











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
The political and social awareness raising that has happened in the past 50 years about gender-based violence has allowed for the deployment of equality policies, and regional and state legislations, as well as the creation of entities responsible for promoting and guaranteeing the treatment of gender-based violence in different countries around the world.
In Spain, in line with the National Plan for Sensitization and Prevention of Gender-based Violence, contained in the Boletín Oficial del Estado (2004) , specialized work teams are responsible for organizing, designing, and executing interventions under the coordination of different intervention axes: justice, security, health, social services, and psychological intervention.
More than ten years after the implementation of these services, it is important to look back at the teams that work against violence because, in accordance with different studies, the professionals engaged in care for victims of violence could be vulnerable to the stress resulting from helping and caring for victims of traumatic events ( Arón & Llanos, 2004 ; Ojeda, 2006 ; Acinas, 2012 ; Izcurdia & Puhl, 2017 ; Gomà-Rodríguez, Cantera, & Pereira, 2018 ). According to Arón and Llanos (2004) , being exposed to a high level of work-related wear can cause severe psychological disorders and departure from the profession or the work area.
In the context of the workers engaged in care for gender-based violence, Izcurdia and Puhl (2017) refer to the complexity of roles and tasks that confront these professionals and their relationship with stress and spillover in professional practice. Their results conclude that burnout rates are high among the professionals working with these problems. In another study by Quiñones, Cantera, and Ojeda (2013) , the focus was on the reproduction of violence at the centers that work against gender-based violence. In the conclusions, the “effects of this violence” are referred to, mentioning physical symptoms, paralysis, and low self-esteem because of the workers’ professional activity.
The studies cited above ( Arón & Llanos, 2004 ; Ojeda, 2006 ; Acinas, 2012 ; Quiñones et al., 2013 ; Izcurdia & Puhl, 2017 ; Gomà-Rodríguez et al., 2018 ) try to raise awareness and give voice to the repercussions of working with these issues. Transferring this discomfort to institutions and achieving an in-depth understanding of the need for action is a very hard task, mainly due to the lack of resources in the sector and the professionals’ responsibility for their own health and well-being. To promote the well-being and health of these workers and achieve an appropriate care relationship, this scenario needs further visibility. This also implies taking urgent measures and making proposals that help these professionals to face the difficulties they suffer. Therefore, some authors ( Arón & Llanos, 2004 ; Ojeda, 2006 ; Santana & Farkas, 2007 ; Guerra, Guenzalida, & Hernández, 2009 ; Cantera & Cantera, 2014 ) propose the investigation and implementation of self-care in all of its dimensions. Self-care has been defined by Cantera and Cantera (2014) as “the development of skills for the management of emotions, which permit, in an active and conscious way, care in the first person while intervening to promote personal and collective well-being” (p.89). The function of self-care is to regulate the factors that affect individual development and activities for the benefit of life, health, or well-being ( Prado, González, Gómez, & Romero, 2014 ).
The general objective of this research is to grasp relevant concepts related to the health and self-care of professionals working in care for victims of gender-based violence. Therefore, this research aims to achieve three specific objectives: 1. describe and analyze the repercussions of working with victims of gender-based violence on health; 2. describe and analyze factors (personal, social, or institutional) that influence the occurrence of these physical or psychological repercussions on the professionals’ health; 3. describe and analyze the practices performed to prevent or solve these consequences.
Method
Design
This research has a qualitative, analytical, and exploratory design. Due to the recent creation of teams specialized in the treatment of gender-based violence in the Spanish context, references describing the professional reality and the health and self-care of these professional teams are scarce. Nevertheless, a framework of models and studies on the issue is fundamental as these shortcomings should not affect the health of the professionals working in the sector, which would contradictorily turn them into obstacles for the elimination of gender-based violence. The use of the qualitative method permits knowing the facts, processes, structures, and people in their totality and depth ( Mendoza, 2006 ). Therefore, it is considered a suitable method to capture and identify relevant phenomena in this field.
To achieve the objectives, a semi-structured interview was used; this involved a conversation between researcher/participant to understand, through the own words of the subjects interviewed, their perspectives on their experiences ( Mendoza, 2006 ). This sample consisted of 20 female and male workers from the province of Barcelona-Spain who had worked or are currently working in actions related to the elimination of gender-based violence.
For the qualitative analysis of these data, the grounded theory was applied, which supposes the emergence of social patterns from research data ( Trinidad, Carrero, & Soriano, 2006 ). As a guide for the presentation of the results, the recommendations of the COREQ ( Tong, Sainsbury, & Craig, 2007 ) were followed.
Sample and context
The choice of the sample was not random. For the selection, snowball and theoretical sampling was used. Snowball sampling involves the selection of participants in a small group, which leads to other individuals who meet the characteristics; these then lead to others and so on until the number of individuals needed is obtained ( Fuentelsaz, 2004 ). On the other hand, theoretical sampling is used to select those units (persons, situations) that enhance the quality of the information ( Trinidad et al., 2006 ). One of the principal investigators was acquainted with three of the interviewees (without any personal relationship), while none of the investigators knew any of the other 17 participants. The interviewer was not familiar with the interviewees.
In this research, 18 women and two men participated from the province of Barcelona-Spain. To choose these professionals, the only inclusion criterion was having been involved in the past or being currently involved in prevention, intervention and eradication of gender-based violence (without taking into account the type of association or institution where they worked). The interviewees were members of teams created as a result of the trend to implement stable care programs for women and specific technical structures at the autonomous and local levels (state, autonomous, and local equality policies) ( Lombardo, 2002 ) after the implementation of Ley Orgánica 1/2004 de Medidas de Protección Integral contra la Violencia de Género in the Spanish State. The participants’ sociodemographic characteristics are displayed in Table 1 . To comply with ethical issues and preserve the interviewees’ identity, after the interviews, the participants received fictitious names, which were used from the transcripts onwards.
Table 1. Sociodemographic characteristics
| Type | ||||||
|---|---|---|---|---|---|---|
| Participant | Age | Sex | Children | Marital status | Function | of institution |
| Laura (5) | 36 | Woman | One daughter | Divorced | Coordination | Public |
| Cristina (10) | 52 | Woman | Two sons | Married | Social Educator | Public |
| Lidia (9) | 40 | Woman | No | Single | Coordinator of gender equality programs | Public |
| Carla (8) | 59 | Woman | Two sons | Married | Social worker | Public |
| Esther (7) | 38 | Woman | No | Married | Psychologist | Public |
| Julia (4) | 54 | Woman | Two sons | Married | College teacher | Private |
| Marisa (6) | 47 | Woman | One daughter and one son | Married | Psychologist | Public |
| Sofía (2) | 77 | Woman | Two sons and one daughter | Divorced | Coordinator women’s association | Private |
| Javier (3) | 43 | Man | One daughter and one son | Married | Private association | Private |
| Mireia(1) | 44 | Woman | Two daughters | Married | Psychologist | Public |
| Ana (11) | 27 | Woman | No | Single | Psychologist women’s association | Private |
| Sonia (12) | 56 | Woman | One daughter | Married | Social educator | Public |
| Araceli (13) | 53 | Woman | One son | Married | Equality technician | Public |
| Susana (14) | 52 | Woman | One son | Married | Psychologist | Public |
| María (15) | 27 | Woman | No | Single | Psychologist in association | Private |
| Jorge (16) | 28 | Man | No | Single | Psychologist in social entity | Public |
| Daniela (17) | 46 | Woman | No | Single | Legal counselor and lawyer | Public |
| Sílvia (18) | 43 | Woman | One son | Married | Center coordinator and social educator | Private |
| Beatriz (19) | 38 | Woman | One daughter | Married | Legal advisor | Public |
| Judith (20) | 36 | Woman | No | Married | Psychologist in women’s care | Public |
Procedure
Instrument
The instrument used was the semistructured interview. This is considered as a planned and goal-oriented interaction between two people. The interviewee gives his opinion and the interviewer collects that particular view ( Campoy & Gomes, 2015 ). The interview was created ad hoc for the purpose of this research. A short questionnaire was also prepared to collect the participants’ sociodemographic characteristics.
Before the elaboration of the interview, an exhaustive search was performed of the most representative terms related to the following theme; violence, gender-based violence, burnout, occupational health, health of workers engaged in teams specialized in violence, and self-care. Then, a reference based was created for all the team members. To design the interview, background experiences in contexts like our research context were used, as these could serve as a guide to design our study. In addition, the members of the research team discussed the interview questions and themes until they reached a consensus on these topics. Finally, a semistructured interview was created with open questions, which was sufficiently flexible to be able to identify themes the researchers had not captured in advance. Next, the general themes are presented, as well as some of the interview questions used:
Questionnaire with sociodemographic data.
Professional trajectory: In what labor conditions do you perform your work? What are your responsibilities? Why did you start working with violence? How long have you worked with this theme?
Statements about violence: What does violence mean for you? What is gender-based violence? What types of violence do you recognize?
Conflicts and work-related violence: What forms of violence have you met in this work context? Have you experienced some type of conflict in your workplace? What is the effect of working with violence in the conflicts?
Health and Self-Care: How is your physical and psychological health doing? Do you believe that working with violence affects your health? Do you perform any personal care measure? Are there institutional care measures?
Data collection and analysis strategy
The interviews took between 30 and 60 minutes, were held face-to-face in Spanish (the only people present were the investigator and interviewee), and took place over an eight-month period, from October (2016) till June (2017). First, the participants were contacted by telephone, agreeing on a suitable place to guarantee their participation in the study. In addition, field notes were taken during the interviews, including: incidences, the interviewer’s impressions, non-verbal language, and other considerations. Interviews were held until the theoretical saturation of the data was reached (this means that the collection of new data no longer provides additional information to explain the existing information ( Vivar, Arantzamendi, López-Dicastillo, & Gordo, 2010 ).
All interviews were recorded with a simple recorder and transcribed using InqScribe software. To analyze these interviews, the premises of the Grounded Theory were followed. Following the method proposed by this theory and the constant comparative method (collecting, coding and analyzing the data in a systematic way) ( Vivar et al., 2010 ), open, axial and selective coding of the reported information was carried out, as follows:
Open coding: the main concepts were identified through the “line by line” process (Strauss, Corbin, & Zimmerman, 2002), which supposes a detailed analysis of each of the interviews. After this analysis, codes were assigned to represent the ideas and situations detected in the interviewees’ words. In addition, a script was created with comments on the identified elements. Based on this initial coding, the themes were established which the participants represented most, departing from the axes created in the interview script (health, self-care, work-related violence, work-related conflicts, professional trajectory, violence, and gender-based violence).
Axial coding: the data collected in the previous phase were grouped in semantic families, systematically constructing the categories and subcategories and inquiring about existing relationships among them. The script with comments was used as a guide. At the end of this process, 23 categories and 90 subcategories emerged, organized in three dimensions (health, ideas about violence, and work-related conflicts) related to the main research axes.
Selective coding: we inquired about the central meaning or idea of the research, exhaustively integrating, refining and developing the categories surrounding a central theoretical concept (health problems and conflicts). The categories were reduced to 21, as two were similar and therefore combined. Finally, 90 subcategories were obtained. Furthermore, after the selective coding of the data, the theoretical saturation of the different categories and subcategories was identified, permitting the final construction of the central categories in the study through the analysis of the properties and theoretical meaning of their contents.
The investigators met every two weeks and/or every month to analyze the data. In addition, they shared doubts, suggestions, and comments by email. In that period, the suitability of the categories was discussed, as well as their relationship with the subcategories and their properties. During those meetings, they particularly debated on the theoretical saturation of the data (and hence about the quality of the categories) and on the need to proceed with the theoretical sampling. The interviews were analyzed in two batches. First, 11 interviews were analyzed. After the analysis, the researchers identified that some categories had little meaning and properties, which is why they proceeded with the theoretical sampling. The saturation point was reached after nine additional interviews (second batch). For the analysis, the interview transcripts were used, together with a shared Excel database, to construct the matrix of analytic dimensions, categories, subcategories, and elements.
To improve the methodological quality of the study, an intra-method methodological triangulation was designed which, according to Aguilar and Barroso (2015) , involves the review of information at different points in time. For the sake of this triangulation, the transcripts were reread on several occasions and compared with the result matrix during the months after the end of the analysis (March and May).
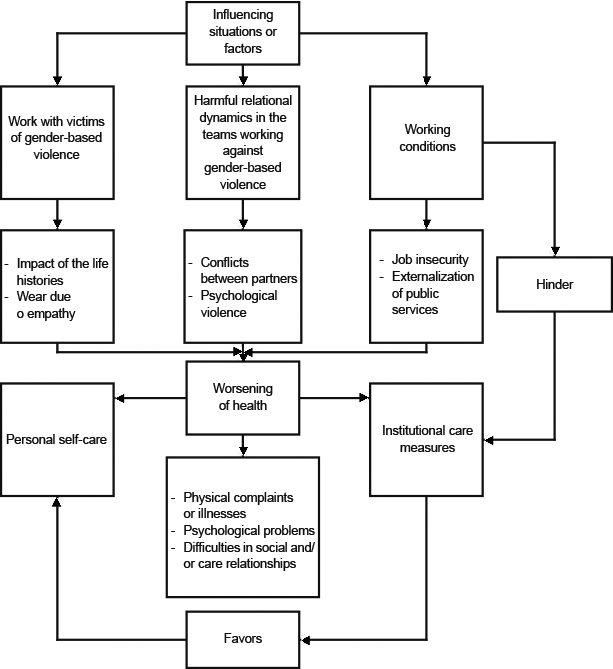
To locate and relate the phenomena that emerged from the categories and graphically represent the situation under analysis, we created a conceptual map to interpret the relations inferred among the phenomena detected in the interviewees’ discourse ( Figure 1 ).
Ethical aspects
All participants were informed of the aims and phases of this investigation. Therefore, an informed consent form was used, which included information on: objectives, method, and rights of the interviewee. All participants were required to sign this form before their inclusion in the study. The interviewees were informed about the team members and the status and credentials of the interviewer. The ethical aspects of this research complied with the guidelines for good research practices of Universitat Autònoma de Barcelona (2013) . There are no conflicts of interest in this study.
Results
The analysis of the interviews resulted in 560 elements, which were grouped in three dimensions, 21 categories, and 90 subcategories. Due to the large quantity of information resulting from the data analysis in this study, an explanation and detailed interpretation of all of these dimensions, categories, and subcategories would go beyond the limits of this article. Therefore, and to respond to the proposed objectives, we will analyze those data that offer a larger quantity and higher quality of information. The data are organized into six categories within the dimensions “Health and daily life” and “Conflicts at work” ( Table 2 ). These dimensions, categories, and subcategories were mutually related in a central conceptual map, which allows us to explain the interpretation process of the extract information ( Figure 1 ). To clarify and support the results displayed, the set of citations for each category is shown in Tables 3 and 4 . We consider that this presentation mode facilitates the organization of the results and offers a simpler and more contrasting view.
Table 2. Dimensions, categories, and subcategories analyzed
| Dimension: health and daily life | Dimension: work-related conflicts | ||
|---|---|---|---|
| Categories | Subcategories | Categories | Subcategories |
| Repercussions for health | Physical | Institutional problems | Dismissal |
| Psychological | Job insecurity | ||
| Behavioral | Political changes | ||
| Institutional maltreatment | |||
| Lack of resources | |||
| Lack of economic transparency | |||
| Employment repercussions | Transfer | Team problems | Discussions |
| Exhaustion | Triangulation | ||
| Discouragement | Competitiveness | ||
| Traumatization of the team | |||
| Competitiveness | |||
| Self-care | Definition of self-care | ||
| Strategies | |||
| Implementation problems | |||
| Institutional care measures | Basic conditions | ||
| Physical conditions | |||
| Psychological conditions | |||
| Insufficient measures | |||
| Proposals for improvement | |||
Table 3. Word-for-word quotes from the categories: repercussions on health and repercussions on work
| Category | Participant | Quote | Text |
|---|---|---|---|
| Repercussions on health | Lidia | A | “We are on the frontline, we have sustained the crisis (…) It has really gotten to us these years. We all have something that hurts, if you don’t go down...” |
| Clara | B | “This work has made me seek many things, which are not relevant to it but I have to thank them …” | |
| Judith | C | “Lately you sometimes see, as you see such bad and important situations in which you play a very important role, in which I can’t get the woman’s history out of my head, in my free time” | |
| Silvia | D | “Getting pregnant with this tension you feel is impossible. That is, whether you want to or not you blame yourself a bit for not having done otherwise and for not having gone on leave immediately...” | |
| Ana | E | “I haven’t experienced migraine, headaches, lack of sleep, fatigue, sadness… I never feel bad. I am very rational” | |
| Lidia | F | “My partner gets angry at me, he said I didn’t have to do this …” | |
| Marisa | G | “I completely lost my immunity, I started to get sores, I was totally exhausted” | |
| Lidia | H | “The diseases are also telling you how much you have borne and kept quiet” | |
| Javier | I | “What you didn’t say at work you said it at home…” | |
| Repercussions on work | Marisa | J | “I can get terrible statements, but if I simply listen to that terrible discourse and that’s it, if I am no longer motivated, I have no illusions… that can be lethal” |
| Laura | K | “In something of course… yes… but I have always seen to the women or interacted with them differently because someone was pinching me here or… but well... unconsciously something must have been transmitted of course” |
Table 4. Literal quotes in the category conflicts at work and literal quotes categories self-care and institutional care measures
| Category | Participant | Quote | Text |
|---|---|---|---|
| Conflicts with the institution | Carla | A | “The burden, everything related to charging in management can cause conflicts and health problems in a team that does not know how to manage it …” |
| Esther | B | “There are low salaries with emotionally very stressful jobs… there is great turnover in the teams because the recognition part is not there, the good working conditions are not there…” | |
| Mireia | C | “This thing of being required to demonstrate and deliver what I have been doing for so long…” | |
| Carla | D | “You can think, jeez, I get everything… if they do not put it on another person…” | |
| Conflicts in the teams | Judith | E | “We are a team, which is traumatized. Historically I believe it has been traumatized but – there is a person on leave – there is a way, a self-care strategy is to give you power to try and analyze how the violence affects our team” |
| Javier | F | “In this last entity I have experienced situations of violence, let’s see how I’d put it… ah, I don’t know… ah… I don’t know, it’s hard to recall… if I recall having felt bad but no idea… I don’t know” | |
| Sonia | G | “There was a very abusive environment, it got to me emotionally… I needed treatment for depressive symptoms” | |
| Esther | H | “Violence in the team is terrible, it’s devastating… in my case there has been great anguish, not eating and having great difficulty to sleep” | |
| Self-care | Ana | I | “Self-care means gaining awareness and the need to think of oneself, positive self-concept, self-esteem, safety and reconstruction” |
| Julia | J | “Self-care is a space that allows you to recognize yourself as needing care” | |
| Sofía | K | “Self-care means working for yourself, doing things for yourself, being well yourself…” | |
| Marisa | L | “Self-care is what I got left when everyone goes to sleep… I am very tired and I want to sleep” | |
| Javier | M | “My self-care is, if I can, I sleep. And, if I can, I take a shower. And if I can, I eat… and if I’ve got that I already feel that I’m taking care of myself” P. 7. | |
| Institutional care measures | Beatriz | N | “I believe that the institution should preview, on the one hand, a standard, in the decree that regulates that service’s safe houses...” |
| Lidia | O | “I do not have to be well because I spend my salary on therapies. Here the institution would have to do things to prevent psychosocial risks” | |
| Marisa | P | “What’s good about them is that they allow us to provide plenty of education and supervisions” | |
| Beatriz | Q | “I believe that the institution should preview, on the one hand, a standard, in the decree that regulates that service’s safe houses...” |
Categories repercussions on health and repercussions on work
For the category of repercussions on health, the interviewees claim to suffer mainly physical, psychological, and behavioral consequences. The most cited physical problems were burnout syndrome, stress, reduced immunity, tics, headaches, musculoskeletal problems and somatization. In general, the participants’ discourse indicates generalized tiredness “I was completely exhausted” and the feeling of living with a lot of stress “you blame yourself a bit for not having done otherwise” ( Table 3 , quotes A, D, G, H).
Among the psychological repercussions found there are symptoms of anxiety and depression: negative thoughts, restlessness or insomnia and feelings of loneliness. They were expressed by the inability to disconnect from work “I am unable to get the woman’s history out of my head,” leaves due to depression and anxiety or constant worry ( Table 3 , quote C). The interviewees affirm that they are also victims of behavioral repercussions, which would have to do with problems with the family environment or with their friendships. The main consequences cited in this aspect are discussions in the couple “my partner gets angry at me...,” reduction of free time or discussions with friends and difficulties to set limits ( Table 3 , quotes F and I). In response to the question “What repercussions does work with violence have for you?,” used to investigate the consequences suffered, two of the participants affirmed that they had not suffered health consequences ( Table 3 , quote E). Their narratives also indicate that the repercussions were only positive aspects, such as personal growth, the search for resources “This work has made me look for many things ... I have to thank them,” strengthening or learning ( Table 3 , quote B).
The category labor repercussions give us information about the incidence of working with violence in the same professional practice; the interviewees affirmed that the main consequences in this sense are related to the transfers with the users, demotivation for the work to be done, and loss of empathy ( Table 3 , quotes J and K). The results presented above respond to our first objective: the analysis and interpretation of the repercussions for the professionals.
Categories institutional problems and team problems
The categories institutional problems and team problems provide information about the causes of the repercussions the professionals interviewed in this research suffered and, therefore, provide a response to our second objective: description, analysis and interpretation of the influential factors in the workers’ health.
Among all the subcategories that emerged from the narratives analyzed, those that all the participants cited as strongly influencing the problem are detailed below: first, the job insecurity “there is no part about good working conditions...” or the lack of resources to carry out the work in optimal conditions “I get everything ... if they do not put it on another person...” ( Table 4 , quotes B and D). The main elements that make up these concepts are the practice of unpaid overtime, low salaries, temporary contracts and part-time contracts. On the latter, participants say they do not have enough time at work to provide adequate care to users or to meet the required commitments.
Second, the institutional abuse they suffer because of these precarious working conditions they describe. The analysis of the interviewees’ discourse indicates that “the burden” of work in terrible working conditions in some cases is a reason that directly and clearly affects the health of these workers ( Table 4 , quotes A and C).
Thirdly, the participants affirm that the conflicts in the work teams in this sector are strongly present and entail repercussions both at work and at a personal level. The narratives of these professionals reflect that these conflicts not only have to do with factors related to the type of work or working conditions, but also with the reproduction of violent dynamics present in other relational systems that would be reproduced in this sector. The most present subcategories would be discussions, competitiveness and traumatization of teams, “we are a team, which is traumatized...” ( Table 4 , quote E). These factors turn into the existence of violence in some cases, “in this last entity I have experienced situations of violence...,” mainly psychological, in the work teams that work to eradicate gender violence ( Table 4 , quotes F, G, and H).
Categories self-care and institutional care measures
To respond to our third study objective, we investigated the interviewees’ concept of self-care. The analytic elements that constitute the category “definition of self-care” were: “Space that allows you to recognize yourself as needing care,” connection with oneself, free time, emotional management tools, good relations, to take oneself into account and “gaining awareness and the need to think about oneself” ( Table 4 , quotes I, J, and K). The strategies that the interviewees say they carry out for self-care are mainly to disconnect, repair, share, reflect, and live loneliness, hope and have illusions, play sports (connect with the body), eliminate harmful habits, share experiences, have contact with nature and animals, be positive, do therapy, and perform distracting activities.
The participants expose some problems for the accomplishment of this self-care though. The main difficulties exposed are related to the condition of being a woman (refers to the burden of tasks and the assigned family care roles), the lack of time “self-care is what I have left when everyone goes to sleep...” and the lack of institutional response to the physical and psychological problems the workers report “I do not have to be well because I spend my salary on therapies” ( Table 4 , quotes L and O). The narrations of the interviewees indicate that there are deficits in the practice of this care.
Likewise, the institutional care response constitutes the following category; institutional care measures. In the first place, the participants’ discourse reveals that it is essential to have basic working conditions (salary, schedule, vacations, etc.) as a starting point for institutional care. Secondly, the subcategories physical care and psychological care are presented. The elements that make up these subcategories are supervisions, training and the emphasis on postural improvement ( Table 4 , quote P). On the other hand, the main problems our participants reported are incomprehension, political changes, lack of institutional commitment, and lack of awareness about the workers’ needs ( Table 4 , quotes N and O). The interviewed professionals affirm that there should be legal regulations, facilities to take sabbaticals, supervisions, constant training, and an increase in personnel as institutional measures to improve self-care and working conditions ( Table 4 , quote Q).
Discussion and conclusion
The study participants’ reports draw a scenario full of obstacles, deficiencies, and heavy professional burdens. The repercussions described entail severe consequences for health that, far from being solved, are mostly ignored or treated partially by the institutions where they perform their professional work. These difficulties derive from some situations in the social, economic, and relational context of work in care for victims of violence ( Figure 1 ).
The study participants relate the physical and psychological problems they suffer or have suffered, occasionally and in the long term, with the type of work that is performed; work against gender-based violence. Therefore, the impact of these issues is recognized as one of the main triggers of the stress and exhaustion suffered.
Freudenberger (1974) defines burnout as a syndrome in response to the chronic emotional stress (physical and psychological exhaustion) individuals dedicated to caring for others are victims of. The physical and mental health conditions the study participants described because of their professional practice could indicate burnout.
Some studies clarify and offer information on the variables that influence the emergence of this syndrome. To give an example, in a study by Gil-Monte (2003) on the emergence of burnout in nursing, the importance of addressing problems in the organizational context (work climate, working conditions, etc.) was mentioned to avoid its emergence among the professionals. In another study, involving teachers, some social or work-related factors (misalignment in schedules, lack of external support, conflicts with the institution, etc.) were also considered as antecedents of the health problems detected ( Castillo & Alzamora, 2015 ). Soto-Rosales and González-Losada (2018) argue that the social workers face highly stressing tasks, due to the complexity of their professional practice.
The work-related framework (extreme work-related demands, personal characteristics of the workers, social service work, etc.) in those study results coincides with the information analyzed in our study. Nevertheless, the difference in the roles, tasks, themes, users, or expectations among the different job contexts become realities that are hard to compare, as care for victims of gender-based violence implies not only working with people, but also constant contact with the horror of violence.
Thus, beyond the social service work described in the studies cited about burnout, some more specific studies involving professionals working with the elimination of violence highlight the costs of working with emotionally stressful situations and the difficulties of caring for those who suffer emotionally ( Claramunt, 1999 ; Arón & Llanos, 2004 ; Ojeda, 2006 ; Acinas, 2012 ; Bernad, Pérez, Díaz, García, & Villagrasa, 2013 ; Cantera & Cantera, 2014 ). Our findings are in line with those authors’ findings, arguing that listening to the stories and experiences of the service users compromised the interviewed workers’ health. In addition, and according to the professional discourse analyzed, besides the emotional impact of working with violence, there are two factors with a crucial influence on the interviewees’ self-perceived health: the working conditions under which the work is carried out and the reproduction of the violence that occurs within the teams.
Regarding the first factor, working conditions, it is important to contextualize this labor market within the economic crisis that took place in 2008 worldwide, which meant a drop in economic activity, a long period of recession and cuts in public spending ( Sánchez-Martínez, Abellán-Perpiñán, & Oliva-Moreno, 2014 ). Based on their experience, the participants affirm that the outsourcing of services and the job insecurity resulting from the economic crisis negatively influence their working conditions and their health.
The second aspect analyzed, the reproduction of violence in the teams that work against it, is a form of psychological violence among colleagues, which includes abusive actions such as excessive demands, threats, pressure, insults, blackmail, or other forms of disrespect. In a qualitative study ( Quiñones et al., 2013 ), it was stated that violence can be generated in work teams engaged in care for victims of gender-based violence, and that it is not due to stress derived from work, but to the interactions that reproduce the political, economic and control system that sustains the patriarchal ideology.
In a study on the self-care of professionals who take care of victims of violence, Arón and Llanos (2004) exposed the traumatization of the teams as a difficulty in these professional environments. This traumatization was defined as “the effect of reproducing the dynamics of the circuit of violence in the workgroup” (p.5). On the other hand, Izcurdia and Puhl (2017) argue that the contradictions (on different viewpoints) in the transdisciplinary teams in charge of care for victims of family or gender violence suppose difficulties that need to be overcome. That is the only way to achieve a common perspective among the different professionals on the complex psychosocial realities. Finally, and according to Quintana (2005) , the traumatization of the teams working against child mistreatment affects the mental health and the organizational climate, which can make these professionals experience emotional fatigue, irritability, or feelings of abandonment, among others.
The ideas taken from these studies alert us about the presence of conflicts or violence that result from the relational interactions in the teams that oversee fighting violence. Our study results are in line with the results presented earlier.
In line with the literature ( Santana & Farkas, 2007 ; Betta, Morales, Rodríguez, & Guerra, 2007 ; Bernad et al., 2013 ), the interviewees’ statements in this research invite us to continue working on finding healthy strategies that allow the professionals to effectively face the problems they suffer. One of the tools presented as a mechanism to protect oneself from the stress that work with violence generates is active self-care. From the participants’ accounts, the need to understand active self-care is understood not only as a personal care strategy, but also as a labor and professional right. Self-care needs to be systematized and preventive, it needs to be recognized and incorporated into violence training plans, and, finally, it needs to be assumed as a usual practice in the occupational risk plans of institutions and companies. In addition, according to the data analyzed in this study, the work-related conditions are the main obstacle for the implementation of institutional care measures (Figure 1).
Among the limitations of this study is the failure to thoroughly explore the psychological repercussions the workers were suffering. This exploration could have entailed certain prejudices for the interviewees, as well as some ethical problems in this investigation. Likewise, the participants may avoid going deeper into certain topics because they are too intimate and sensitive. It would be interesting to consider these aspects in the design of other studies. The main strength of this research is not simply the detailed description of this reality, but the interpretation (i.e., the model) based on the data and the method employed. This model served to grant a holistic meaning to the health problems the workers in the sector report and their relationship with the existing socioeconomic characteristics and between the work and the violence. The figure presented allows us to confront what Arón and Llanos (2004) indicate about the teams specialized in violence, affirming that the lack of references able to explain the problems the teams suffer favors the trend to attribute the deficits to personal and/or relational shortcomings.
In conclusion, and considering the descriptive and exploratory design of this study, our findings allow us to draw and visualize an unfavorable working environment for the workers in this sector. This image, in which the consequences for health are recurrent, should alert public and private institutions about the need to implement institutional care measures. These should be aimed at mitigating and preventing the professionals’ health problems and improving labor market conditions, thus ensuring the quality of the services provided.
The self-care practices the study participants described can serve as a guide or help to improve or implement psychosocial risk plans for companies and improve and provide self-care strategies to professionals in a personal way. Finally, it is important not to underestimate the reproduction of violent behaviors at the heart of these teams and their relationship with the labor unrest.

