











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Health systems worldwide keep radical protocols and strategies for emerging and reemerging diseases. These rigid measures can counteract epidemics and pandemics among the population, protecting physical health, especially in vulnerable people. One of these measures is quarantine, which involves separating and restricting the movement of people who have potentially been exposed to a contagious disease, thereby reducing the risk of infecting others. This definition differs from isolation, which involves separating people who have been diagnosed with the disease (Brooks et al., 2020).
At present, a new coronavirus, called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has infected the human population and a pandemic has developed that has altered the psycho-socioeconomic fabric of the world population. This virus has caused a large number of deaths and tens of thousands of confirmed cases worldwide, posing a serious threat to physical and mental public health (Li, Liu, Yu, Tang, & Tang, 2020).
A virus with a pandemic potential must be exhaustively monitored to prevent both direct and indirect clinical and epidemiological manifestations (de Jong, Claas, Osterhaus, Webster, & Lim, 1997), which is the basis for building first-line plans for its containment and, if possible, eradication (Kuri-Morales, Betancourt-Cravioto, Velázquez-Monroy, Alvarez-Lucas, & Tapia-Conyer, 2006). A pandemic has direct effects on health, due to its effects on the functioning of the organism, and indirect effects, such as the attitudes, perceptions, and psychological distress caused in a population (Perrin, McCabe, Everly, & Links, 2009), and in some cases secondary effects have greater repercussions on social functioning than primary ones (Cheng & Cheung, 2005), since this forces the population to undergo emergency isolation to avoid future risky infections. In response to this outbreak, quarantine has been implemented in Mexico, as well as in other countries, as a measure to prevent and control the pandemic. The population most susceptible to severe cases are the elderly and people with underlying diseases or low immune function and pregnant women, while infected newborns are prone to developing severe pneumonia (Li et al., 2020). The costs of epidemics and pandemics, as well as the measures implemented, such as quarantine, not only encompass economic and cultural issues, but also negative psychological effects such as post-traumatic stress symptoms, confusion and anger, as well as fear of infection, frustration, boredom inadequate supplies, inadequate information, financial losses, and stigma. Some studies suggest that these effects can be long-lasting (Brooks et al., 2020).
The idea that social isolation is extremely dangerous for mental health is not necessarily new, with findings clarifying the magnitude of its effect on other populations, both pathological and healthy (Andersson, 1998). They also demonstrate that isolation and/or loneliness have more detrimental effects on mental health service users than the general population (Lauder, Sharkey, & Mummery, 2004). In previous studies, a relationship between the feeling of isolation and loneliness (I&L) and the presence of anxiety (Caplan, 2007) and suicidal behavior (Goldsmith, Pellmar, Kleinman, & Bunney, 2002) has been demonstrated. Interventions to lessen the detrimental effects of I&L have had a strong impact on the population suffering from it (Windle, Francis, & Coomber, 2011), especially in reducing worry and uncertainty levels (Butler, 2006).
Worry is essentially the core of anxiety, as this is a sequence of anxious thoughts with a highly emotional content usually directed towards the future (Kelly & Miller, 1999), which, in turn, are prone to appear during I&L (Flett, Goldstein, Pechenkov, Nepon, & Wekerle, 2016). Although they are a phenomenon commonly experienced on a day-to-day basis, worry is a concept associated with stress and anxiety (Hirsch & Mathews, 2012), although they are not synonymous in phenomenological terms (Davey, 1993). Previous studies have reported that approximately 72% of people experience severe worry at least once a month (Tallis, Davey, & Capuzzo, 1994). However, pathological worry is a risk factor during pandemics. This type of worry is perceived as excessive and uncontrollable for the person experiencing it (Davey, 1994).
Therefore, due to the recent outbreak of COVID-19, which had its epicenter in China and has spread globally (Dong & Bouey, 2020), certain forms of mental health care have been developed that seek to prevent harmful effects due to the constant worry about infection, uncertainty and isolation (Jiang et al., 2020; Liang, Mays, & Hwang, 2017). And as has been the case with other pandemics such as H1/N1, stronger anxiety outbreaks will occur during phases two and three that will significantly decline during the last phase (Bults et al., 2011) since it is a natural response to pandemics, as has been observed in previous experiences (Wheaton, Abramowitz, Berman, Fabricant, & Olatunji, 2012). Knowing, relatively accurately, the effects on mental health due to I&L (Taha, Matheson, Cronin, & Anisman, 2014) and monitoring the perceptions and behavioral responses of the general public enables us to obtain useful information for future measures in response to pandemics (Taylor et al., 2009). This has been the case in previous years. A series of studies on risk perception and responses in the case of 2009 influenza were published, which enabled the development of preventive measures for the population (Seale et al., 2010).
Overestimation of both the positive and negative consequences of excessive, uncontrollable worry is one of the characteristics of Generalized Anxiety Disorder and other mood disorders (González, Bethencourt, Fumero, & Fernández, 2006). This variable and its related aspects have been evaluated through various instruments, such as the following: Why worry?, the Intolerance of Uncertainty Scale (IUS) (Freeston, Rhéaume, Letarte, Dugas, & Ladouceur, 1994), the White Bear Suppression Inventory (WBSI) (Wegner & Zanakos, 1994), The Problem Solving Inventory-Revised (Maydeu-Olivares & D’Zurilla, 1995), Beck’s Anxiety Inventory (BAI) (Beck, Epstein, Brown, & Steer, 1988), the Structured Interview Guide for the Hamilton Anxiety Scale (SIGH-A) (Shear et al., 2001), the Penn State Worry Questionnaire (PSWQ) (Meyer, Miller, Metzger, & Borkovec, 1990), and so on. All the above instruments are reliable and valid and have been used in various populations for studies on worry.
The latter is an instrument validated in Mexican population that is ideal for the evaluation of pathological worry, as well as being useful in clinical contexts. Studies have analyzed the psychometric properties of the Penn State Worry Questionnaire (PSWQ) in its Spanish versions: the original scale (PSWQ-16) (Meyer et al., 1990), the direct form of the scale PSWQ-16D (Ruiz Díaz, Montorio Cerrato, & Nuevo Benítez, 2002), and two abbreviated versions PSWQ-11 (Sandín, Chorot, Valiente, & Lostao, 2009) and PSWQ-8. In this regard, it has been determined that the original scale (PSWQ-16) is built according to a model of two related factors, in contrast to the analysis of the PSWQ-16D, PSWQ-11, and PSWQ-8 versions built under a single factor (one-dimensional). In all cases, high internal consistency and test-retest reliability and adequate concurrent and discriminant validity were identified (Padrós-Blázquez, González-Betanzos, Martínez-Medina, & Wagner-Echeagaray, 2018).
Regarding the assessment of perceived exposure, vulnerability, and risk of contagion to diseases, there are several instruments designed for specific clinical contexts, such as HIV infection (Bayés, Pastells, & Tuldrá, 1995), avian influenza (Fielding et al., 2005), and so on. Also in the context of alarming public health situations, research has been conducted on perceived vulnerability to influenza A (H1N1), in which four main dimensions were identified: catastrophic power, threat, control, and knowledge of participants (Aragonés, Talayero, & Olivos, 2010). The scale of perceived vulnerability to the disease has also been used (Magallares, Fuster-Ruiz De Apodaca, & Morales, 2017) in the SARS-CoV-2 contingency (González-Olmo, Ortega-Martínez, Delgado-Ramos, Romero-Maroto, & Carrillo-Diaz, 2020), which includes two subscales: perceived infectivity and germ aversion, both with acceptable internal consistency measured by Cronbach’s alpha.
In this regard, it is important to mention that both evaluation of pathological worry in the general population and the perceived risk of contagion in extreme epidemiological situations such as the one we are currently experiencing as a result of COVID-19, is crucial for identifying indicators of vulnerability to psychopathology and exposure to risk situations among the general population. Although the PSWQ-16 and PSWQ-11 questionnaires have already been used in Mexican population samples (Padrós-Blázquez et al., 2018), even in patients in the clinical context (Velázquez Díaz, Espinoza González, Martínez Medina, & Padrós Blázquez, 2016), and also in relation to generalized anxiety disorder (Starcevic, 1995), neither the prevalence nor the association between pathological worry and perceived risk of SARS-CoV-2 in Jalisco have been established. This study therefore has various objectives, the first one being to determine the prevalence of worry in a Guadalajara population during the COVID-19 quarantine. The second objective was to construct and implement an instrument to measure the perceived risk of contagion. The last objective was to identify variables with a differentiating effect in worry in the population under study.
Method
Participants
A convenience sampling was carried out of people who were close to the mental health services of the College of Psychology Professionals in the state of Jalisco and social networks of the University of Guadalajara, who wished to participate voluntarily. A total of 255 subjects from western Mexico (Guadalajara, Jalisco) participated voluntarily. The average age of subjects between 18 and 70 years was 31.71 (± 5.19), who answered the Penn State Worry Questionnaire (PWSQ) adapted to Mexican population by Padrós-Blázquez et al. (2018). The distribution by sex was 33.33% (85) men and 66.67% (170) women. In addition, they were asked about the number of days they had been self-isolated, regardless of whether this had been voluntary or obligatory. Of the total sample, 81.5% had been self-isolated for between five and 10 days, while the remaining 18.5% answered it when they had done so for 10 to 25 days.
Measurements
Of the instruments validated for Mexican population, the PSWQ-16 was used in its Spanish version with 16 5-level Likert-type items where 1 is scored as nothing and 5 as very much. Eleven items are direct and five are inverse (1, 3, 8, 10, and 11) and evaluate the general tendency to worry or worry-trait, which appears to play an important role in generalized anxiety disorder. The scale has an alpha of .917, X2 = 404.23, gl = 104, p < .001, CFI = .91, TLI = .90, and RMSEA (90% CI) = .06 [.05, .08], which seems to indicate a reliable, stable instrument for the evaluation of the construct (Padrós-Blázquez et al., 2018). To determine the participants' state of worry, a calculation was made through standardization where the mean and standard deviations of the expected scores were obtained (41.70 ± 10.97). The intervals used are shown in Table 1.
Procedure
The questionnaire was applied individually from March 22 to April 3, 2020 by filling in the scale on a table or computer. Data were stored virtually to be analyzed later. At the time of application, instructions were given verbally and in writing. Subjects read and accepted the informed consent before answering the scale, and were informed that the study adhered to the ethical code established by the Official Mexican Norm regarding research with human beings (NOM-012-SSA3-2012), and it was also specified that the data obtained would only be used for research purposes and that the privacy and identity of the participants would be protected. The average time they took to answer the questionnaire was 4:03” (± 2:32”) minutes.
Statistical analyses
Statistical tests were performed in Software R version 3.6.3 (R Core Team, 2020). For the treatment of data, the Kolmogorov-Smirnov normality test was submitted, obtaining scores that confirm a non-parametric treatment of the data (p < .05). Data that were treated in a non-parametric way were tested with a Mann Whitney’s U test to determine whether there were differences by group for the total PSWQ score. Additionally, when the data allowed, Cohen’s d (d) was calculated for the effect size and derived from the latter, the overlap index (OVL), which enables us to know the percentage of intersection observations have in scores.
Ethical considerations
The Project was approved (SELPUDGA00421320) by the Ethics Committee of the Society of Graduates of the Degree in Psychology A.C., and was developed according to institutional ethical standars and those established by the Declaration of Helsinki. All participants signed informed consent which safeguards the voluntary and free participation of the participants in the study. In addition, it ensured the follow-up of the participants identified with high concern and taking care of anonymity.
Results
Figure 1 shows the categories into which the sample to be studied was distributed, with 58.6% of participants obtaining scores within expectations (44.69 ± 4.75). The remaining 30.6% scored high levels of worry (56.39 ± 2.94) with only 10.6% obtaining scores reflecting alarm (67.48 ± 4.10). Within these, 50.59% answered that they were self-isolating although 49.41% said they were not. Attempts were made to determine whether there was a differential effect between the groups that were in total isolation and the PSWQ scores where no significance was obtained (Table 2).
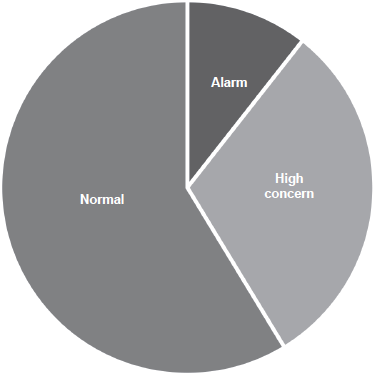
Table 2 Differences in PSWQ in groups by sex, educational attainment, and occupational demandingness
| Variables | PSWQ | U | p | d | OVL | |
|---|---|---|---|---|---|---|
| Sex | Woman | Man | ||||
| 52.32 ± 9.15 | 47.40 ± 7.30 | 9455.5 | .001* | .60 | .76 | |
| Occupational demandingness | Low | HIgh | ||||
| 49.53 ± 8.50 | 51.23 ± 9.02 | 7768.5 | .210 | .19 | .92 | |
| Educational attainment | HE | Graduate | ||||
| 48.88 ± 8.01 | 50.26 ± 7.68 | 900 | .673 | .18 | .92 | |
| Isolation | Yes | No | ||||
| 51.48 ± 9.05 | 49.87 ± 8.65 | 7120 | .087 | .18 | .92 | |
Notes: U = Mann Whitney’s U; p = Significance; d = size effect; OVL = Cohen’s d overlap coefficient; HE = higher education;
*p < .01.
Table 3 shows the answers to questions on contagion measures, attitudes, and behaviors towards COVID-19. The questions that were answered were: Have you had contact with someone with symptoms? (Primary contact), Do you think that you observe the hygiene rules properly? (Hygiene), Do you think any of your nuclear relatives (parents and/or siblings) has symptoms? (Nuclear family contagion), Do you think that any of your extended relatives (cousins, uncles and/or grandparents) has symptoms? (Contagion extended family), Do you think that any of your nuclear contacts (close friends and/or partner) has symptoms? (Contagion in nuclear relations), Do you think any of your extended contacts (neighbors, acquaintances, frequent friends) has symptoms? (Contagion in extended relationships), and Do you consider that your actions have a significant impact on preventing the spread of COVID-19? (Impact).
Table 3 Sample’s answers to questions about contagion measures, behaviors adopted and isolation due to suspected COVID-19 in Jalisco
| Isolation | ||
|---|---|---|
| Variables | No | Yes |
| Primary contact | ||
| Perhaps | - | - |
| No | 120 | 125 |
| Yes | 6 | 4 |
| Hygiene | ||
| Perhaps | 47 | 37 |
| No | 5 | 1 |
| Yes | 74 | 91 |
| Nuclear family contagion | ||
| Perhaps | 5 | 7 |
| No | 120 | 119 |
| Yes | 1 | 3 |
| Extended family contagion | ||
| Perhaps | 10 | 12 |
| No | 111 | 115 |
| Yes | 5 | 2 |
| Nuclear relatives contagion | ||
| Perhaps | 12 | 20 |
| No | 107 | 102 |
| Yes | 7 | 7 |
| Extended relatives contagion | ||
| Perhaps | 27 | 26 |
| No | 91 | 11 |
| Yes | 8 | 92 |
| Impact | ||
| Perhaps | 26 | 19 |
| No | 8 | 10 |
| Yes | 92 | 200 |
Given that the best way to determine the probability of being infected is based on contact and isolation, scores were given to the questions asked in the questionnaire, and determined as follows: Isolation (Yes [0], No [1], Maybe [.5]), Primary contact (Yes [1], No [0], Maybe [.5]), Hygiene (Yes [0], No [1], Maybe [.5]), Contagion nuclear family (Yes [1], No [0], Maybe [.5]), Contagion extended family (Yes [1], No [0], Maybe [.5]), Contagion nuclear relatives (Yes [1], No [0], Maybe [.5]), Contagion extended relatives (Yes [1], No [0], Maybe [.5]), Impact (Yes [1], No [0], Maybe [.5]). The total sum was obtained directly in such a way that the higher the score, the higher the risk. Once the risk score had been obtained, a correlation was made with the score obtained on the scale of worry to determine the level of relationship between these two variables, from which Figure 2 was obtained.

Figure 2 Scatter graph of total score of scale and score obtained from risk due to contact in Jalisco population. Spearman’s p = .1; p = .111.
Additionally, we were interested in knowing whether sex, education, and occupational demandingness played an important role in the perception of worry. These three aspects were compared, separating for this variable. For the educational attainment comparison, the two educational extremes were considered: Higher education (50) and Postgraduate (38). In order to determine occupational demandingness the occupational index was used with the considerations proposed by Stern et al. (1994) that resulted from a general census. These occupation categories were: 1. Non-professionalized student (elementary, middle, high school); 2. Homemaker; 3. Non-specialized or semi-specialized (non-professional employees); 4. Employees by trade (carpenter craftsmen, merchants or electricians); 5. Employment careers (general employees, clerks or clerics); 6. Advanced job careers (managers, entrepreneurs or high-ranking public servants); 7. Professional or higher university technician. For the purposes of this article and to be able to obtain two comparable groups, the low requirement group (82), belonging to categories 1 to 5, and the high requirement (173) of categories 6 and 7 were obtained.
Discussion and conclusion
The first objective of the study was to determine the prevalence of worry in the Guadalajara population during the COVID-19 quarantine through a convenience sample. It is necessary to clarify the implications of this type of sampling at this point. Among the possible biases is the lack of randomization together with low variability in the population, as a result of which there could be a tendency for only those who felt uncomfortable or worried beforehand answering the questionnaire. However, we observed that there appears to be no significant difference between people who measure the amount of worry they feel and those who do not, which could be considered a solution to this bias. At the same time, caution is required when interpreting the data since it might be difficult to generalize to all social strata in Jalisco, considering that there may be people who do not have contact with the university’s social networks or are older adults.
Another possible bias in this type of sampling is the fact that the replicability of the study could pose a problem since the characteristics of time or place of the population would no longer be available if the same population could be used. This would make it partly impossible to undertake with a different population due to the inability to replicate the characteristics of the first sample. However, for future studies, attempts are being made to do a retest with a random sampling of the sample to determine whether it has evolved in accordance with the number of days of self-isolation.
According to our results, it was found that 10.6% of the sample had worry levels at least two standard deviations above the mean, which can be regarded as pathological according to the instruments, while 30.6% had levels of concern one standard deviation above the mean, classified as high. This means that a total of 40.12% of the sample could develop some symptoms due to involuntary self-isolation since excess worry is related to generalized anxiety disorder (Padrós-Blázquez et al., 2018).
As for the attitudes, behaviors, and perceptions surrounding the risk of contagion, favorable responses for prevention were observed in most individuals. Answers (Table 3) were tabulated according to frequency and arranged according to the answers on self-isolation. For the primary contact question, it was found that regardless of the length of self-isolation, subjects did not think they had had contact with someone with symptoms, so it is assumed that just over 50% of the sample had been self-isolated, although they had not recently experienced danger. At least 35% of people who have self-isolated have adopted proper hygiene measures, together with 29% of those who have not self-isolated. Regardless of whether they have self-isolated, 32% doubt they are complying with the hygiene regulations adequately or are not complying with them at all (2.3%). As for social relations, the 47% who did not self-isolate thought that no-one from their nuclear family had had risky contacts, as did 46% of those who did self-isolate. A total of 1.5% knew that a relative had symptoms while the remaining 4.7% were unsure. Regarding extended families, 43% of those who did not self-isolate reported that they were not infected, followed by 45% who did self-isolate, who did not report contagion. A total of 8.6% were unsure whether their extended family had been infected regardless of their self-isolation, while the remaining 2.7% did know their extended family had been infected.
Regarding social relationships or those not belonging to the family nucleus, the 41% who did not self-isolate said that members of their closest social circle were not infected, as did the 40% who self-isolated. Twelve per cent were unsure whether they had been infected and 5.4% were sure that their close relatives had been infected. For distant (or extended) family relationships, a somewhat different picture emerged. Of those who had self-isolated, 36% knew someone who had been infected, 4.3% reported that they did not, and 10.1% were unsure. At the same time, of those who did not self-isolate, only 3.13% knew that their extended contacts had been infected, while the remaining 35.6% thought that none of their extended family members had been infected, while 20.7% were not unsure, regardless of whether they had self-isolated. Finally, of those who self-isolated, 78% thought that their actions were important to prevent infection, 12.5% believed they had no impact, and the remaining 7.4% were unsure. Of the participants who did not self-isolate, 36% thought that their actions had an impact against the pandemic, 10.19% were unsure, and only 3.1% thought that they did not.
In relation to the risk and worry score (Figure 1), there seems to be a very weak (.1) insignificant association, meaning that it can be assumed that worry is an independent phenomenon from self-isolation for this sample, perhaps due to the fact of its premature launching on March 22, when the order to self-isolate was issued. On the other hand, this probably indicates that high levels of worry act as as trigger for the predictions of the risk of onset of anxiety, depression, and stress that professionals think could emerge (Unidad de difusión del INPRFM, 2020).
As for groups findings, the following was observed. In the gender comparison, a significant difference was observed. The overlap coefficient indicated that at least 24% of the observations had different responses. Nevertheless, before assuming that this is an important effect, it should be recalled that the sample is uneven, given that the group comprised almost twice as many women as men. However, one should recall that it has been reported that women tend to score higher than men in terms of worry (Robichaud, Dugas, & Conway, 2003; Stewart, Taylor, & Baker, 1997). Perhaps future research, while the pandemic lasts, may change these figures. However, for this sample it was observed that women score higher on the worry indexes by at least six points. A similar thing occurs with occupational demandingness. The group with high occupational demandingness is twice as large as the group with low occupational demands. However, calculating the size of the effect does not predict a scenario that will change regardless of the n since the answers in the two groups only differ by 8% in this sample.
Regarding educational attainment, although this is a group that can be easily compared due to the number of members, the latter decreased considerably since most of the sample (66%) had a university education. Nevertheless, its overlap coefficient does not look promising either in increasing an n since, in the same way as in occupational requirement and isolation, answers only differ by 8%. The comparison that is most reliable both because of its well-matched number of members and its statistical power is self-isolation, since this apparently did not yield a different effect in the face of the pandemic, although it is important to note that the instrument is out of context, in other words, it does not focus directly on worry about the pandemic but rather about everyday life, so, to a certain extent, it makes it possible to detect a premorbid condition that may become exacerbated as the pandemic progresses due to the harmful effects it has on mental health (Caplan, 2007; Hirsch & Mathews, 2012; Lauder et al., 2004).
Although we are still at the early stages of the pandemic, it is possible to observe that 40% of our sample may be vulnerable. Although this vulnerability will depend on psychosocial factors such as overcrowding, the economy, interpersonal relationships, and premorbid status, data suggest that, in a pessimistic scenario, mental health services will be saturated since there is usually not as much demand in natural conditions. At this time, it is crucial for information on the latest findings of the disease to be shared with the public in such a way as to leave little room for uncertainty. It is considered necessary for public health authorities to update their messages to motivate and encourage people to adopt preventive measures more effectively, build trust and avoid misconceptions. If they have adequate access to information, this could significantly prevent people vulnerable to anxiety from developing symptoms.
Appropriate, effective, and rapid information is a means of counteracting the negative psychological effects of quarantine. It is essential for people to understand the situation and to provide them with the necessary supplies. They should be politically encouraged to altruistically choose quarantine to avoid the perception of imposition and restriction of freedom, and to implement preventive mental health measures to cope with future mental disorders. The practice of remotely organized activities could serve as mitigating measures and reduce the likelihood of the psychological costs of COVID-19 quarantine becoming permanent.

