











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Self-efficacy is a psychological construct understood as one’s belief in one’s ability to execute a specific behavior (Bandura, 1982, 1993, 2001). Self-efficacy is closely linked to mental health. It is associated with well-being, perceived stress, socialization, performance, optimism, self-control, self-esteem, depression, and anxiety. It has been found that self-efficacy determines changes in the lifestyles of people with chronic illnesses (Bonsaksen, Fagermoen, & Lerdal, 2014; Bonsaksen, Lerdal, & Fagermoen, 2012). Healthy eating is understood as the diet required to achieve a healthy caloric balance and weight. It is recommended to reduce the intake of fats, sugar, and sodium, and to increase the consumption of fruit, vegetables, pulses, whole grains, nuts, and water (Organización Mundial de la Salud, 2013). The main treatment for people with obesity is the adoption of this healthy diet, which involves a series of cognitive processes to adhere to this behavior. The Health Action Process Approach (HAPA) has proven that self-efficacy is a construct that explains a large part of the variance in various domains of behaviors associated with healthy lifestyles, such as physical exercise and diet (Anderson, Winett, & Wojcik, 2000, 2007; Delahanty et al., 2013; Kreausukon, Gellert, Lippke, & Schwarzer, 2012; Luszczynska, Gutiérrez‐Doña, & Schwarzer, 2005a; Motl et al., 2002; Parschau et al., 2013; Renner et al., 2008; Scholz, Sniehotta, & Schwarzer, 2005).
The HAPA model helps to understand the process of adopting a healthy diet. Figure 1 distinguishes two phases in the processes of behavioral changes. The first phase is a motivational one, in which intentions are formed to initiate a behavior and the second, called volitional, consists of the process of formation of the new behavior (Schwarzer, 2008). In the motivational phase, the advantages and disadvantages of behavioral change are analyzed, together with the damage and adverse consequences habits have had on health, as well as the possible outcomes of behavioral change, such as success or failure. When people expect positive results in this change of lifestyle, it increases the intention and likelihood of changing behavior. Moreover, confidence in one’s own abilities to achieve the desired goal is essential (Luszczynska et al., 2005a; Schwarzer & Gutiérrez-Doña, 2009).
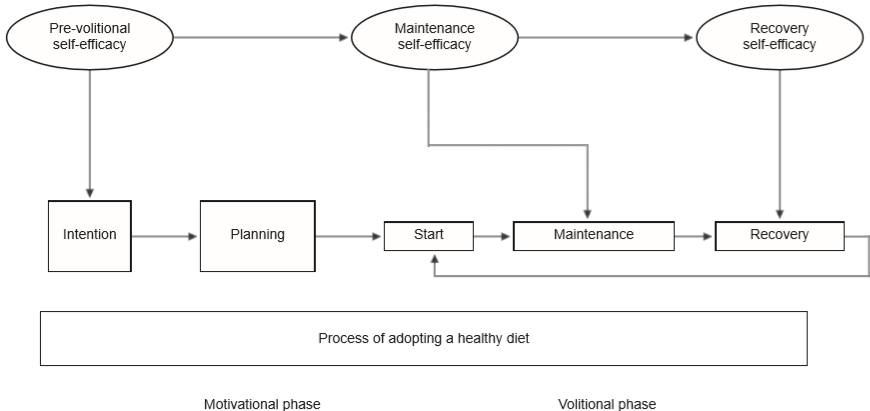
The volitional phase determines whether intentions will be achieved. Regulatory skills and strategies are required, which consist of detailed plans on how, when, and where behavioral changes will take place. Moreover, strategies are required to cope with the difficulties in achieving the desired results and whether one’s initial expectations have been met. This phase is crucial to maintaining healthy behaviors, because the ability to recover from relapses is tested (Luszczynska et al., 2005a; Schwarzer, 2008; Schwarzer & Gutiérrez-Doña, 2009).
According to the HAPA model, there are three types of self-efficacy, one which operates in the motivational phase and two in the volitional phase: a) self-efficacy in actions or pre-volitional refers to an optimistic belief about the results of one’s behavior; individuals with a high level in this component imagine success and are more likely to start a new behavior; b) maintenance self-efficacy is the optimistic belief in one being able to cope with the problems that arise when the actions have begun. Individuals with a higher level of this factor will invest more effort in maintaining the behavior despite the difficulties and barriers that occur; c) self-efficacy in relapse recovery is the conviction that one will be able to continue with the plans drawn up, regain control of the situation and minimize the risks arising from relapses. (Renner et al., 2008; Schwarzer, 2008; Schwarzer & Gutiérrez-Doña, 2009).
In recent decades, several instruments have been constructed to measure self-efficacy, usually on the basis of the General Self-Efficacy Scale (Luszczynska, Scholz, & Schwarzer, 2005b). The instruments have been developed for each specific behavior, such as The Self-Efficacy for Managing Chronic Disease Scale (Ritter & Lorig, 2014), and the Nutrition Self-Efficacy Scale/ Exercise Self-Efficacy Scale (Schwarzer & Renner, 2005). In Mexico, the following instruments are applied Self-Efficacy for Physical Activity in School-age Children (Aedo & Ávila, 2009), Self-Efficacy for Engaging in Healthy Behaviors in Healthy Children (Flores León, González-Celis Rangel, & Valencia Ortíz, 2010), and the Inventory of Perceived Self-Efficacy for Weight Control Adapted for the Mexican School Population (Saldaña, Peresmitré, Meraz, & del Castillo Arreola, 2011). These instruments are difficult to use in the population of interest because they are mainly designed for children in a school context. At present, there is no instrument in Mexico for measuring self-efficacy for an adult diet based on the HAPA model (Luszczynska et al., 2005b; Scholz, Nagy, Göhner, Luszczynska, & Kliegel, 2009; Schwarzer & Renner, 2005).
Developing an instrument that makes a conceptual distinction between various self-efficacies is extremely useful in health behavior research since it allows one to focus on the type of self-efficacy that must be reinforced at each stage of the change, particularly because of its impact on the formation of intentions, maintenance, and recovery from relapses. It has been shown that self-efficacy in actions is the best predictor of intentions, whereas self-efficacy in maintenance is the best predictor of behavior (Schwarzer, 2008; Schwarzer & Gutiérrez-Doña, 2009). Previous studies have found a significant association between self-efficacy in actions and maintenance and scores and the adoption of healthy foods (Hromi-Fiedler et al., 2016; Zhang et al., 2018; Zhou, Gan, Knoll, & Schwarzer, 2013). The higher the score in these two types of self-efficacy, the greater the decrease in body weight (Hattar, Pal, & Hagger, 2016). Self-efficacy in relapse recovery is related to both the intention of making changes in behavior and to an increase in physical exercise in people with obesity (Luszczynska et al., 2005a; Schwarzer & Gutiérrez-Doña, 2009).
Method
Study design
This is a descriptive, analytical, multicenter cross-sectional study with a convenience sample design, which considers the recommendations previously established in the literature of having at least 200 participants (Lloret-Segura, Ferreres-Traver, Hernández-Baeza, & Tomás-Marco, 2014; MacCallum, Widaman, Zhang, & Hong, 1999).
Sites
Participating patients were recruited from three public sector clinics in the metropolitan area of the Valley of Mexico, which offer specialized treatment programs to lose body weight; these consist of diet modification, general recommendations for physical exercise, and medical supervision.
Participants
The inclusion criteria for participants were men and women aged 18 to 65 years, with a Body Mass Index (BMI) ≥ 30, who were seeking nutritional treatment to reduce body weight and were able to read and write. The exclusion criteria were being candidates for bariatric surgery and attending treatment as a requirement for a surgical operation.
Development of the instrument
The construction of the SSHD was based on the Schwarzer Nutrition Self-Efficacy Scale (Schwarzer & Renner, 2005) with five items with four response options. The authors reported a good Cronbach’s alpha internal consistency of .87 (n = 1 726) and a r = .59 in the test-retest test (n = 982). This scale has been developed and tested on various samples (Gutiérrez-Doña, Lippke, Renner, Kwon, & Schwarzer, 2009; Renner et al., 2008; Schwarzer, 2008). To this end, the following steps were taken:
A bank of 60 statements was constructed to encompass the dimensions of the HAPA model (Luszczynska et al., 2005b; Scholz et al., 2009; Schwarzer & Gutiérrez-Doña, 2009; Zhou et al., 2013): pre-volitional self-efficacy (18 items), maintenance self-efficacy (22 items), and self-efficacy for relapse recovery (20 items).
The qualitative technique of cognitive laboratories was used (Johnstone, Bottsford-Miller, & Thompson, 2006; Zucker, Sassman, & Case, 2004) to culturally adapt the statements and make them understandable for the Mexican population. The participants were people with obesity who had been in treatment to reduce body weight, male and female with an age range of 24 to 60 years, whose educational attainment ranged from middle school to undergraduate degree level. Based on their feedback, sentences or words that were not understood were modified.
An evaluation was conducted by judges to obtain the validity of the content of the instrument. Judges were chosen based on the criteria of: (a) experience in making judgments and decision-making based on evidence or expertise (such as degrees, research, publications, position, experience, and awards), (b) reputation in the community, (c) availability and motivation to participate, (d) impartiality and inherent qualities such as self-confidence and adaptability (Skjong & Wentworth, 2000). The judges numerically rated each of the 60 items on a scale of one to four, in addition to making suggestions about the wording of the items, which were then modified. Items that obtained a degree of agreement of less than 80% were eliminated, in other words, those that obtained an average of less than 3.5 of all the judges’ evaluations (Appendix 1)
Measurements
The instrument applied to the sample was made up by 45 Likert items comprising the SSHD, with three dimensions of self-efficacy: pre-volitional, maintenance, and relapse recovery. Each dimension contains 15 items. Each item contains six response options ranging from Totally Agree to Totally Disagree.
Procedure
The SSHD was applied to 300 participants, on the assumption that 30% of the applications might have missing data. Patients who were at different stages of treatment were included and a database with 202 questionnaires was developed.
Construct validity was tested by exploratory factor analysis (EFA).
Items showing collinearity were eliminated, based on modification indices and ensuring that the item removed did not affect the measurement of an important dimension of the construct according to the theory.
Lastly, a confirmatory factor analysis (CFA) was performed.
Statistical analysis
Descriptive statistics were used for the analysis of sociodemographic data. An exploratory factor analysis (EFA) was applied to find a model with a good fit and contrast it with the theoretical proposal of the Health Actions Process Approach. This analysis was performed with SPSS 23. The method employed was Main Components with VARIMAX rotation, and the significant contribution criterion of more than .4 was used to consider that the item corresponded to a factor. To confirm the structure obtained by the EFA, a confirmatory factor analysis (CFA) was performed. Because the data set failed to meet the assumption of multivariate normality, the maximum likelihood estimation with robust standard errors and a mean and variance adjusted test statistic (MLMV) was used. Since the estimator uses scaling measures, the goodness of fit measures considered were Satorra and Bentler’s chi-square (χ2S-B), the scaled comparative adjustment index (CFIS ≥ .95), and the Root Mean Square Error of Approximation (RMSEAS ≤ .05). The regression coefficients, standard errors, and statistical significance for each parameter estimated in the model are given. In addition, the internal consistency of each factor and of the total scale was evaluated with the coefficient of reliability of the compounds (ω). To this end, the recommendations established in the literature were used (Raykov & Marcoulides, 2011). The CFA and the estimation of the reliability coefficients were carried out using Mplus 8 software.
Results
Participants had a BMI > 30 (range 30 to 42) and an average age of M = 46.3 (SD = 11.9) with a range of 27 to 65 years. Table 1 describes the sociodemographic characteristics of the sample.
Table 1 Characteristics of participants
| n | % | |
|---|---|---|
| Sex | ||
| Men | 57 | 28.2 |
| Women | 145 | 72.8 |
| Occupation | ||
| Housewife | 76 | 37.6 |
| Employee | 52 | 25.7 |
| Shopkeeper | 34 | 16.8 |
| Other | 40 | 19.9 |
| Educational attainment | ||
| Did not answer | 26 | 12.9 |
| Elementary | 9 | 4.5 |
| Middle school | 71 | 35.1 |
| High school | 47 | 23.3 |
| Technical degree | 27 | 13.4 |
| University | 19 | 9.4 |
| Master’s degree | 3 | 1.5 |
| x̄ | SD | |
| Age | 46.3 | 11.9 |
Exploratory factor analysis
Forty-five items were analyzed, yielding a three-component solution that explains 41.1% of the variance. Table 2 reports the 27 items with factor loads of over .40, while items 2, 8, 13, 15, 16, 17, 18, 19, 20, 22, 25, 26, 29, 31, 32, 33, 38, and 42 had a lower load. Component 1, labeled “Pre-volitional Self-efficacy (PS),” grouped together 10 items corresponding to the belief in one’s capacity to initiate behaviors related to healthy eating. Component 2, called “Maintenance self-efficacy (MS),” grouped together eight items that measured the belief in the ability to maintain a healthy diet, even when barriers or difficulties began to be observed. Lastly, component 3, called “Self-efficacy for relapse recovery (SRR),” included nine items measuring beliefs in the ability to resume healthy eating following a suspension or relapse.
Table 2 Factor loads obtained in the exploratory analysis for the solution of three factors
| Factor | |||
|---|---|---|---|
| Item | 1 | 2 | 3 |
| 37 | .65 | .03 | .21 |
| 34 | .60 | .12 | .24 |
| 10 | .60 | .01 | .16 |
| 36 | .59 | .22 | .33 |
| 6 | .56 | .14 | .18 |
| 3 | .55 | .13 | .24 |
| 1 | .54 | .16 | .09 |
| 21 | .53 | .12 | .07 |
| 25 | .52 | -.12 | .07 |
| 9 | .52 | -.05 | .12 |
| 45 | .05 | .91 | -.05 |
| 41 | .07 | .69 | .09 |
| 39 | .15 | .66 | .08 |
| 40 | -.09 | .59 | .04 |
| 44 | .07 | .58 | .21 |
| 24 | .08 | .57 | -.02 |
| 28 | -.02 | .54 | -.04 |
| 43 | .17 | .54 | .14 |
| 23 | .02 | .48 | .32 |
| 35 | .23 | .40 | .31 |
| 14 | .12 | .14 | .75 |
| 11 | .22 | .01 | .73 |
| 7 | .19 | .02 | .69 |
| 5 | .18 | .29 | .64 |
| 12 | .24 | -.03 | .53 |
| 27 | .37 | .10 | .51 |
| 4 | .11 | .22 | .50 |
| 30 | .34 | -.02 | .47 |
| Eigen Values | 3.85 | 4.04 | 3.63 |
Confirmatory factor analysis
The CFA tested the 27 items with a factor load of at least .40. Items with high modification rates were eliminated following the recommendations to avoid collinearity (Byrne, 2010) and taking into account their theoretical importance (Kline, 2011).
The following items were eliminated: factor one 37, 34, 25, 21, 9, and 1, factor two 44, 43, 41, 35, 28, and 23, factor three 27, 14, 7, 5, and 4.
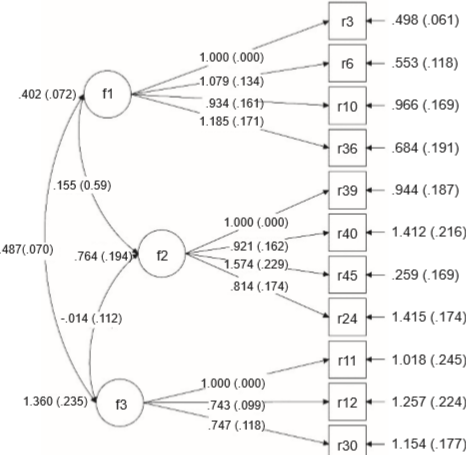
After evaluating the model, the following measures of goodness of fit χ2 = 66.49, p < .001, and χ2 S-B/gl = 41 were obtained. CFIS = .955, NFI = .893, RMSEAS = .056 (95% CI [.029, .079]). The coefficients, standard errors and z values of the items comprising the final version of the CFA are shown in Figure 2 . Factor one comprised items 3, 6, 10, and 36; factor two items 24, 39, 40, and 45; and factor three items 11, 12 and 30. As regards internal consistency, the reliability coefficients of the compounds were: AP ω = .724 (CI 95% [.655, .793]); AM ω = .779 (CI 95% [.655, .793]); ARR ω = .711 (CI 95% [.628, .794]); total scale ω = .896 (CI 95% [.876, .915]).
Discussion and conclusion
Measuring self-efficacy in the population with obesity poses a challenge for research. The development of this scale was based on the need to measure self-efficacy as regards diet in a population with obesity. Schwarzer’s Self-efficacy Scale for Nutrition (Schwarzer & Renner, 2005), which we used as a base, contains five items. We consider that we could cover other aspects of self-efficacy by increasing the number of items for each dimension of the construct. These include the perception of support from one’s partner or family, criticism for being on a diet, the time and money spent preparing food, frustration in response to unsuccessful attempts, and being able to resist non-nutritious foods in poorly-controlled environments such as parties, etc.
The evaluation of psychological constructs during the initial, maintenance, and recovery from relapses stages requires the use of instruments that consider the sociocultural context. It was therefore necessary to consider the way patients understand the construct of self-efficacy and not only the definition. Accordingly, time and resources were spent on constructing statements that were clear enough to assess the patient’s beliefs in their own abilities in relation to healthy eating, the axis of treatment for reducing body weight. Although the HAPA model (Schwarzer & Gutiérrez-Doña, 2009; Schwarzer & Renner, 2005) has been translated into Spanish and used in the Latino population, as a result of analyzing the items it contains, we consider that the Spanish translation is insufficient. Mexicans may observe different barriers and obstacles from the populations that have been researched. Another reason for creating a new instrument was that some studies used four and seven response options interchangeably. In short, we believe we could obtain greater validity by systematically conducting the development of the instrument (based on the HAPA model) from preparing the items to obtaining psychometric properties. To this end, cognitive laboratories were conducted to adapt it culturally. Content validity was obtained through expert judges, and construct validity through EFA and CFA to obtain the Self-efficacy Scale for a Healthy Diet (SSHD). The results obtained show a three-factor SSHD model with an adequate fit.
The factor structure of the SSHD coincides with the three types of self-efficacy proposed by the Health Actions Process Approach (Schwarzer, 2008; Schwarzer & Gutiérrez-Doña, 2009; Schwarzer et al., 2007). The first factor, called “Prevolitional Self-efficacy,” is very important for beginning the changes in the diet required to reduce body weight in obesity treatment. This type of self-efficacy is the best predictor of the intention to make a change in one’s diet (Anderson et al., 2000; Anderson, Konz, Frederich, & Wood, 2001; Delahanty et al., 2013). Accurately measuring this construct makes it possible to distinguish between people who are prepared to begin treatment from those who need to develop their intention and increase their self-efficacy. The second factor is called “Self-efficacy for relapse recovery.” It has been found that people who consider relapses a total failure are less likely to continue treatment, unlike those who perceive themselves as capable of recovering. The third factor was called “Maintenance Self-efficacy.” Once people begin treatment, it is important that they feel effective in overcoming the barriers and difficulties that come along with changes in food.
It was found that factors two and three are correlated, as observed in the results, while the third factor only comprised three items corresponding to maintenance self-efficacy. This may be because once people start a healthy diet, they perceive relapses as part of the barriers to maintaining behavioral change rather than an independent difficulty. Recent studies have found that this type of self-efficacy predicts positive results in weight loss. Measurement of this factor is essential, once actions have been initiated, since individuals with a higher level of perceived self-efficacy will persist more and invest more effort in maintaining the new behavior (Schwarzer, 2008; Schwarzer & Gutiérrez-Doña, 2009; Schwarzer & Renner, 2005).
Limitations of the study include the fact that it is a non-probabilistic sample, which makes it impossible to generalize the results obtained through the sample to the population from which it was extracted, and the fact that data collection was based on self-reporting. An additional limitation is related to the use of the same sample to perform EFA and CFA, even though this is a practice used in similar studies. This makes it impossible to determine whether the resulting model is strictly generalizable within the population or to other populations.
Although several articles on self-efficacy scales based on the HAPA model show internal consistency data (Luszczynska et al., 2005b; Schwarzer & Gutiérrez-Doña, 2009; Schwarzer & Renner, 2005), since no studies were found reporting the assessment of the factor structure of the instruments they use, the findings of this research contribute empirical evidence to the HAPA model. It is a Spanish instrument, based on this model, which measures the three types of self-efficacy and has confirmatory factor analysis.
SSHD could be useful for evaluating the self-efficacy of people with obesity who begin treatment to reduce body weight, since self-efficacy is related to changes in diet such as the consumption of fruits and vegetables (Hromi-Fiedler et al., 2016; Zhou et al., 2013). High scores increase the chances of success in treatment, in addition to the fact that the instrument could provide important information for focusing psychological interventions on this group of patients, since if they have low self-efficacy, they have a high probability of dropping out of treatment or being unsuccessful in their attempts to lose weight.

