











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Chronic kidney disease (CKD) negatively impacts patients’ lives in various spheres (social, economic, psychological, work, and in the family nucleus) (Cukor, Cohen, Peterson, & Kimmel, 2007). These psychopathologies are most common in patients with CKD in hemodialysis-based substitute treatment, and impact their morbi-mortality (Cukor, Coplan, Brown, Friedman et al., 2008; Cukor, Rosenthal, Jindal, Brown, & Kimmel, 2009).
Resilience is defined as a person’s ability to develop healthily and successfully, despite being exposed to situations that jeopardize his/her integrity (Cukor et al., 2009). When resilience is seen from this positive approach, it is possible to understand the close link between health psychosocial adaptation and successful recovery from adverse experiences (Cabanyes Truffino, 2010), particularly illness, due to the presence of protective factors learned in childhood (Rodriguez-Piaggio, 2009). Resilience makes it easier for patients to perceive a low degree of physical interference and improve their future health perspectives, since they remain more optimistic, stave off illness, and perceive more control over their behavior and emotional states, which in turn encourages their treatment adherence and improves their overall quality of life (Vinaccia & Quiceno, 2011). Conversely, various sustained, unresolved psychosocial stressors in kidney patients may be associated with low resistance or allostatic burden, when applied to health and illness settings, particularly CKD (Cukor et al., 2007). For example, it is known that the time of diagnosis of an illness is inversely related to resilience (Quiceno & Vinaccia, 2012), and that depression and anxiety symptoms are associated with certain distorted thoughts in patients with CKD (Lerma, Salazar, Perez-Grovas, Bermudez et al., 2012). It is also know that modifying these distorted thoughts makes it possible to reduce depression and anxiety symptoms and improve the quality of life of these patients (Lerma, Perez-Grovas, Bermudez, Peralta-Pedrero, Robles-García et al., 2017). Multicultural studies of kidney patients point to the need to explore their resilient response from the context of their ethnic-family origin (White, Bichter, Koeckeritz, Lee, & Munch., 2002). In transplant situations, resilience is associated with aspects of positive or negative emotional adjustment, depending on patients’ perception of the disease (guilt, fear, gratitude, physical limitation, independence) (Schipper, Abma, Koops, Bakker et al., 2014), as well as social support, confidence, self-esteem, devaluation, and self-efficacy (Tong, Cheung, Nair, Kurella et al., 2014).
Against this background, it is important to be able to reliably measure resilience in this population with CKD, since it has been evaluated using questionnaires in Spanish in other non-Mexican populations (Vinaccia et al., 2011). There is also a questionnaire to evaluate resilience that has been validated in Mexican population as a whole (Palomar-Lever & Gómez-Valdéz, 2010), but there is no information to date on its validity or reliability in the specific context of patients in chronic hemodialysis.
Nor have researchers evaluated whether resilience factors in kidney patients are associated with depression or anxiety symptoms, or their distorted thoughts. Having a valid, reliable questionnaire to assess resilience in this population would make it possible to identify the relationship between resilience and the development of depression and anxiety and key clinical repercussions (such as morbidity, hospitalizations, and premature mortality). Likewise, a reliable evaluation instrument would make it possible to test the effects of potential therapeutic interventions that include resilience as a modifying variable that prevents or reduces the depression and anxiety symptoms of kidney patients.
The objective was to evaluate the validity and reliability of a psychological instrument to measure the resilience of Mexican patients diagnosed with chronic kidney disease under treatment with hemodialysis, and to evaluate the correlation between resilience factors and depression and anxiety symptoms and distorted thoughts.
Method
Participants
The study included a non-probabilistic sample of 280 patients with CKD in renal replacement therapy by hemodialysis for at least two months. They were aged between 18 and 85, of both sexes, with any etiology of their CKD or comorbidity (with the exception of any psychiatric disorder that was documented in their files or which had a prescription for psychiatric pharmacological treatment).
Location
The sample was obtained from six hemodialysis units in four states in Mexico: Mexico City (Comprehensive Renal Support, 19 = 6.8%, CEDIASA, 102 = 36.4%, Ignacio Chávez Instituto Nacional de Cardiología, 21 = 7.5%), León, Guanajuato, 68 = 24.3%; Mazatlán, 45 = 16.1%; Puerto Vallarta, 25 = 8.9%. Participants were recruited between March and August 2015 and the evaluation was undertaken between September and December 2015.
Instruments
Resilience was evaluated through a questionnaire incorporating items from two foreign instruments adapted and validated for the Mexican population (Palomar-Lever et al., 2010). The Mexican questionnaire included 43 items with a Likert-type scale measuring the following resilience factors: strength and self-confidence, social competence, family support, social support, and structure. Two hundred and seventeen members of the general public participated in the Mexican validation of the resilience questionnaire, which obtained a Cronbach’s alfa of .936. Depression and anxiety symptoms were evaluated using Beck’s Depression Inventory (BDI) and Beck’s Anxiety Inventory (BAI), which included 21 items each to measure somatic and cognitive anxiety and depression symptoms respectively (Beck, Epstein, Brown, & Steer, 1988; Beck, 2006), both instruments having previously been validated in the Mexican population (Beck et al., 1988; Robles, Varela, Jurado, & Páez, 2001; Torres-Castillo, Hernández-Malpica, & Ortega-Soto, 2012). Distorted thoughts were evaluated using a 30-item instrument developed for patients with CKD (Lerma et al., 2012), which comprises four factors: catastrophism, dichotomous thinking, intrinsic perfectionism, extrinsic perfectionism, and negative self-labeling. In a sample of 255 patients with CKD, the following Cronbach’s alpha were obtained: .92 for BDI, .92 for BAI, & .936 for the distorted thoughts instrument (Lerma et al., 2012; Lerma et al., 2017).
Procedures
The clinical data and demographic information of each patient selected to participate in the study were identified and the psychological instruments delivered. Each patient was shown how to answer the self-administered questionnaires and care was taken to ensure they had understood and answered each of the questions. In the case of patients who were unable to read and write or who had some form of visual or motor disability, the survey implementer read the items in the instrument and noted the respondent’s answers. The material obtained was then submitted to the principal investigator of the project for analysis.
Statistical analysis
Validation of the scale was carried out through an exploratory factor analysis (EFA) with the following steps: (i) compare the discrimination capacity of each item using the Student’s t-test, (ii) evaluate the directionality of the items by cross-tables, (iii) evaluate internal reliability using Cronbach’s alpha, (iv) identify factors through factor analysis using the Varimax method, (v) determine the usefulness of the structure of the components by means of the sample adequacy index and the Bartlett sphericity test.
Next, a confirmatory factorial analysis (CFA) of the first order was carried out using the maximum likelihood (ML) method, which assumed a multifactorial model with five domains or latent factors with covariance among the measurement errors. The following procedures suggested by Byrne were used to estimate the structural equations model (Byrne, 2010); AMOS 23 program was used (IBM-SPSS, USA) (Arbuckle, 2012). Several indices were estimated: X2 (CMIN) and the ratio of X2/degrees of freedom (CMIN/gl) as measures of parsimony; the Goodness of Fit Index (GFI) and its complements; the Adjusted Goodness of Fit Index (AGFI) and the Tucker-Lewis Index (TLI) and the Comparative Goodness of Fit Index (CFI), which is a better indicator for samples of over 200 (Byrne, 2010; Ullman, 2006); and the Root Mean Square Error of Approximation (RMSEA).
Finally, the association between resilience factors and depression and anxiety symptoms and distorted thoughts was evaluated by calculating Pearson’s correlation. The statistical analysis was undertaken using SPSS 15.0. A value of p < .05 was considered significant.
Results
The study included 280 patients who had been in hemodialysis for some time (median [25th - 75th percentile]) = 33 (16 - 50) months. Patients were aged between 18 and 85, 40% of whom had diabetes mellitus. The main occupations were: retired or unemployed (33%), housewife (28%), or employee (17%). Educational attainment was as follows: secondary (66%), basic (21%), and university (11%) education. The respondents’ marital status was as follows: 39% lived alone (single, widowed, divorced), while 61% are partnered (married or living with their partners).
Exploratory analysis
All the items showed a capacity for discrimination (Student’s t test, p < .001). The survey implementers checked that there were no empty boxes and the corresponding directionality of the data in the cross tables for each item. Table 1 shows the result of the factor analysis. Out of the original questionnaire with 43 items, items 19 (“When I’m not well, I know things will improve”) and 29 (“I enjoy being with my family”) were eliminated because they duplicated more than one factor. Five factors were obtained: strength and self-confidence (18 items), social competence (8 items), family support (5 items), social support (5 items), and structure (5 items). All the items had factor loads between .547 and .838.
Table 1. Distribution of resilience items in 280 patients with chronic kidney disease in hemodialysis treatment Results of factor analysis with orthogonal rotation. The numbers represent the factorial load
| Factors | |||||
|---|---|---|---|---|---|
| Items | SSC | SC | FS | SS | STR |
| Factor 1 - Strength and self-confidence | |||||
| 3 I am a strong person. | .727 | .209 | .082 | .197 | .159 |
| 11 I think I will be successful. | .715 | .217 | .239 | .013 | .208 |
| 14 My future looks good. | .673 | .189 | .293 | -.056 | .179 |
| 8 I am proud of my achievements. | .672 | .245 | .143 | .258 | -.003 |
| 12 I know how to achieve my goals. | .655 | .123 | .202 | .124 | .292 |
| 7 I strive to achieve my goals. | .650 | .114 | .257 | .196 | .236 |
| 10 Believing in myself helps me overcome difficult moments. | .632 | .301 | .210 | .253 | .016 |
| 16 I’m satisfied with myself. | .622 | .326 | .177 | .028 | .110 |
| 1 What has happened to me in the past makes me feel confident I will be able to cope with new challenges. | .612 | .190 | -.005 | .027 | .233 |
| 13 Whatever happens, I will always find a solution. | .598 | .207 | .084 | .226 | .153 |
| 5 I have control of my life. | .596 | .272 | .170 | .273 | .193 |
| 4 I know very well what I want. | .593 | .372 | .084 | .234 | .174 |
| 2 I know where to seek help. | .588 | .241 | -.069 | .060 | .165 |
| 9 I know I have skills. | .588 | .261 | .129 | .139 | .193 |
| 6 I like challenges. | .569 | .208 | .162 | .250 | .311 |
| 15 I know I can solve my personal problems. | .566 | .256 | .210 | .119 | .186 |
| 18 I trust my decisions. | .564 | .350 | .157 | .145 | .312 |
| 17 I have realistic plans for the future. | .547 | .128 | .244 | -.123 | .374 |
| Factor 2 - Social competence | |||||
| 21 It is easy for me to establish contact with other people. | .211 | .838 | .150 | .023 | .057 |
| 22 It’s easy for me to make new friends. | .287 | .798 | .125 | -.023 | .141 |
| 20 I feel comfortable with other people. | .240 | .779 | .018 | .045 | .094 |
| 23 It’s easy for me to have good conversation topics. | .217 | .767 | .048 | .130 | .143 |
| 26 I enjoy being with other people. | .334 | .708 | .126 | .172 | .094 |
| 27 I know how to start a conversation. | .295 | .701 | .164 | .222 | .152 |
| 24 I easily adapt to new situations. | .334 | .697 | .169 | .059 | .266 |
| 25 It’s easy for me to make other people laugh. | .327 | .635 | .115 | .173 | .110 |
| Factor 3 - Family support | |||||
| 30 In our family we are loyal to each other. | .100 | .118 | .831 | .193 | .158 |
| 31 In our family we enjoy doing activities together. | .142 | .198 | .777 | .285 | .166 |
| 28 I have a good relationship with my family. | .261 | .166 | .758 | .259 | .023 |
| 33 In our family we agree on what we consider important in life. | .194 | .094 | .709 | .341 | .233 |
| 32 Even in difficult times, our family has an optimistic attitude towards the future. | .320 | .162 | .603 | .290 | .129 |
| Factor 4 - Social support | |||||
| 34 I have friends /relatives who really care about me. | .143 | .119 | .357 | .814 | .079 |
| 35 I have friends / relatives who support me. | .218 | .076 | .337 | .802 | .076 |
| 36 I always have someone who can help me when I need it. | .189 | .171 | .199 | .798 | .081 |
| 37 I have friends / relatives who encourage me. | .102 | .140 | .311 | .735 | .294 |
| 38 I have friends / relatives who value my skills. | .218 | .091 | .356 | .727 | .229 |
| Factor 5 - Structure | |||||
| 41 I prefer to plan my activities. | .298 | .166 | .059 | .107 | .742 |
| 39 Rules and routine make my life easier. | .250 | .187 | .131 | .283 | .733 |
| 40 I maintain my routine even in difficult times. | .307 | .203 | .030 | .154 | .721 |
| 42 I work better when I have goals. | .349 | .063 | .217 | .007 | .641 |
| 43 I’m good at organizing my time. | .210 | .155 | .161 | .142 | .600 |
A summary of the reliability analysis by factors is shown in Table 2 . The final instrument with 41 items had an overall internal consistency (Cronbach’s alpha) of .96, accounting for 63.6% of the total variance, while consistency by subscales ranged from .85 to .95, with an overall average of 134.90 ± 19.45. Bartlett’s sphericity test yielded a value of 9208.06 (p ≤ .001) indicating non-identity of the correlation matrix, while the Kaiser-Meyer-Olkin index (.942) indicated sampling adequacy, because it is close to 1.
Table 2. Variance, means and Cronbach’s alpha coefficients of the final version of the instrument (n = 280)
| Factors | Number of items | Explained variance | Mean | Variance | Cronbach’s alpha |
|---|---|---|---|---|---|
| n = 41 | 63.6% | 134.9 | 378.30 | .964 | |
| Strength and self-confidence | 18 | 20.34% | 58.50 | 91.90 | .945 |
| Social competence | 8 | 13.97% | 25.74 | 24.87 | .930 |
| Family support | 5 | 10.58% | 17.14 | 9.81 | .903 |
| Social support | 5 | 10.21% | 17.72 | 8.65 | .932 |
| Structure | 5 | 8.55% | 15.84 | 9.70 | .853 |
Confirmatory analysis
The fit of the five-factor model obtained through the exploratory analysis was evaluated through a confirmatory factor analysis (CFA) using the maximum likelihood method, with the following steps:
Identification of the model: For the model analyzed, there were 46 endogenous variables (41 involving measures and five involving structures) out of a total of 93 variables. There were 52 non-observed variables (total parameters to be estimated by the model), 46 of which were exogenous (41 measurement errors, five residual errors), out of a total of non-redundant elements of the matrix equal to 1081. Since the parameters to be estimated are clearly lower than the total number of non-redundant elements in the matrix, we can say that the model is over-identified and can be identified. Since there are no correlations between the residuals, it is a recursive model.
Specification of the model: Based on the exploratory analysis of reliability and the factor analysis previously presented, a model for Figure 1 was designed whereby the circumferences or ovals represent latent variables and the rectangles represent the observable variables. Measurement and residual errors are shown as smaller ovals.
Estimate of parameters: The AMOS program was asked to apply the maximum likelihood method, with standardized estimators, R2 estimator (multiple squared correlations), covariances of the estimators, indices to be modified and critical proportions for the differences.
For the evaluation of fit (the sample exceeds n = 200), as a first step, all the results were examined to ensure that the estimated coefficients did not exceed the acceptable limits (that there were no negative or insignificant error variances, standardized coefficients over 1, or excessively high standard errors related to an estimated coefficient). No collinearity was observed in the variables measured, since the correlations were less than .3 (Kline, 2005) or extreme or univariate or multivariate scores (George & Mailery, 2010). Moreover, excellent asymmetry was observed in all the variables (values not over ± 1.00), (± 10 points) except in the Family Support and Social Support variables, yet still within adequate parameters (Tabachnick & Fidell, 2001).
Table 3 shows that as regards the absolute measures of overall adjustment, the chi square value was 1755.32 (p = ≤ .001, 766 gl), while the chi square ratio and degrees of freedom (CMIN/DF = 2.29) is excellent, indicating that mistakes in the variances and covariances of the model are null and adjusted to samples of over 200 data as recommended by the experts (Byrne, 2010).
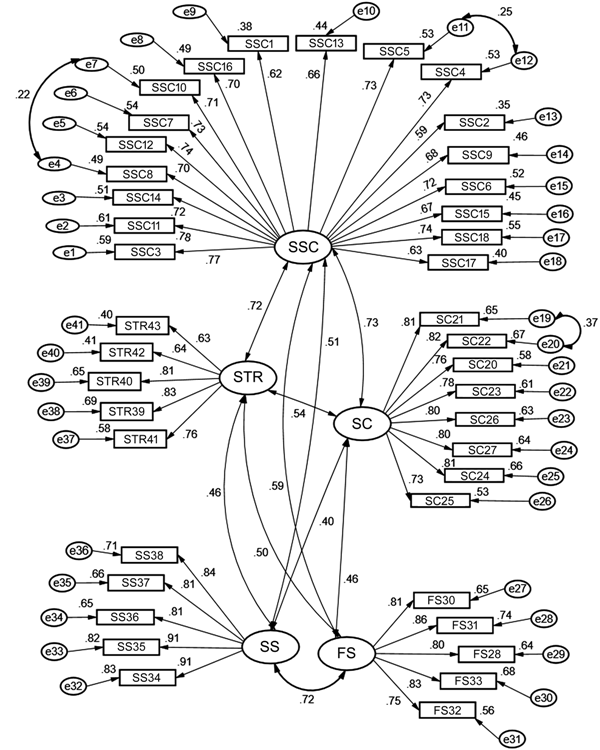
Figure 1. Confirmatory model of five resilience factors in Mexican kidney patients (n = 280). Chi square = 1755.32, 766 gl, p ≤ .001; CMIN/gl = 2.292; RMR = .031; GFI = .769; CFI = .881; RMSEA = .068 (.064 - .072).
Table 3. Goodness-of-fit indices of the confirmatory model resulting from 5 factors in kidney patients (n = 280)
| Statistics | Desirable criterion | Value in the present study | Interpretation |
|---|---|---|---|
| Absolute fit X2/gl (CMIN/gl) | Less than 2 or 3 | 1755.32/766 gl = 2.292 | The errors of the model are null with the |
| used and the absolute fit is excellent | |||
| Goodness of fit index (GFI) | > .90 Preferential > .95 | GFI = .769 | Good fit |
| Comparative goodness of fit index | > .90 Preferential > .95 | CFI = .881 | Acceptable comparative fit |
| (CFI) | |||
| Root Mean Square Residual (RMR) | Near zero | RMR = .031 | Model error close to zero, almost perfect fit |
| of model to data | |||
| Root mean square error of approx | Less than .08, close to zero | RMSEA = .068 (.064 - .072) | Model error close to zero, almost perfect fit |
| -imation | of model to data |
The comparative measures of global adjustment, and the comparative fit index (CFI), are very close to the ideal (CFI = .88), as is the Tucker-Lewis index, which takes into account the complexity of the model (TLI = .87), indicating an acceptable fit with the data, since at least 87% of the covariance in the data can be reproduced by the model (Byrne, 2010).
Since the parsimony indices (PCFI = .823) are very close to the optimal value (.900), the model can be described as complex ‒ (Hu & Bentler, 1998), as the goodness of fit statistics show to an acceptable extent (GFI = .769, AGFI = .740, PGFI = .684), in addition to the Root Mean Square Error of Approximation (RMSEA = .068, CI95% = .064 - .072), which penalizes the increase in the complexity of the model and indicates an excellent fit with the data, since it is less than .08 and is confirmed by the value in the Residual Mean Error (RMR = .031), since this fulfils the requirement of being below the threshold value, indicating nearly zero error and an almost perfect fit (less than .05) (Byrne, 2010).
Correlation of resilience with other psychological variables
The five factors correlated positively with each other, and negatively with anxiety and depression symptoms and distorted thoughts (Table 4). These correlations were significant (p < .05) between the total resilience score and the total and subscale scores of depression and anxiety symptoms and distorted thoughts. All resilience factors correlate with the cognitive and somatic subscales of depression and anxiety, and there was correlation between resilience factors and most of the distorted thoughts subscales.
Table 4. Correlation between dimensions of resilience and depression and anxiety symptoms and distorted thoughts (n = 280)
| Resilience factors | Total | |||||
|---|---|---|---|---|---|---|
| Psychological variables | SSC | SC | FS | SS | S | resilience |
| Social competence (SC) | .68** | |||||
| Family support (FS) | .60** | .39** | ||||
| Social support (SS) | .51** | .38** | .65** | |||
| Structure (S) | .68** | .47** | .47** | .44** | ||
| Total resilience | .94** | .78** | .74** | .67** | .75** | |
| Anxiety Symptoms | ||||||
| Total score | -.49** | -.45** | -.35** | -.31** | -.32** | -.51** |
| Somatic anxiety | -.50** | -.44** | -.32** | -.28** | -.33** | -.50** |
| Cognitive anxiety | -.41** | -.39** | -.35** | -.30** | -.23** | -.44** |
| Depression symptoms | ||||||
| Total score | -.58** | -.41** | -.42** | -.28** | -.40** | -.56** |
| Somatic depression | -.57** | -.40** | -.38** | -.26** | -.41** | -.55** |
| Cognitive depression | -.52** | -.38** | -.42** | -.26** | -.31** | -.51** |
| Distorted thoughts | ||||||
| Total score | -.37** | -.27** | -.28** | -.25** | -.20** | -.36** |
| Catastrophism | -.45** | -.33** | -.33** | -.27** | -.28** | -.43** |
| Dichotomous thinking | -.23** | -.15* | -.22** | -.16* | -.07 | -.22** |
| Intrinsic perfectionism | -.14* | -.06 | -.21** | -.16* | -.02 | -.15* |
| Extrinsic perfectionism | -.23** | -.14* | -.30** | -.22** | -.10 | -.24** |
| Perfectionism (Total score) | -.17** | -.09 | -.24** | -.20** | -.05 | -.18** |
| Negative self-labeling | -.25** | -.14* | -.24** | -.20** | -.09 | -.24** |
Notes: FS = Family support; SS = Social support; SC = Social competence; S = Structure; SSC = Strength and self-confidence;
*p <. 05 (bilateral),
**p < .001 (bilateral).
Discussion and conclusion
The results of this study show that the instrument evaluated is reliable and valid for measuring resilience in patients with CKD. This specific version retained 41 of the 43 original items, with the same number of original subscales, all associated with depression and anxiety symptoms as well as distorted thoughts. In the confirmatory analysis, a theoretical structural model was obtained, which acceptably fits the complexity of the data in this specific sample with kidney patients, according to the most important reliability indices shown and suggested by experts (Byrne, 2010; George et al., 2010; Hu & Bentler, 1998; Kline, 2005; Tabachnick et al., 2001). The model contains five factors with a strong association between them, as the exploratory analysis showed, which allows us to recommend this instrument to assess resilience in patients with chronic kidney insufficiency (CKI). The most powerful indicators of the fit of the model’s structure (CFI, RMR, and RMSEA) suggest that it is a balanced, parsimonious model (Ullman, 2006).
This adjusted version for measuring psychological resilience could be used to complement information on psychological aspects of kidney patients. The psychological vulnerability of these patients to the disease could be detected by the factorial components of the adapted resilience scale. In future studies, the clinical usefulness of resilience could be evaluated as part of new strategies to reduce dysfunctional behaviors (e.g., dropping out of treatments) and the negative physical (e.g., impaired health), mental (depression and anxiety) and social consequences (such as social abandonment and functional dependence).
This psychological instrument evaluates resilience in patients with CKD, which would enable new studies to understand, analyze, and explore how they use their internal and external resources to positively cope with illness, because some previous studies mainly focus on detecting the negative effects of the disease (Cukor et al., 2009; Dobrof, Dolinko, Lichtiger, Uribarri, & Epstein, 2002; Elliott, Gessert, Larson, & Russ, 2014; Ma, Chang, Liu, Hsieh et al., 2013; Nicholas, Picone, & Selkirk, 2011; Shidler, Peterson, & Kimmel, 1998; Tong et al., 2014; Wick, Bauer, Malessa, Settmacher, Strauss, 2015).
This study confirms the relationship between distorted thoughts and depression and anxiety symptoms (Lerma et al., 2012) and is now combined with the measurement of resilience in kidney patients. We regard these associations as empirical evidence that support the development of cognitive-behavioral strategies combined with these variables in order to impact psychological and clinical aspects in this population (Tong, Lesmana, Johnson, Wong et al., 2013). For example, the reliable quantitative evaluation of resilience in these patients would make it possible to evaluate the effectiveness of psychological interventions that include resilience to reduce depression, anxiety, and the presence of distorted thoughts, all of which reduce the quality of life (Cukor, 2007; Cukor et al., 2009; Shidler et al., 1998). Likewise, this validated instrument would make it possible to study the relationship between resilience and other variables such as family ethnicity (White et al., 2002), time of diagnosis (Quiceno & Vinaccia, 2012), perception of disease (Schipper et al., 2014), social support, devaluation, self-efficacy, and self-esteem (Tong et al., 2013) so that they can be explored in studies of diagnosis, prognosis, and psychological intervention.
Although the constructs of resilience and depression and anxiety belong to different theoretical models ‒with the former coming from a positive psychosocial approach (Cabanyes Truffino, 2010; Rodriguez-Piaggio, 2009; Vinaccia et al., 2011) which attempts to identify protective or risk elements or factors‒, whereas depression and anxiety are more closely linked to the medical risk model (Cukor et al., 2009; Ma et al., 2013; Wick et al., 2015) (for example, age, sex, education, negative attitudes, or perception of disease) ‒ the relationship found between them in our research suggests the need for new studies to explore and empirically test the mechanisms that explain this relationship from the point of view of their pertinence and clinical interest for measuring the quality of life in patients with CKD. The role of psychological resilience in these patients, as well as the impact it has on the emotional state and quality of life has barely been researched. The instrument validated in the present study could be used to evaluate whether low resilience in a population predisposes it to greater hypersensitivity and inadequate responses to the presence of adverse symptoms of the disease (Cukor et al., 2007; Cukor et al., 2009; Lerma et al., 2017; Shidler et al., 1998) (e.g., hypotension during hemodialysis).
As suggested by previous research (Miranda-Zapata, Riquelme-Mella, Cifuentes-Cid, & Riquelme-Bravo, 2014) our study was conducted with a multicentric sample of patients with CKD, from secondary and tertiary level hospitals (in kidney substitution treatment), which strengthens our confidence in the external validity of the scale used. However, more extensive, heterogeneous studies are required nationwide to increase the generalization of the results that will facilitate the construction of standardized scales of this instrument. The present study did not evaluate the associations between resilience and sociodemographic and clinical variables of patients, which is undoubtedly an important research topic. However, the evaluation of these associations goes beyond the scope of the objectives of this paper and future studies are required to address the issue comprehensively and sufficiently. Another limitation of the study is that it failed to evaluate the cognitive capacity of respondents, one of the factors that can be altered by disease or age. Lastly, the results of the validation, including the structural equations model obtained in the confirmatory analysis, are applicable to patients with CKD only. Other studies must be undertaken to evaluate this scale in patients with other chronic diseases (such as diabetes mellitus) where it is known that there is also high comorbidity of anxiety and depression symptoms.

