% were in their basic years and 30.5% were in their advanced years, which resulted in a significant difference in the ages of the two groups. However, when stratified by gender, 63.8% were female and no difference in age was observed.
Depression, anxiety, and stress among Mexican and Colombian medical students
The average scores for depression, anxiety, and stress using the DASS-21 questionnaire for Mexicans and Colombians were 6.7 ± 1.2, 8.8 ± 1.2, and 5.6 ± 1.2, respectively (Figure 1A). For depression, when the scores were categorized, most of the students were normal with few defined as having significant depression (26.6%, Figure 1B). For anxiety, when the scores were categorized, most of the students presented with some level of anxiety (55.9%, Figure 1C). Interestingly, for stress, a majority of the students were normal (95.5%, Figure 1D).
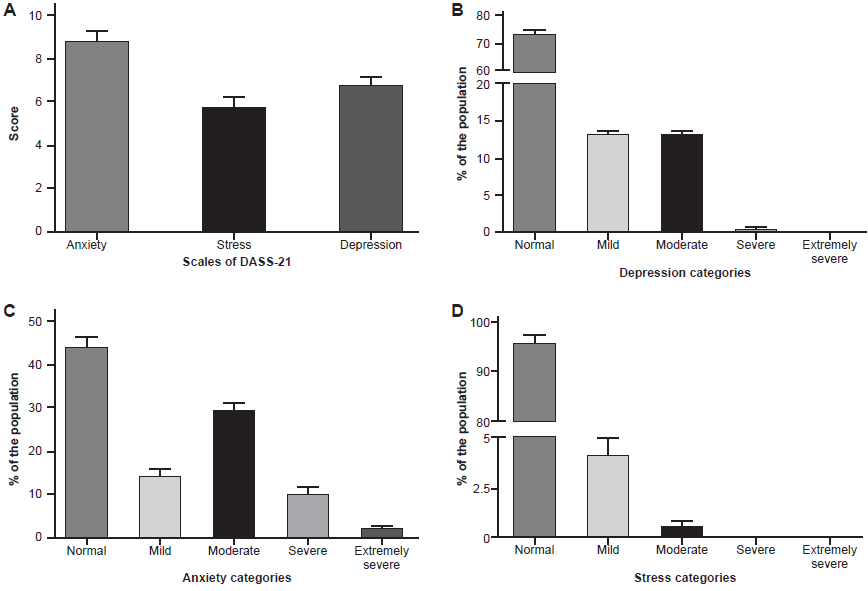
Figure 1 The prevalence and severity of depression, anxiety, and stress among Mexican and Colombian medical students during the COVID-19 Pandemic. A) Overall scores for depression (right bar), anxiety (left bar), and stress (center bar). B) Depression, C) anxiety, and D) stress were categorized as normal, mild, moderate, severe and extremely severe. The bar height and lines correspond to the average score and 95% confidence interval.
Using the data for Mexicans and Colombia together, when stratified by gender, females had significantly higher overall scores for depression (.24-fold increase), anxiety (.25-fold increase), and stress (.40-fold increase) than males (p < .01, Table 1). Moreover, females presented with higher severity for anxiety than males (63.3% versus 42.9%, respectively, Table 1), an observation not seen with depression or stress. The frequency of the responses to the DASS-21 questionnaire, categorized by school year or gender is shown in Supplement Table 1.
Table 1 The level of depression, anxiety, and stress for medical students, as determined by the DASS-21 questionnaire, stratified by gender and education level
| Gender a | Year c | |||||||
|---|---|---|---|---|---|---|---|---|
| Rank | Male | Female | p-value b | Advance | Basic | p-value b | ||
| Overall score | 5.8 ± 5.2 | 7.2 ± 5.3 | .007* | 6.0 ± 5.0 | 7.0 ± 5.4 | .084 | ||
| Depression | Normal | 77.9 (70.8-83.8) | 71.0 (66.2-76.1) | .286 | 80.0 (72.3-86.9) | 70.6 (65.5-76.0) | .204 | |
| Mild | 12.3 (7.1-18.2) | 13.6 (9.6-17.6) | 10.0 (4.6-15.4) | 14.5 (10.5-18.2) | ||||
| Moderate | 9.7 (5.2-14.3) | 14.7 (10.7-18.8) | 10.0 (5.4-15.4) | 14.2 (10.1-18.6) | ||||
| Severe | 0 (N/A) | .7 (0-1.8) | 0 (N/A) | .7 (0-1.7) | ||||
| Extremely severe | 0 (N/A) | 0 (N/A) | 0 (N/A) | 0 (N/A) | ||||
| Overall score | 7.6 ± 4.9 | 9.5 ± 4.4 | < .001* | 7.5 ± 4.2 | 9.4 ± 4.8 | < .001* | ||
| Anxiety | Normal | 57.1 (49.4-64.9) | 36.7 (31.3-42.3) | .002* | 53.1 (44.6-60.8) | 40.2 (34.8-45.6) | .012* | |
| Mild | 12.3 (7.1-18.2) | 15.4 (11.4-20.2) | 16.9 (10.0-23.8) | 13.2 (9.5-17.2) | ||||
| Moderate | 21.4 (15.6-28.6) | 33.8 (28.3-39.0) | 23.8 (16.9-31.5) | 31.8 (26.4-36.8) | ||||
| Severe | 7.1 (3.2-11.0) | 12.1 (8.5-15.8) | 6.2 (2.3-10.0) | 12.2 (8.8-16.2) | ||||
| Extremely severe | 1.9 (0-4.5) | 1.8 (.4-3.7) | 0 (N/A) | 2.7 (1.0-4.7) | ||||
| Overall score | 4.5 ± 4.1 | 6.3 ± 4.5 | < .001* | 4.5 ± 3.8 | 6.2 ± 4.6 | < .001* | ||
| Stress | Normal | 96.8 (93.5-99.4) | 94.9 (92.3-97.4) | .471 | 97.7 (94.6-100.0) | 94.6 (91.9-97.0) | .317 | |
| Mild | 3.2 (.6-6.5) | 4.4 (2.2-7.0) | 2.3 (0-5.4) | 4.7 (2.7-7.1) | ||||
| Moderate | 0 (N/A) | .7 (0-1.8) | 0 (N/A) | .7 (0-1.7) | ||||
| Severe | 0 (N/A) | 0 (N/A) | 0 (N/A) | 0 (N/A) | ||||
| Extremely severe | 0 (N/A) | 0 (N/A) | 0 (N/A) | 0 (N/A) | ||||
Notes: Values are either frequency (% ± 95% confidence interval) or mean ± standard deviation.
aGender was based on the participant’s biological sex.
bp-values were calculated using either the chi-squared test for categorical data (normal, mild, moderate, severe, or extremely severe) or either Student’s T test or Mann U test for overall score.
cBased participants year of education (semester), they were either classified as basic (school years 1 to 3) or advanced (school years 4 to 6).
*Indicates a significant difference (p < .05, two-tailed) between the two genders.
It has been shown that as medical student progress through their education, depression, anxiety, and stress increase; therefore, Mexican and Colombians medical students were stratified by school year (Table 1). Depression’s overall score as well as its categories were not affected by the student’s school year. However, for anxiety and stress, there was a difference between the overall score for basic and advanced years, in which basic years were associated with higher scores (.25- and .38-fold increase, respectively). When stratified into normal, mild, moderate, and severe, there was no statistical difference in the distribution of stress; however, for anxiety, there was an increase in the prevalence of the moderate form for basic years, with a significant decrease in the mild and severe forms for a student in their advance years.
The risk associated with gender and school year for developing depression, anxiety, and stress was evaluated (Table 2). For depression, using males in advanced years as the referent, only females in their basic years demonstrated a significant increase in risk. Therefore, being a male doesn’t affect developing depression, as well as being a female in her advanced years. However, being a female starting medical school (1-3 years) did show an increased risk for depression, even when compared to male students in their basic years (a .38-fold increase). For Anxiety, when males in their advanced years were compared to males in their basic years, a significant increase in the risk of almost 3-fold was observed. On the other hand, when females in their advanced years were compared to females in their basic years, a .21-fold increase was observed. Stress did not show any significant difference between any of the comparisons. Lastly, due to the different COVID-19 mandates between Mexico and Colombia, the group was stratified by country (Table 3). For Mexico, there was an increased risk for depression and anxiety but not for stress, when compared to Colombia as the referent.
Table 2 The risk of developing depression, anxiety, or stress based on gender and school year
| Gender a | Year b | Negative c | Positive c | Odds ratio d | 95% CI d | p-value d | |
|---|---|---|---|---|---|---|---|
| Depression | Male | Advance | 42 | 8 | 1.00 | Referent | - |
| Basic | 78 | 26 | 1.69 | .74-4.19 | .219 | ||
| Female | Advance | 62 | 18 | 1.48 | .62-3.80 | .387 | |
| Basic | 131 | 61 | 2.34 | 1.10-5.51 | .026* | ||
| Anxiety | Male | Advance | 37 | 13 | 1.00 | Referent | - |
| Basic | 51 | 53 | 2.89 | 1.42-6.15 | .003* | ||
| Female | Advance | 32 | 48 | 4.15 | 1.97-9.14 | < .001* | |
| Basic | 68 | 124 | 5.05 | 2.59-10.36 | < .001* | ||
| Stress | Male | Advance | 50 | 0 | 1.00 | Referent | - |
| Basic | 99 | 5 | 5.58 | .61-738.33 | .148 | ||
| Female | Advance | 77 | 3 | 4.56 | .43-618.26 | .238 | |
| Basic | 181 | 11 | 6.40 | .81-826.53 | .088 |
Notes
aBased participants year of education (semester), they were either classified as basic (school years 1 to 3) or advanced (school years 4 to 6).
bGender was based on the participant’s biological sex.
cPositive cases were participants identified as either mild, moderate, severe, or extremely severe, whereas negative cases were participants identified as normal.
dOdds ratios and 95% confidence intervals were calculated using R logitf package (Firth Logistic regression).
*Indicates a significant result (p < .05, two-tailed).
Table 3 The risk of developing depression, anxiety, or stress based on the medical students’ location (Mexico versus Colombia)
| Country | Negative a | Positive a | Odds ratio b | 95% CI b | p-value b |
|---|---|---|---|---|---|
| Depression | |||||
| Colombia | 64 | 12 | 1.00 | Referent | - |
| Mexico | 249 | 101 | 2.16 | 1.12-4.18 | .022* |
| Anxiety | |||||
| Colombia | 45 | 31 | 1.00 | Referent | - |
| Mexico | 143 | 207 | 1.10 | 1.27-3.48 | .004* |
| Stress | |||||
| Colombia | 74 | 2 | 1.00 | Referent | - |
| Mexico | 333 | 17 | 1.89 | .43-8.35 | .402 |
Notes:
aPositive cases were participants identified as either mild, moderate, severe, or extremely severe, whereas negative cases were participants identified as normal.
bOdds ratios and 95% confidence intervals were calculated using R logitf package (Firth Logistic regression)
*Indicates a significant result (p < .05, two-tailed).
DISCUSSION AND CONCLUSION
Using the DASS-21 questionnaire, significant levels of depression (27%), anxiety (56%), and stress (5%) were determined for Mexican and Colombian medical students. When compared by gender, level of education, and country, females showed significantly higher scores for anxiety and stress than males that are in their basic years of medical training. Moreover, Mexico had an increased risk for depression and anxiety, when compared to Colombia.
Anxiety was the most prevalent psychopathological condition, regardless of sociodemographic variables, such as gender, age, and school year, which suggests that the confinement and lifestyle restrictions caused by the pandemic generated anxiety among this subset of students. For the general population, Shigemura and collaborators demonstrated that overwhelming and sensational news headlines as well as imagery add to anxiety (Shigemura, Ursano, Morganstein, Kurosawa, & Benedek, 2020). It is postulated that rumors and hyped information filled these individuals in the absence of information. Additionally, Rubin and Wessely (2020) proposed that during disease outbreaks, community anxiety can rise following the first death, increased media reporting, and an escalating number of new cases (Rubin & Wessely, 2020). In Mexico and Colombia, these characteristics were met, fostering anxiety in our group. Moreover, mass quarantines are likely to raise anxiety substantially (Rubin & Wessely, 2020). Medical students in Saudi Arabia reported higher levels of anxiety during the MERS pandemic (Al-Rabiaah et al., 2020). Moreover, medical students in South Carolina also reported higher levels of anxiety during the H1N1 flu (Wheaton et al., 2012). Thus, it is reasonable to presume that the effects due to the COVID-19 pandemic are the causes of the increased prevalence and risk of anxiety for these medical students, and a baseline, which is provided here, is necessary to evaluate an effect on their future performance.
Before the COVID-19 pandemic, one of the most recent studies found that the prevalence of depression was 32.7% among medical students in China, whereas the prevalence of anxiety was 27.2% (Mao et al., 2019). As reported for medical students in India, the prevalence of moderate to severe depression was 14.9%, whereas stress was exceedingly high at 83.7% for moderate to very-high levels (Kumar, Kattimani, Sarkar, & Kar, 2017). Here, our values were similar, in which depression was 13.3%; however, severe stress was only 4.5% for the group. This does suggest that the pandemic impacted the levels of depression and stress for our group and other medical students around the world.
Typically, medical students reported that the causes of stress were difficulty in understanding the content, feeling incompetent in managing the patient, feeling compelled to participate in the scenario, and competition with team members to name a few (Pai, Ram, Madan, Soe, & Barua, 2014). Therefore, it is postulated that any effect the pandemic has had on these medical students will be minimal for their future performance when only considering stress and depression; however, the lack of these stressors could put these medical students at a disadvantage due to inexperience and failure to resolve these stressors. As indicated by Pai and collaborates, repeated training sessions reduce stress, which these students did not receive (Pai et al., 2014).
It was shown that depression and anxiety are more prevalent in females. In a systematic review of medical students from the USA and Canada, they indicated higher rates of psychosocial distress among female students (Dyrbye, Thomas, & Shanafelt, 2006). However, our results show a higher female prevalence for anxiety only in firsts years students, with a significant decrease in advanced years of medical training. This suggests that levels of anxiety decline as the students adapt to the medical school program. In support of this, Brenneisen and collaborators demonstrated that as female students progress through medical school, their Beck Depression Inventory and State-Trait Anxiety Inventory scores decreased (Brenneisen Mayer et al., 2016). They also confirm our results in which female medical students were more prone to have depression and anxiety symptoms than males.
COVID-19 has exacerbated educational inequalities across countries. Numerous studies published during the pandemic have demonstrated a country-dependent difference in levels of depression, anxiety, and stress (Bibi, Lin, Zhang, & Margraf, 2020). In our study, the DASS-21 scores for Colombian and Mexican students were found to be different, where a higher risk of suffering from depression and anxiety was associated with Mexicans. These inequalities in most cases are multifactorial and are related to the school’s operating standards, socioeconomics, geographic conditions, and other variables that make it difficult to guarantee equitable coverage for the entire territory and social strata. In Colombia, the COVID-19 restrictions (Ministerio de Salud y Protección Social, 2020) were more severe than in Mexico (Diario Oficial de la Federación, 2020). These different factors have a direct impact on how the two countries went through the pandemic. One interesting occurrence was the country that had more sanitary restrictions had lowers levels of these psychopathologies. This can be related to the concept that people care about not being infected and all the government mandatories gave them a feeling of security.
This study has a few limitations. First, the response rate was lower for advanced-year medical students and may limit the interpretation of the findings. Second, the sample selected for this study was specifically medical students. The results obtained may not apply to students outside of this designation. Third, this study did not examine the psychological impact that COVID-19 has had on all Mexican and Colombian students. Fourth, the regional differences between Mexico and Colombia, as well as the regional differences within each country, were not taken into consideration. Even though the format for most medical programs, such as the number of classes, the order in which the classes are taken, the literature used, and the methods of teaching, are similar between each school, the number of medical schools in Mexico (113 institutions) and Colombia (61 institutions), the potential of socioeconomic and demographical factors could influence the results shown here. For future studies, a more complex sampling methodology should be implemented to be able to assess these factors. Moreover, the type of school, private or public, could affect the association. Here, all schools that participated were public institutions. Fifth, potential sample/selection bias could be present. For the overall sample, the sample size was sufficient but the reason for participating in the study was unknown. Moreover, the representativeness of the sample was not qualified. Within Mexico as well as Colombia and between each country, the demographic and socioeconomic factors do range. However, during the period in which the study occurred, implementation of COVID-19 restrictions did vary between each state in Mexico and Colombia. Nevertheless, the effects of the COVID-19 pandemic restrictions between each state were similar. Lastly, the previous assessments for depression, anxiety, and stress were not available. Here, it was observed that the rate of depression, anxiety, and stress were similar to pre-pandemic levels. However, the influence of the pandemic on depression, anxiety, and stress could not be deduced, as for the difficulty of predicting a pandemic and getting the project’s approval. Nevertheless, future studies are being designed in which students are to be followed during their medical school, independent of the events that take place.
A high prevalence of anxiety and depression was observed in medical students from Mexico and Colombia. Females and students early in their medical training were factors associated with an increase in depression and anxiety. This study serves as a baseline analysis for future assessments of these students, which can determine how the COVID-19 pandemic has affected their future performance as clinicians. Lastly, Mexicans were more at-risk to suffer from higher levels of depression and anxiety than Colombians.

