











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Transsexual, trans, and transgender are often used interchangeably (Aguirre-Sánchez-Beato, 2018). Exact definitions of these terms vary and have changed over time (American Psychological Association [APA], 2011); for the sake of clarity, we will define these terms. Transgender is an umbrella term for people whose gender identity, expression, and/ or behavior is different from those typically associated with their assigned sex at birth (APA, 2011). Many identities fall under the transgender umbrella, including but not limited to transsexual people, androgynous people, and two-spirit people. In contrast, the term cisgender refers to people whose sex assigned at birth fits their gender identity and expression (Aguirre-Sánchez-Beato, 2018). The term transsexual woman is contained under the umbrella transgender term and it specifically refers to people who identify themselves as women, even though their assigned sex at birth is male (APA, 2011) or being aware that they are anatomically males (Moreno-Pérez, Esteva De Antonio, & Grupo de Identidad y Diferenciación Sexual de la SEEN [GIDSEEN], 2012). The term transsexual woman is sometimes restricted to describe individuals who seek to change or have changed their sexual characteristics through femininizing medical interventions (World Professional Association for Transgender Health [WPATH], 2012). Some consider the term transsexual to be offensive and stigmatizing, and it is also associated with pathologization (Aguirre-Sánchez-Beato, 2018). Therefore, the current trend is to use the term transgender instead (T’Sjoen, Arcelus, Gooren, Klink, & Tangpricha, 2019). “Trans” is frequently used as a shorthand for transgender or transsexual (Manning, Baruth, & Lee, 2017). In this article, we use the conceptual definition of “trans woman” (TW) to refer to people who are assumed to be female, even though their assigned sex at birth is male (Ramírez-Rentería, López-Juárez, Cruz, Román, & Fong, 2018). This term encompasses women who have undergone gender-affirming procedures (GAPs) and those who have not, but in either case these people play a female role. Gender dysphoria refers to the stress caused by gender incongruence and emphasizes that the clinical problem is the dysphoria suffered by the transgender person, not their identity per se (Ramírez-Rentería et al., 2018; Wiepjes et al., 2018).
Some TW search for congruence between their body and gender identity, undertake a gender transition, have a stronger need for gender affirmation than their cisgender counterparts, suffer gender dysphoria, and yearn for passing. For TW, passing refers to being identified by others as a woman (Gyamerah et al., 2021). Transition usually starts at the social level, with changes in role expression and identification with a name and pronouns that are congruent with their identity. Some TW need hormone replacement therapy (HRT) and/or GAPs to mitigate gender dysphoria (Williams, Patete, & Thaller, 2019). GAPs include but are not limited to facial feminization surgery, augmentation mammoplasty, genital reconstruction, and voice feminization surgery. Previously, TW were required to live full-time as their self-affirmed gender before accessing HRT, GAPs, or changing their legal status. The so-called “real life test” is no longer required (Unger, 2016). Gender transition is a very personal process and is challenging for most TW. The importance of adequate psychological support before, during, and after transition by empathetic mental health professionals cannot be overstated (Deutsch, & Center of Excellence for Transgender Health, 2016).
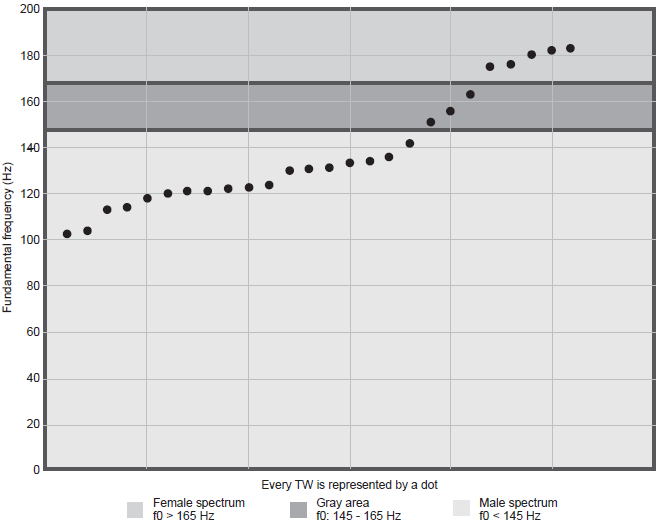
Voice is a gender marker. Voices considered feminine differ from those considered masculine in pitch, intensity, voice quality, resonance, articulation, word selection, and prosody, among others (Van Borsel, Janssens, & De Bodt, 2009; Nešić, Čičević, Nešić, Kostić, & Ćirić, 2013). Mean fundamental frequency (f0) is an acoustic property associated with the perceptual notion of the pitch and is considered the most relevant gender marker. Voices identified as masculine have an f0 < 145 hz, while those identified as feminine have an f0 > 165 Hz. Voices with an f0 within the range from 145-165 Hz fall in a gray area, where gender recognition depends on other factors (Meister, Kühn, Shehata-Dieler, Hagen, & Kleinsasser, 2017).
The prevalence of depression (Hoffman, 2014) and anxiety disorder (Millet, Longworth, & Arcelus, 2017) in trans people is higher than in the cis population and has been linked to substance abuse, high-risk sexual behaviors, and suicide. Gender dysphoria added to frequent experiences of stigma and discrimination may partly explain the disproportionately high rates of anxiety and depression (Owen-Smith et al., 2018). Failure to conceal a masculine voice may lead to embarrassment and social isolation with a detrimental effect on the quality of life (QoL; Song & Jiang, 2017). In contrast, feelings of “passing” have been associated with a higher quality of life and self-esteem (Owen-Smith et al., 2018). Moreover, a significant association between symptoms of anxiety and depression and self-reported voice difficulties using the Trans Woman Voice Questionnaire (TWVQ) has been described. (Novais Valente & Mesquita de Medeiros, 2020). HRT in transgender individuals reduces the risk of depressive disorders (Witcomb et al., 2018) and anxiety (Bouman et al., 2017). GAPs are associated with higher body-gender congruence and lower rates of depression and anxiety (Boza & Perry, 2014; Dhejne, Van Vlerken, Heylens, & Arcelus, 2016); yet, these studies do not specifically discuss voice-gender congruence nor the effect of voice femininization.
HRT does not play a role in voice feminization (Schwarz et al., 2017). Alternatives for voice feminization include speech therapy and surgical procedures. Speech therapy is focused on adapting the voice and communication patterns to reflect the desired gender identity by modifying the pitch, intonation, resonance, breathiness, word selection, and other parameters of verbal and non-verbal communication (Hancock & Helenius, 2012). Voice feminization surgery modifies the anatomy of the vocal cords to increase f0. The most widespread surgical technique is endoscopic shortening glottoplasty (Song & Jiang, 2017). An increase in f0 is the main outcome in literature discussing results of voice feminization (Nolan et al., 2019). Despite this focus on f0, the fact remains that some TW are not perceived as female despite having an f0 > 165 Hz, and the correlation between f0 scores with the degree of happiness in TW is weaker than expected (Dacakis, Oates, & Douglas, 2017; Meister et al., 2017). In 2019, a systematic review exploring the efficacy of voice feminization procedures found that surgery and therapy are effective in rising f0 and the patient’s satisfaction. However, it also recognizes that a knowledge gap remains on how to measure the success of current procedures, in terms of patient’s satisfaction and improvement of QoL (Nolan et al., 2019).
Affirmation needs and specific concerns for passing depend on the person’s sense of self, but they are also influenced by the sociocultural environment. High gender affirmation needs coupled with a lack of access to gender affirmation in social, medical, and legal contexts lead to a riskier transition and negative health outcomes (Glynn et al., 2016; Sevelius, 2013). The World Professional Association for Transgender Health emphasizes the importance of improving access to GAPs (WPATH, 2012).
In Mexico, transgender health programs focus mainly on the prevention and treatment of sexually transmitted infections (STIs), HRT, and psychological support (Enriquez-Estrada, 2019). Access to voice feminization is limited due to the few qualified physicians and centers offering these services (Safer et al., 2016). A financial barrier also exists, as these procedures are not covered by insurance companies and neither are offered in most public health facilities (APA, 2015). After a thorough search, we were unable to find specialized Mexican literature focused on voice non-conformity in TW. Articles focused on transgender health in Mexico do not consider management of transgender voice and do not include the participation of otolaryngologists nor speech therapists as part of the multidisciplinary team assisting these people (Ramírez-Rentería et al., 2018). The number of TW demanding voice feminization is increasing (Schmidt, Goulart, Dorfman, Kuhl, & Paniagua, 2018). Understanding what causes and mitigates voice-related gender dysphoria is an initial step for designing protocols to produce patient-centered, evidence-based recommendations. Increasing visibility of a problem that has not been sufficiently represented is also essential to improve access to voice feminization procedures.
The main objective is to describe the degree of voice-related dysphoria experienced by Mexican TW and what drives them to seek voice feminization. A secondary objective was to determine if f0 correlates with the scores obtained with QOL questionnaires and self-perception of voice.
Method
Subjects
The inclusion criteria were to identify, oneself as female while being assigned male at birth, being older than 18 years old, and having expressed a desire to undergo vocal feminization treatment. Participants were requested to either provide a referral from a mental health specialist or a transgender health professional or to be legally recognized as women. TW who lacked either requirement but were interested in the study were evaluated after referral to a clinic specialized in human immunodeficiency virus (HIV) prevention that offers health services to the transgender population in Mexico City. The exclusion criterion was structural laryngeal pathology.
Participants were 26 TW voluntarily seeking voice feminization treatment at the Otolaryngology Department of the Instituto Nacional de Rehabilitación in Mexico City, during July 2019 and March 2020. This report is a data analysis of the participants’ records obtained before voice feminization.
For recruitment purposes, information regarding voice feminization services was provided to physicians working at the afore mentioned clinic, which provides transgender health services, psychiatrists with interest in the trans population, trans activists, and civil associations focused on the trans community. The three authors also attended Mexico’s City 2019 Sexual Diversity and Pride Parade to provide information. The clinic specialized in HIV prevention and the association Red de Familias Trans turned out to be effective recruiting channels. The participants of the study started a snowball effect with their friends and acquaintances.
Measurements
Sociodemographic data, history of gender transition, referral, treatment expectations, voice related QoL measures, self-perception of voice, and voice recordings were obtained.
A laryngeal endoscopy was performed to exclude structural laryngeal pathology.
A structured interview was performed. Sociodemographic data and referral information were obtained through close-ended questions, such as: “How old are you?” To determine the history of gender transition open-ended and close-ended questions were done, such as: “What has been your experience with gender transition?,” “Are you taking hormone replacement treatment?,” “Have you undertaken gender affirmation procedures, including but not limited to: breast augmentation surgery, tracheal shave, facial feminization surgery, voice feminization surgery, orchiectomy, feminization genitoplasty?”
To measure QoL, the validated Spanish versions of the Voice Handicap Index (VHI) and the Trans Woman Voice Questionnaire (TWVQ) were applied.
The VHI is the most widely used instrument for assessing self-perceived handicap associated with voice disorders. It contains 30 statements organized into three subgroups. Each subgroup contains 10 statements that reflect the physical, functional, and emotional aspects of the voice handicap. The participant is asked to read each statement and indicate how often that statement applies to her situation on a 4-point Likert-type scale (0 = never to 4 = always). If each subscale is evaluated independently, possible scores range from 0 to 40, while the possible total VHI scores range from 0 to 120. Higher scores translate to a higher self-perceived handicap (Jacobson et al., 1997). In 2007, the instrument was translated and validated in Spanish. This version has a Cronbach’s alpha of .93 (Núñez-Batalla et al., 2007). Despite the extensive use of the VHI, it was not designed to evaluate concerns specific to TW. The first attempt to create a self-evaluation tool for trans voices was the Transgender Self-Evaluation Questionnaire (TSEQ). An extensive review of the TSEQ led to the development of the Transsexual Voice Questionnaire for Male-to-Female Transsexuals (TVQ MtF), which has a Cronbach’s alpha of .964 (Dacakis, Davies, Oates, Douglas, & Johnston, 2013). In 2017 it was adapted to Spanish. This version has a Cronbach’s alpha of .976 and an intraclass correlation coefficient of .885 (Mora et al., 2018). The TVQ MtF was renamed the TWVQ in July 2020. The TWVQ contains 30 items assessing the impact of the voice on the participant’s experience living as a woman. The items are rated with a 4-point Likert-type scale (1 = never or rarely to 4 = frequently or always), and possible scores range from 30 to 120. Higher scores reflect that the subject considers her voice hinders her experience living as a woman, which interferes with her QOL.
Self-perception of voice is also specifically assessed in the TWVQ. Additionally to the 30 items evaluated, the TWVQ instructs the subject to “provide an overall rating of your voice” in current and ideal situations. Options given are: “very feminine, somewhat feminine, neutral, somewhat masculine, or very masculine.”
To evaluate the motivation to seek voice feminization procedures, TW were also asked: “What do you expect to achieve from a voice feminization treatment?”
Each speaker was recorded while reading out loud the Grandfather Passage in Spanish, a standardized test for the evaluation of speech (Contreras, Muñoz, Prieto, & Valdés, 2017). The recordings were analyzed using the phonetic software Praat, version 6.1.13 to obtain the f0.
Subjects received no economic, material, or any other compensation for participating.
Statistical analyses
Descriptive statistics were performed by exploratory analysis
To assess the reliability of the VHI and the TVWQ, Cronbach’s alphas were obtained. The value of Cronbach alpha ranges from 0 to 1. Values closer to 1 represent a greater internal consistency for the items in the scale. The Shapiro-Wilk test determined the normality of the variables and then the dispersion and central tendency values were obtained. Either a Student’s t-test or a Wilcoxon test was performed to evaluate the differences between TW enrolled in therapy and those programmed for surgery. The selection of the test was based on the distribution of data, and a Wilcoxon test was chosen to evaluate data that did not follow a normal distribution. According to the characteristics of variables, either a Spearman or a Kendall correlation test was done to determine the relationship between f0, the scores obtained from the VHI and TWVQ, and the self-perception of voice. A significance level of 5% was considered for the tests performed.
All analyses were carried out with the software IBM SPSS Statistics version 26.
Results
Of the 116 TW that asked for information about voice feminization treatment, 31 made an appointment at the otolaryngology department where an explanation of the pros and cons of each voice feminization treatment was given (Table 1).
Table 1 Comparison between therapy and vocal cord surgery for voice feminization
| Therapy | Surgery |
|---|---|
| Non-invasive. | Invasive. |
| Low risk to no risk of complications. | Risk of complications, some severe and irreversible. |
| Does not limit the vocal range. | It limits the vocal range. |
| It requires practice, hence patients must go to the office sev- eral times per week for several weeks. |
It requires absolute vocal rest for 3 weeks. |
| It requires voluntary control. | It does not require voluntary control. |
| A deep voice may reappear in spontaneous moments, such as laughter. |
The high voice is maintained during spontaneous mo- ments, such as laughter. |
| After some time, the changes accomplished might fade away partially or completely. |
Changes accomplished after surgery are more stable over time. |
| Low to moderate ability to increase the vocal pitch. | Higher ability to increase the vocal pitch. |
| It aims to modify the resonance, articulation, choice of words, and other aspects of language. |
It mainly modifies the fundamental frequency. |
Note: Adapted from Casado, O´Connor, Angulo, & Adrián, 2016; Hancock & Helenius, 2012; Nolan et al., 2019.
Of the 31 subjects evaluated at the office, the following five were not included in the study. One desired surgery but was not medically fit to undergo general anesthesia for elective procedures and declined speech therapy. Another participant was taking HRT without medical supervision, so she was referred to an endocrinologist and did not return. Another participant had not made a full-time social transition and decided to postpone voice feminization. Two more participants mentioned they did not have the resources to attend hospital appointments regularly.
Twenty-six TW were included in the study. Twelve enrolled in vocal therapy and 14 were programmed for surgery (Table 2 for demographics). One of the participants enrolled in vocal therapy was a professional singer, so a recommendation against surgery was provided in her case. Another one was initially more inclined toward surgery but considered it was more expensive and decided to enroll in a therapy program instead.
Table 2 Characteristics of participants according to the type of preferred voice feminization treatment
|
All
(N = 26) |
Vocal therapy
(N = 12) |
Vocal cord surgery
(N = 14) |
Statistical
differences |
|
|---|---|---|---|---|
| Age x̅(SD) | 34 (8.05) | 33 (8.29) | 35 (7.9) | .56 |
| Residence in Mexico City metropolitan area | 26 (100%) | 12 (100%) | 14 (100%) | - |
| Time since social transition (years) Mdna (Q1,Q3) | 10.5 (2-19) | 4.5 (1.25-14.5) | 13.5 (4.5-22.5) | .12 |
| Living with HIV | 3 (11%) | 2 (16.7%) | 1 (7%) | .46 |
| Current HRT | 25 (96%) | 11 (92%) | 14 (100%) | .46 |
| History of GAS | 7 (27%) | 2 (16.7%) | 5 (36%) | .28 |
| Legally recognized as women | 20 (77%) | 9 (75%) | 11 (79%) | .82 |
| Fundamental frequency in Hz Mdna (Q1,Q3) | 131 (120.75-157.75) | 138 (121.75-161.25) | 126.5 (117-146) | .32 |
| VHI emotional subscale** x̅(SD) | 24 (9.65) | 23 (12.25) | 25 (7.11) | .66 |
| TWVQ score** x̅(SD) | 95 (14.3) | 93 (17.4) | 97 (11.3) | .47 |
| Voice perceived as masculine* | 21 (81%) | 12 (100%) | 9 (64%) | .02 |
| Voice perceived as neutral | 5 (19%) | 0 (0%) | 5 (36%) | .02 |
Notes: x̅ (SD) were used to summarize parametric variables, Mdna and Q1,Q3 for non-parametric variables, and Freq (%) for dichotomic variables. Self-perception of voice was classified as: very feminine, somewhat feminine, neutral, somewhat masculine, or very masculine.
*This percentage represents the sum of TW that classified their voices as very masculine and somewhat masculine.
**Possible scores for the QoL questionnaires are: TVWQ score (30-120), VHI emotional subscale (0-40).
Abbreviations: x̅ = mean; (SD) = standard deviation; Mdna = median; Q1,Q3 = first quartile, third quartile; Freq = frequency; HIV = Human Immunodeficiency Virus; HRT = Hormonal Replacement Therapy; GAS = Gender affirmation surgery; Hz = hertz; VHI = voice handicap index; TWVQ = Trans Women Voice Questionnaire.
The mean age was 34 (SD = 8) years old, all participants lived in the Mexico City metropolitan area. 57% were referred from a clinic specialized in HIV prevention. Despite the nexus with that clinic, only 11% of the participants evaluated were living with HIV; all were undetectable and had a CD4 count > 500 c/mm3. All had an HIV screening test done once a year.
The median time living as a woman was 10 years and six months. Nevertheless, most women clarified that they had identified themselves as women since childhood. One of the participants had her birth certificate changed when she was a child, so she did not consider that she had undergone a social transition. 77% of the participants were legally recognized as women. 96% were currently under HRT, and 27% had a history of gender affirmation surgery (GAS) including facial feminization surgery, breast augmentation, and orchiectomy. None had undergone vocal cord surgery nor chondrolaryngoplasty. Participants denied receiving structured vocal feminization therapy, but five participants recognized they had tried vocal feminization exercises posted on YouTube.
The two QOL questionnaires demonstrated high overall reliability, with a Cronbach’s alpha of .89 for VHI and .961 for TWVQ. The degree of dysphoria related to voice was better represented by the TWVQ, with a mean score of 95 (SD = 14.3). The median score for VHI was 59. Eighty-one percent of the participants considered their voices to be either very masculine or somewhat masculine, and the rest considered their voices neutral. Self-perception of voice was the only trait where a statistically significant difference was found between the TW enrolled in therapy and those programmed for surgery, with the latter more likely to perceive their voices as neutral.
Regarding expectations, 62% considered their ideal voice would be very feminine, 35% somewhat feminine, and 3% neutral. Open answers obtained from the question “What do you expect to achieve from a voice feminization treatment?” were classified into six groups. Eighteen participants mentioned a single reason to seek voice feminization, of whom 61% said they wanted a more feminine voice, 22.2% to achieve a voice that “does not betray me”, 5.5% to have fewer social and work conflicts, and 11.1% to lessen the effort required to maintain a feminine voice during spontaneous reactions, like laughter. To feel more confident or less anxious is considered a minor reason because only three participants stated this to be a concern and it was never stated by itself. The two expectations classified as “other” were mentioned as secondary objectives by two participants: “I expect to observe an objective rise on my fundamental frequency” and “I do not want to sound like a teenager.” TW mentioned they are recognized as men more frequently when the interaction is only by the telephone; hence, being recognized as women on the telephone was the ultimate test of passing for some.
Median f0 for TW was 131 Hz, but there was a wide range of f0 values. Five participants (19.2%) had an f0 > 165 Hz, 18 participants (69.2%) had an f0 < 145 hz, and 3 (11.6%) had an f0 between 145-165 hz. this is relevant because based on values alone, only 18 tw should perceive their voices as masculine, five of them feminine. contrasts with the participants’ self-evaluation, where 21 perceived masculine none feminine (Figure 1).
No correlation was found between f0 and TVWQ score, rs (24) = .278, p = .169, VHI score, rs (24) = .324, p = 106, or self-perception of voice, rs (24) = .233, p = 162. There was a significant positive correlation between TVWQ score and VHI score, rs (24) = .674, p < .001.
Discussion and conclusion
Reports on the degree of dysphoria and measurements of QoL are inconsistent in the published literature, as has been shown by the systematic reviews and meta-analysis available (Nolan et al., 2019). Compared to existing reports, participants in this series displayed higher levels of voice-related dysphoria. QoL scores in this study were 59 on the VHI and 95 on the TVWQ, compared to previously reported VIH scores of 32 (Mastronikolis, Remacle, Biagini, Kiagiadaki, & Lawson, 2013), and 45.5 (Remacle, Matar, Morsomme, Veduyckt, & Lawson, 2011), and a TWVQ score of 66 (Dacakis et al., 2017). Other authors have used visual analog scales that are not validated (Meister et al., 2017) or reported TSEQ scores (Casado, O’Connor, Angulo, & Adrián, 2016) which are not entirely comparable to TWVQ. These studies were carried out in Australia and Europe. Stigma, discrimination, and overt violence against transgender people are more prevalent in Latin America (Malta et al., 2019). This difference is relevant because perceived discrimination increases the risk of poor QoL in TW with gender dysphoria (Hasan, Alviany, Clarissa, & Sudana, 2017) and could partially explain the results obtained in QoL measurements. Nevertheless, it should be noticed that higher TWVQ scores have been associated with anxiety and depression symptoms (Novais Valente & Mesquita de Medeiros, 2020) which is why these results are worrisome. A selection bias could also be related.
Compared to another study evaluating characteristics of trans people living in Mexico, participants in this study were older, had better access to HRT and GASs, and were more likely to have had HIV and other STI screening tests (Lozano-Verduzco & Melendez, 2019). A possible explanation is that TW who are actively searching for vocal feminization treatments have already resolved some of the other issues faced by trans people and might be more focused on voice-gender incongruence than the TW population that is not seeking these procedures. Only 26.7% of the TW who asked for information made an appointment at the clinic. Reasons for not making an appointment were not explored, but some TW mentioned that staying in Mexico City for several weeks was not financially feasible for them, others mentioned they lacked an appropriate support network or that their families had prohibited any involvement in programs oriented to gender transition.
Mean f0 was in the range of mean f0 values reported in a meta-analysis that included Spanish-speaking and non-Spanish speaking TW (Song & Jiang, 2017). 30.8% of the participants had an f0 > 145 HZ, so we consider that some TW learn (intuitively or by using tutorials) to raise their f0. Nevertheless, TW that reached an f0 on the feminine spectrum maintain high levels of voice-related dysphoria. They do not perceive their voice as feminine, even when they recognize they could “force themselves to sound feminine” for short periods but fail to do so constantly during daily social interactions. It would be relevant to determine if their self-perception correlates with the perception of others, and how that relates to QoL. A study found that TW who considered their voices adapted to the desired gender, and had lower VHI scores, had their voices identified more frequently as females by naïve listeners (Schmidt et al., 2018). A strong correlation between patient satisfaction and being perceived as female on the phone, regardless of f0 values, has also been found (Meister et al., 2017). Another study found that self-perception had a stronger effect on QoL than the perception by naïve listeners (Hancock, Krissinger, & Owen, 2011). Also, we did not explore if any of the participants presented internalized transphobia, which has been related to an overemphasis on passing (Bockting et al., 2020). This would be interesting to investigate in TW who continue to perceive a masculine voice and report voice-related dysphoria despite having an f0 > 165 HZ and a voice that is perceived by others as feminine. In contrast to findings in previous research (Dacakis et al., 2017) TVWQ scores in this study were not negatively correlated with self-perception. This may be due to the smaller sample size of this study, higher mean TVWQ scores in our sample, or unidentified confounding factors such as differences in social tolerance and discrimination of TW among different cultural environments.
Concerning the preference for surgical vs. non-surgical voice feminization treatments, we had anticipated that TW with higher TWVQ scores and a history of GAS would be more inclined toward surgery than speech therapy. However, the only difference between surgical and non-surgical groups was self-perception of voice. The five participants that considered their voices neutral preferred surgery. Four of them chose surgery because they intended to maintain a feminine voice with no effort and avoid the production of a deeper voice during laughter. Currently, there is no consensus for selecting one type of treatment over another. Studies published by surgical groups (Thomas & MacMillan, 2013) tend to favor vocal cord surgery, while those published by speech therapists tend to favor therapy (Carew, Dacakis, & Oates, 2007; Hancock & Helenius, 2012), and others support a bimodal treatment (Casado, Rodríguez-Parra, & Adrián, 2017). Until better designed studies are performed, we suggest the decision to depend on the resources available and the person’s preference.
While carrying out this study we noticed that a group of residents and consultants, whose specialties are not directly involved in transgender healthcare, had little information about TW and their health needs. Familiarity with the transgender community leads to more positive attitudes toward transgender people (Luhur, Lozano-Verduzco, & Shaw, 2020). We, therefore, gave seminars to increase sensitivity towards trans people and issues. During these seminars, some colleagues expressed that “GAPs are equivalent to cosmetic medicine and consequently public resources should not be destined for these procedures”. This misconception is a barrier to adequate and accessible transgender healthcare. The key reasons reported for undertaking cosmetic surgery are the pressure to look younger, media influence, having a “celebrity look,” influence of family or friends, improving sex life, increasing self-esteem, and bullying, among others (Nuffield Council on Bioethics, 2017). In contrast, the main reasons reported for undertaking voice feminization treatments are obtaining gender conformity or passing. The inability to satisfy gender assurance needs leads to negative health outcomes such as a higher rate of STIs, drug abuse, and suicide (Sevelius, 2013). Besides gender assurance, one of the motivations for passing is fear of discrimination and violence due to transphobia (Anderson, Irwin, Brown, & Grala, 2020; Dias, da Rocha, Tateo, & Marsico, 2021). Mexico is second only to Brazil in the number of hate crimes against transsexual people (Balzer, LaGata, & Berredo, 2016). More studies are required to analyze if GAPs protect against discrimination and transphobic acts.
The findings of this study must be interpreted in light of some limitations. Due to recruitment issues, we had a small sample size and a possible selection bias. Regarding methodology, we could have had the voices analyzed by naïve listeners. Exploring the participants’ experience of discrimination, transphobia, mental health disease, and reasons for not participating in the study would have been interesting.
We can conclude that voice non-conformity can be an important source of dysphoria and that neither psychotherapy nor HRT is sufficient to mitigate voice-related dysphoria in some TW. Addressing voice-related gender dysphoria, and referral to institutions that can provide voice feminization procedures, could have positive effects on the QoL of TW undergoing gender transition (Hancock et al., 2011). Improving access to GAPs, including voice feminization, in public institutions is a pending agenda. Transgender voice services should be offered in the context of a holistic approach to transgender health (Davies, Papp, & Antoni, 2015). Improving knowledge of the trans community and their healthcare needs among healthcare workers is also a pressing need (de Vries, Kathard, & Müller, 2020).
Despite evidence that TW benefit from voice feminization treatments (Van Damme, Cosyns, Deman, Van den Eede & Van Borsel, 2017), it is difficult to define how to measure success (Nolan et al., 2019). We recommend the use of QoL questionnaires, assessment of self-perception, and assessment by naïve listeners to measure results in future research. The goals and expectations of TW should also be considered before any voice feminization treatment is started. TW tend to have very high expectations, and these should be addressed and managed with caution.

