











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Mild and major neurocognitive disorders (mild-NCD and major-NCD) (American Psychiatric Association, 2014) are nosological conditions characterized by alterations in the functioning of one or more cognitive domains with respect to the previous level. In the case of major-NCD, this alteration affects functional independence. Nowadays, both are worldwide public health problems due to their increasing prevalence resulting from the phenomenon of population aging (He, Goodkind, & Kowal, 2016; National Institute of Statistics and Geography, 2015). According to Alzheimer’s Disease International (2015), 46.8 million people around the world present an NCD. Moreover, an increase of up to 131.5 million has been projected for 2050 (Prince et al., 2015). At the same time, it is known that an individual with mild-NCD is ten times more likely to progress to major-NCD than an individual with the same characteristics, but without mild-NCD. These data emphasize the need for evaluation instruments that allow for the timely identification of older adults with signs or symptoms of a particular NCD (Petersen et al., 2014).
One of the most widely used instruments for the detection of NCDs is the Clock Drawing Test (CDT), because it is a brief test that permits the exploration of a wide range of cognitive processes including: attention, understanding of instructions, planning, visuospatial ability, visual construction, programming and graphomotor performance, numerical knowledge, abstract thinking, symbolic representation, and semantic memory (Blair, Kertesz, McMonagle, Davidson, & Bodi, 2006; Cacho-Gutiérrez, García-García, Arcaya-Navarro, Vicente-Villardón, & Lantada-Puebla, 1999; Freedman, 1994; Hubbard et al., 2008; Shulman, Shedletsky, & Silver, 1986).
Given the boom it has enjoyed as a screening test for the identification and assessment of NCDs, numerous methods have been proposed for its application and scoring, some of which seek to quantify the scores obtained by the patient (Blair et al., 2006; Cacho-Gutiérrez et al., 1999; Freedman, 1994; Hubbard et al., 2008; Shulman et al., 1986), while others attempt to analyze the type of performance they present (Parsey & Schmitter-Edgecombe, 2011; Rouleau, Salmon, Butters, Kennedy, & McGuire, 1992). Although the quantitative methods used to score the Clock Drawing Test are extremely useful due to the objectivity and practicality of counting right and wrong answers when performing the task, most of them do not allow for the analysis of characteristics in the performance of each phase of NCDs.
At the same time, although the qualitative methods proposed to date to analyze the clock drawing facilitate the detection of specific features in the performance of patients, they lack systematization and objectivity, which creates ambiguity in the results and subjectivity in the interpretation. The review by Pinto and Peters (2009) showed that using both approaches (qualitative and quantitative) improves the identification of NCDs in comparison with the use of each method separately. Parsey & Schmitter-Edgecombe (2011) proposed a quantitative scoring method based on the qualitative criteria of Rouleau et al. (1992), which considers six error categories: 1. size, 2. graphic difficulties, 3. stimulus-dependent responses, 4. conceptual deficits, 5. spatial/planning deficits, and 6. perseverations. On the basis of these criteria, they were scored on a scale of 0 to 16 points. A cut-off point of 11 points was determined for major-NCD, 12-13 points for mild-NCD, and 14 points for cognitively normal respondents. In addition, a qualitative analysis revealed that the most frequent errors across the three groups were: conceptual, graphic, and spatial/planning difficulties. On the basis of these findings, it was determined that, in addition to the quantitative evaluation that provides scores and cut-off points, qualitative analysis can enhance the sensitivity of the CDT, specifically to distinguish between mild-NCD and normal cognition.
Accordingly, the purpose of this study was to validate the CDT scoring method proposed by Parsey & Schmitter-Edgecombe (2011) for screening NCD in Mexican older adults.
Method
Study design
This retrospective diagnostic accuracy study was conducted between July, 2016 and July, 2017 at the Memory Clinic of a university tertiary care hospital in Mexico City.
Participants
We invited men and women over 65 who agreed to participate, after signing an informed consent form. The sample was estimated with the aim of studying diagnostic performance and validation to find a moderate to high correlation between the Mini-Mental State Examination (MMSE) (Folstein, Folstein, & McHugh, 1975), the Montreal Cognitive Assessment-Spanish (MoCA-S) (Delgado, Araneda, & Behrens, 2017), and the CDT scoring method proposed by Parsey & Schmitter-Edgecombe (2011), with an error of α = 5% and a power of 80%. At least 51 subjects were required per group (51 cognitively healthy individuals [CH], 51 with mild-NCD and 51 with major-NCD). For test-retest reliability and intra- and inter-observer reliability, a sample of at least 23 subjects per group was estimated.
An NCD diagnosis was established on the basis of the criteria proposed by the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association (NINCDS/ADRDA) (McKhann et al., 1984), and the criteria of the Diagnostic and Statistical Manual of Mental Disorders, version 5 (DSM-5) (American Psychiatric Association, 2014) and the Clinical Dementia Rating (CDR) (Hughes, Berg, Danziger, Coben, & Martin, 1982), making it possible to classify participants into: cognitively healthy subjects (category 0), subjects with mild-NCD (category .5), and subjects with major-NCD (≥ 1). The Brief Neuropsychological Assessment in Spanish (NEUROPSI) (Ostrosky, Ardila, & Rosselli, 1999) was used for the evaluation of the cognitive sphere. This test, standardized by age and educational attainment in the Mexican population, makes it possible to explore six cognitive processes (orientation, attention, memory, language, reading and writing, and executive functions). It was considered that subjects who scored ≤ 1.5 standard deviations (SD) in NEUROPSI met the criterion for mild-NCD, while those with ≤ 2 SD fulfilled the criterion for major-NCD. Functional status was evaluated using the Katz index (score of 0-6 where higher scores indicate greater independence for basic activities of daily living, BADL) (Katz, Downs, Cash, & Grotz, 1970) and the Lawton and Brody Index (score of 0-8 points, where higher scores indicate greater independence for the instrumental activities of daily living, IADL) (Lawton & Brody, 1969). Likewise, the informant’s report was evaluated through the B-ADL (Bayer Activities of Daily Living Scale), an instrument comprising 25 items, which evaluates activities with high and low cognitive demand (Sánchez-Benavides et al., 2009). A score above 3.3 is indicative of functional impact in major-NCD (sensitivity: .81, specificity: .72).
Exclusion criteria were participants who were: illiterate; with severe visual or auditory deficit; with the presence of severe or uncontrolled neurological, toxic, metabolic, infectious, or vascular diseases; psychiatric disorders such as untreated or uncontrolled depression and/or schizophrenia; heart, liver or kidney diseases, cancer, or any other type of uncontrolled systemic disease; and/or motor alterations that hinder the application of cognitive tests.
Measurements
A geriatric interview was conducted in which general data were obtained: age, sex, and educational attainment. Subsequently, a cognitive evaluation was performed, consisting of the application of the following instruments: MMSE (Mini-Mental State Examination) (Folstein et al., 1975). The maximum score is 30 points; the cut-off point for major-NCD is 24 points (sensitivity: 91%, specificity: 38%); the cut-off point < 26 for mild-NCD (sensitivity 92%, specificity: 42%), and MoCA-S (Aguilar et al., 2017), the Spanish version, validated in Mexican population; total score 30 points, cut-off point for major-NCD:24 (sensitivity 98%, specificity 93%); for mild-NCD with a cut-off point of 26 (sensitivity 80%, specificity 75%).
The CDT was scored based on the scoring method proposed by Parsey & Schmitter-Edgecombe (2011), using a version translated into Spanish by a certified translator, and subsequently reviewed and approved by an expert committee (Table 1).
Table 1 Version translated into Spanish: CDT rating register proposed by Parsey & Schmitter-Edgecombe (2011)
| Type of error | Errors | Points |
|---|---|---|
| Clock size | Small: less than 1.5 inches (3.8 cm) in diameter | 1 |
| Large: more than 5 inches (12.7 cm) in diameter | 1 | |
| Graphic difficulties | ||
| Inaccurate lines with distortions of the face or numbers that are hard to read. | Mild: some distortions of the clock face and/or hands and/or numbers. Overall performance was adequate. | 1 |
| Hands that are not straight and do not connect in the center of the clock. | Moderate: obvious distortions, but overall performance is still interpretable. | 2 |
| General performance seems inaccurate or clumsy. | Serious: Obvious, severe distortions, which may result in a non-interpretable drawing. | 3 |
| Responses related to stimuli | ||
| The tendency of the drawing dominated or guided by a single stimulus. | The time is written with letters or numbers, near or next to the numbers 11 and 10. | 1 |
| Hands point to the numbers "11" and "10" or absence of hands. | 1 | |
| Conceptual deficits | ||
| Errors reflect a loss/deficit in accessing knowledge of the attributes, characteristics and meaning of a clock. | Poor representation of the clock (clock without numbers or missing the outer circle, outline of the clock). | 1 |
| Poor representation of time (hands missing or poorly represented, incorrect length of hands or both hands have the same length, time written with letters or numbers on the clock). | 1 | |
| Numbers missing or in the wrong order (the sequence begins with "1" in the position of "12", the sequence of numbers ends before or does not reach 12, numbers missing in the sequence). | 1 | |
| Spatial and planning difficulties | ||
| Deficits in the distribution of numbers on the clock face. | Neglect of left hemispace (numbers only placed in right hemifield). | 1 |
| Difficulty planning, with large spaces before numbers 12, 3, 6, or 9. | 1 | |
| Difficulty in the spatial distribution of numbers, without any specific pattern, disorganization. | 1 | |
| Numbers written outside the clock face, or numbers written on the circumference of the clock. | 1 | |
| Numbers written in the opposite direction to the clock. | 1 | |
| Perseveration | ||
| Continuation or repetition of the activity without proper stimulus. | Perseveration of hands more than 2 hands. | 1 |
| Perseveration of numbers: abnormal prolongation of numbers (e.g. numbers beyond number 12, or repetition of numbers). | 1 | |
| TOTAL ERRORS: | ||
| Final score (16 -Total errors): | ||
Source: CDT scoring scheme proposed by Parsey and Schmitter-Edgecombe (2011)
Procedures
The subjects performed the CDT as part of the cognitive evaluation. All participants were given an 8.5 x 11-in blank sheet and instructed to do the following:
“Draw the clock face, put in all the numbers and set the hands for 10 after 11,” If necessary, the full instructions were repeated one more time.
The CDT was rated according to the quantitative and qualitative method proposed by Parsey & Schmitter-Edgecombe (2011), which analyzes six categories: 1. size, 2. graphic difficulties, 3. stimulus-dependent responses, 4. conceptual deficits, 5. spatial/planning deficits, and 6. perseverations.
To obtain inter-observer reliability, two previously trained assessors (MASC and FRG), blind to each other, scored 23 clocks from each group, randomly selected using the adapted criteria. For intra-observer reliability, the evaluators scored the 23 clocks in each group at the beginning of the study and three months later.
Statistical analysis
The content validity of the instrument had been previously established by Parsey & Schmitter-Edgecombe (2011). In this study, due to the categorical nature of the items, the validation process was performed with non-parametric tests. The Spearman correlation coefficient was used to determine construct validity (convergence) when comparing the total score and each of the errors analyzed in the CDT with the applied cognitive tests (MMSE and MoCA-S). One factor analysis of variance (ANOVA) was undertaken, together with the Post Hoc DSM test to identify differences between the groups in the types of errors.
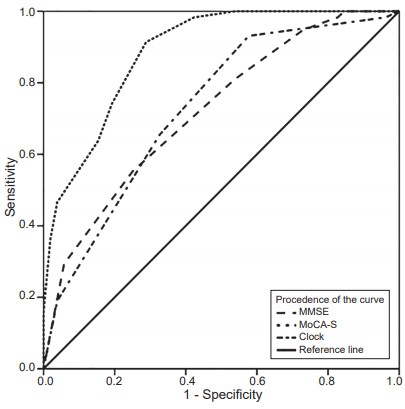
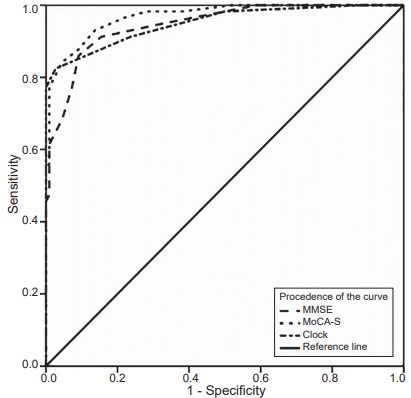
The kappa coefficient was obtained from the total score to analyze inter-rater reliability. The internal consistency of the test was determined in both raters using Cronbach’s alpha coefficient. The Receiver Operating Characteristics (ROC) curve was constructed and the area under the curve was calculated to estimate sensitivity and specificity and establish cut-off points and 95% confidence intervals.
All data analyses were performed using the SPSS statistical package version 20. The level of statistical significance established was .05 (SPSS Inc., Chicago, IL, version 20.0 for Windows).
Results
A total of 167 older adults were included (76% female, average age:75 [SD = ± 8], range 60-90 years, average educational attainment: 10.7 years [SD ± 5.2], range 0-2 2 years), 58 cognitively healthy subjects (CH, average age: 69.91 [SD ± 7.1]; average educational attainment: 12.4 [SD ± 3.8)]), 52 subjects with mild-NCD (average age:75.15 [SD ± 6.2]; average educational attainment: 10.2 [SD ± 5.6]), and 57 subjects with mild-NCD (average age: 81.8 [SD ± 5.9]; average educational attainment: 9.6 [SD ± 5.8]).
Regarding the cognitive sphere, scores were lower in the group with major-NCD, with statistically significant differences across all tasks, except for register and reading comprehension, compared with the CH and mild-NCD group. It was observed that the three groups differed in the overall scores of the MMSE, MoCA-S and CDT, and in the domains of temporo-spatial orientation, deferred recall, language block, and copying pentagons, whereas in executive function tasks, the group with major-NCD had the lowest score, followed by the group with mild-NCD and the CH group. (Table 2)
Table 2 Sociodemographic characteristics, cognitive and functional performance across groups
| CH (n = 58) | Mild-NCD (n = 52) | Major-NCD (n = 57) | F | gl | p | |
|---|---|---|---|---|---|---|
| Sociodemographic variables | ||||||
| Agea,b,c | 69.91 (7.1) | 75.15 (6.2) | 81.8 (5.9) | 48.92 | 2, 164 | < .001 |
| Educational attainmenta,b | 12.4 (3.8) | 10.1 (5.6) | 9.6 (5.8) | 4.98 | 2, 164 | .008 |
| Cognitive assessment | ||||||
| MMSEa,b,c | 28.6 (1.2) | 27.1 (2.1) | 20.4 (4.7) | 110.92 | 2, 164 | < .001 |
| MoCA-Sa,b,c | 27.3 (2) | 22.9 (2.9) | 13.7 (4.9) | 218.48 | 2, 164 | < .001 |
| CDTa,b,c | 14.8 (.9) | 13.9 (.9) | 9.3 (2.9) | 147.86 | 2, 164 | < .001 |
| Functional assessment | ||||||
| BDLA Functionalitya,b,c | 5.78 (.421) | 5.40 (.74) | 5.05 (1.18) | 10.50 | 2, 164 | < .001 |
| IDLA Functionalitya,b,c | 7.81 (.54) | 6.65 (1.7) | 2.67 (2.15) | 154.92 | 2, 164 | < .001 |
| Informant's report | ||||||
| B-ADLa,b,c | 1.4 (.3) | 1.8 (1.8) | 7.2 (1.34) | 19.38 | 2, 164 | < .001 |
Note: The data are presented as means and standard deviations. The analysis shows the differences between groups using the ANOVA test, post hoc DSM.
CH = cognitively healthy: Mild-NCD = mild neurocognitive disorder; Major NCD = major neurocognitive disorder; MoCA-S = Montreal Cognitive Assessment-Spanish; MMSE = Mini-Mental State Examination; BADL = Basic Activities of Daily Living; IADL = Instrumental Activities of Daily Living; B-ADL = Bayer Activities of Daily Living Scale-corroborated by the informant.
asignificant difference between CH and mild-NCD p < .005;
bsignificant difference between CH and major-NCD p < .005;
csignificant difference between mild-NCD and major-NCD p < .005.
In terms of functionality, as expected, the major-NCD group obtained the lowest score in a statistically significant way with respect to the mild-NCD and CH group; likewise, the NCD group had less functionality in comparison with the CH group (Table 2).
The internal consistency of the method used in this study to rate the CDT was α = .750. The test-retest correlation had an r = .637 (p < .001) and an intraclass correlation coefficient (ICC) of .774 (95% CI [.47, .90]; p < .001). Inter-observer correlation was .988 with a ICC = .993 (95% CI [.99, .99]; p < .001).
The area under the curve of the CDT rating method was .600 (95% CI [.511, .679]; p < .001), with a sensitivity of 40% and a specificity of 70% for the diagnosis of mild-NCD with a cut-off point of 14 points. For major-NCD with a cut-off point of 12 points, sensitivity was 90% and specificity 95% (Figures 1 and 2).
The analysis of the total score of the CDT showed statistically significant differences between the groups, with the CH group obtaining a higher score superior (
Table 3 Correlation between the CDT and the cognitive assessment instruments used in this study (MMSE and MoCA-S)
| Total score | Clock size | Graphic difficulties | Responses linked to stimuli | Conceptual difficulties | Spatial and/or planning difficulties | Perseverations | |
|---|---|---|---|---|---|---|---|
| MMSE | -.23* | -.48* | -.44* | -.58* | -.54* | -.45* | -.63* |
| MoCA-S | -.35* | -.50* | -.49* | -.65* | -.62* | -.49* | -.74* |
Note: MMSE = Mini-Mental State Examination; MoCA-S = Montreal Cognitive Assessment-Spanish. *Significant correlation, p < .01.
Finally, it was found that there were statistically significant differences among the three groups in all the errors, except in the section that measures responses linked to stimuli, of which the group with major-NCD had more errors than the group with mild-NCD. This group had a higher frequency of conceptual errors (93%), followed by spatial/planning difficulties (89.5%) and a greater number of errors in graphic difficulties in relation to the CH group (42.4% and 67.3% respectively p < .001) (Table 4).
Table 4 Errors in the CDT in groups studied
| CH (n = 58) | Mild-NCD (n = 52) | Major-NCD (n = 57) | p | |
|---|---|---|---|---|
| Clock sizea,b,c | 9 (15.8%) | 15 (28.8%) | 33 (57.9%) | < .001 |
| Graphic difficultiesa,b,c | 25 (42.4%) | 35 (67.3%) | 49 (86.0%) | < .001 |
| Slight | 25 (42.4%) | 35 (67.3%) | 20 (35.1%) | |
| Moderate | 0 (0%) | 0 (0%) | 20 (35.1%) | |
| Severe | 0 (0%) | 0 (0%) | 9 (15.8%) | |
| Responses linked to stimulib,c | 6 (10.2%) | 5 (9.2%) | 31 (54.4%) | < .001 |
| Conceptual difficultiesa,b,c | 13 (22.0%) | 21 (40.4%) | 53 (93.0%) | < .001 |
| Spatial and/or planning difficultiesa,b,c | 17 (28.8%) | 25 (48.1%) | 51 (89.5%) | < .001 |
| Perseverationsa,b,c | 2 (3.4%) | 5 (9.6%) | 30 (52.8%) | < .001 |
| Total errorsa,b,c | 1.22 (.9) | 2.10 (.9) | 6.74 (2.9) | < .001 |
Note: The data present the frequency and percentage of participants in the group that made each type of error.
CH = cognitively healthy; Mild-NCD = Mild Neurocognitive Disorder; Major-NCD = Major Neurocognitive Disorder;
asignificant difference between CH and mild-NCD p ≤ .001;
bsignificant difference between CH and major-NCD p ≤ .001;
csignificant difference between mild-NCD and major-NCD p ≤ .001.
Discussion and conclusion
This study showed that the combined quantitative and qualitative method proposed by Parsey & Schmitter-Edgecombe (2011) for the CDT is valid and reliable, and could therefore represent an excellent alternative for the detection of mild-NCD and major-NCD in Mexicans. The internal consistency of this method was .750 and its temporal stability was corroborated, since the test-retest and inter-observer results obtained a reliability (concordance or reproducibility) of .774. These results indicate that, despite the subjectivity entailed by scoring on the basis of qualitative criteria, this method is accurate, regardless of the scorer.
It was also observed that this method has satisfactory psychometric properties to detect major-NCD with a cut-off point of < 12 (sensitivity: 90%, specificity: 95%), whereas for the identification of mild-NCD with a cut-off point < 14, it showed a sensitivity of 40%, and a specificity of 70%.The psychometric properties previously published for the Parsey & Schmitter-Edgecombe (2011) method, with a cut-off point of ≤ 11, were: 57% sensitivity and 100% specificity for the detection of NCD, whereas with a cut-off point of between 12 and 13 for NCD, sensitivity was 39% and specificity 87%. Accordingly, these authors suggest that this method should be complemented by a more complex cognitive evaluation system for mild forms of cognitive impairment.
This study also made it possible to identify the degree of correlation between the quantitative and qualitative evaluation method of the CDT and other cognitive assessment tests used for the screening of major-NCD and mild-NCD. Both the total score and the score in each of the types of errors explored in this method showed a high correlation with the tasks evaluated (Freedman & Dexter, 1991).
At the same time, some researchers have said that the CDT is an instrument which, since it does not focus on the assessment of verbal skills like most screening instruments (MMSE, MoCA), makes it possible to explore other cognitive functions that are also affected in cases of cognitive deficit, such as visuospatial ability and visuoconstructional processes, which facilitates the complementary exploration of these aspects, in which alterations are usually heterogeneous (Ainslie & Murden, 1993; Sunderland et al., 1989).
Regarding the errors identified through the qualitative method criteria, it was found that, as in the study by Parsey & Schmitter-Edgecombe (2011), the most frequent errors across all groups were: graphic, conceptual and spatial, and/or planning difficulties.
According to these results, the three groups made performance errors. However, the complexity and frequency of errors was significantly lower in the CH group than in the others.
Likewise, a high frequency of conceptual errors and graphic difficulties was observed in the major NCD group. Moreover, the group with major-NCD had a higher frequency of errors in all categories than the CH and mild-NCD groups. This is to be expected, given that as cognitive deterioration progresses, compensatory cognitive resources and strategies are insufficient for identifying and preventing the occurrence of performance failures (Suchy, Lee, & Marchand, 2013).
The quantitative and qualitative scoring method of the CDT is easy to apply and has ideal psychometric properties for the detection of patients with major-NCD. It also offers the possibility of rating alterations in cognitive performance, thereby enhancing the characterization, comprehension, detection, and monitoring of this type of patients.
Limitations
A limitation of the study is the low sensitivity of the method used for screening mild-NCD. It is therefore suggested that these patients be further explored through both error analyses of the performance of the CDT and with more specific complementary tests, which will make it possible to improve the detection and characterization of this type of condition. The effect of educational attainment on the performance of the CDT must also be considered. Several authors have noted that this variable may affect graphic skills and the capacity for abstraction/conceptualization of the clock (Kim & Chey, 2010).

