











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Thirty-six point nine million people were estimated to carry human immunodeficiency virus in 2014 (HIV) and an additional two million were infected ( UNAIDS & UNICEF 2012 ; AIDS, 2015 ).
People with a severe mental illness (SMI) also make up a highly vulnerable group to the risk of HIV transmission. Information available about this group shows a high and growing HIV seroprevalence. Joska Kaliski and Benatar (2008) estimated that in 2008 the average seroprevalence of 10% (range 0% - 59.3%) was high when compared to that of the world population (0.8%, range 0.1% - 25.9%) ( AIDS, 2015 ). At the same time, we are dealing with a growing seroprevalence due to the fact that its ranges increased from 0% - 22.9% (prior to 1996) to 6% - 59.3% (after 1996) ( Joska et al., 2008 ). In this population group, said average seroprevalence would be located above the prevalences registered in countries receiving the classification of both low-level and concentrated epidemic, but not for countries with generalized or hyperendemic epidemic reaching a prevalence of 15% ( AIDS, 2015 ).
Besides greater HIV seroprevalence in population with SMI, life expectancy is shorter for this group in comparison with people not displaying mental illness ( Chan, 2010 ).
In addition to risk factors associated with HIV transmission in people with SMI, a study made in South Africa identified a statistically significant association between HIV+ diagnosis and the presence of unsafe sex practices with multiple and casual partners ( Henning, Krüger & Fletcher, 2012 ).
Around 450 million people in the world suffer some kind of mental illness ( WHO, 2010 ) and more than 100 million in Latin America and the Caribbean present a prevalence of 1.6% for nonaffective psychosis and schizophrenia, 8.7% for serious depression and 1.4% for bipolar disorder ( Kohn et al., 2005 ), and it has become necessary to begin to address the factors that put these populations at risk for HIV infection. We must remember that the lifetime prevalence for any mental disorder in Mexico is 26.1% and that the psychosocial problems faced daily by people who suffer them are multiple, so it is also important to address them. This is more so if we take into account information indicating that the prevalence of any mental disorder during our life is 26.1% in Mexico ( Medina-Mora, Borges, Benjet, Lara & Berglund, 2007 ).
Most of the epidemiological studies of risk factors associated with HIV prevalence in people with SMI have focused on individual factors or those inherent to a person’s characteristics, but very few have looked into the sociocultural factors conditioning sexual behavior and prevention practices ( Carey, Carey, Weinhardt & Gordon, 1997 ; Collins, Von Unger & Armbrister, 2008 ; Coverdale, Shotte, Ruiz, Pharies & Bayer, 1994 ; Loue & Sajatovic, 2006 ; Pinto, Mann, Wainberg, Mattos & Oliveria, 2007 ). These factors are deemed to be implied, are beyond a person’s control and reduce his/her ability to avoid risk, such as social exclusion for human rights’ violation ( Collins et al., 2008 ; Stevenson & Eilers, 1992 ; Taylor, 2007 ), poor quality and coverage of health services, and social stigma of illness, among others ( Collins, 2001 ; Kloos et al., 2005 ).
Regarding the transmission of HIV among people with SMI, it is important to analyze the interaction of individual and sociocultural dimensions. The two theoretical perspectives currently used to study individual risk practices are the so-called micro-approaches (directed to individual and local factors), linked to a biomedical model, and the macro-approaches (directed to social and structural factors), linked mainly to the fields of sociology and anthropology. The former does not consider the context, and focuses primarily on the search for universal patterns; the second focuses on the search for cultural particularities ( Ingham & Van Zessen, 1997 ; Phillips & Pirkle, 2007 ; Taylor, 2007 ).
However, an ecological approach should include micro and macro factors to understand and to develop programs and public policies that affect the reduction of HIV transmission ( Wilson, Wright, Safrit & Rudy, 2010 ). New approaches such as the syndemic theory consider important to study the added risk or burden attributable to interactions among selected comorbid conditions, which often include medical, behavioral, and social factors ( Batchelder, Gonzalez, Palma, Schoenbaum & Lounsbury, 2015 ).
As Shannon et al. point out, dialogue across social science and epidemiological research is needed, particularly because some macrostructural factors, such as stigma, migration or cultural norms are very difficult to measure and require complex methods to better understand their role in the potentiation or reduction of HIV risk ( Shannon et al., 2015 ).
That is why we did a narrative review of empirical studies published between January 1981 and July 2015 in order to cover information gaps. The objective is to know the different types of individual and socio-cultural factors empirically associated with the risk of HIV transmission among people with SMI.
Individual factors described and linked to a biomedical model that were identified in the analysis include: level of knowledge about HIV/AIDS and wrong believes, risky behaviors for HIV transmission and risky behaviors by type of severe mental illness.
On the other hand, the sociocultural factors related to psychosocial, sociological and anthropological models that were identified in the revision included: vulnerability to risk according to the demographic context, the effects of social stigma and communication on sexuality, a taboo on institutional contexts.
Method
A narrative review was made ( Pawson & Bellamy, 2006 ; Rychetnik, Hawe, Waters, Barrat & Frommer, 2004 ) to create a descriptive interpretative synthesis of the most notable reports in quantitative, qualitative and mixed (combining both quantitative and qualitative) articles about factors associated with HIV transmission risk among people with SMI. A search was made of scientific articles published in three different languages (English, Spanish and Portuguese) between January 1981 and July 2015. Three multidisciplinary indexes were used for this purpose: ISI Web of Knowledge, Redalyc and SciELO; one disciplinary index: PUBMED; and four multidisciplinary electronic databases: Ebscohost Web, ProQuest, Sage Publications and ScienceDirect.
The following keywords were established with the help of MeSH Database (first in English and then in Spanish and Portuguese): HIV/AIDS, HIV, AIDS, HIV Risk in combination with mental illness, mental disorders, affective disorders, mood disorders, psychiatric illness, and these together with: sexual risk behavior, sexual health, sexual practices, risk perception, cultural risk, stigma and risk, social networks, knowledge, beliefs and attitudes, and unsafe sex.
One thousand nine hundred ninety-six potentially pertinent studies were found of which 1 914 were excluded under the following criteria: a) 1 782 articles did not include risk factors associated with HIV transmission, or did not deal with empirical data; they were methodological, reviews or intervention reports; and b) 132 included only substance-related disorders, the HIV diagnosis or substance use or abuse preceding mental illness. At the end, 82 studies were included in the review.
The data analysis was made in terms of two dimensions associated with risk and/or vulnerability to HIV transmission: both the individual and the sociocultural one.
Structured coding results in relation to keywords were used in the process of organizing and analyzing information, so some individual and sociocultural factors were included: risky sexual behavior, sexual practices, risk perception, cultural risk, stigma and risk, social networks, knowledge, beliefs and attitudes as well as unsafe sex. In the same way, an open coding was performed to identify unforeseen issues and enrich the description of results on dimensions such as: age groups, kind of mental disorders, risk-related structural conditions, gender inequality, and communication about sex health in institutional settings.
Results
Characteristics of the reviewed studies
Eighty-eight per cent of the reviewed studies used quantitative methodology, while the rest applied qualitative or combined methodology. All of the quantitative works had a non-experimental design; most were analytical and cross-sectional, and 85% were multivariate. Only one study could be considered retrospective longitudinal. The qualitative and combined studies followed a non-experimental design with levels of descriptive and interpretative analyses of the meaningful dimensions of social action.
Most studies included patients from psychiatric clinics or hospitals (N = 35), community mental health centers or programs (N = 24), both combined (N = 10) and in non-specialized healthcare settings (N = 13). Most of the studies included patients older than 18 years (N = 73) and some cases focused on youngsters from 10 to 25 years (N = 8), while one of the studies did not specify the subjects’ age.
The severe mental illnesses included in the studies were varied but those including people with schizophrenia, depression and bipolar disorder in their samples prevailed (table 1).
Table 1 Most frequent kinds of SMI found in the study samples (N=82)
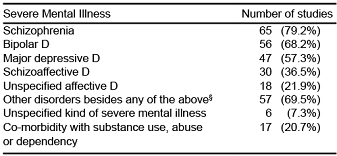
Note: § The most frequent disorders include: Personality disorder (20%), Anxiety disorder (16%), Organic disorder (8%), Behavior disorder (7%), Schizophreniform disorder (3%), Unspecified psychotic disorders (22%), Non-psychotic disorders (3%), Other unspecified disorders (20%)
Individual factors associated with the risk of HIV transmission
1. Knowledge and beliefs about HIV/AIDS
An average of more than 60% of the people with SMI correctly answered the questionnaire evaluating knowledge about HIV/AIDS ( Guimarães, McKinnon, Campos, Melo & Wainberg, 2010 ; Knox, Boaz, Friedrich & Dow, 1994 ; Magagula, Mamabolo, Krüger & Fletcher, 2012 ; Melo et al., 2010 ; Otto-Salaj, Heckman, Stevenson & Kelly, 1998 ; Randolph et al., 2007 ; Stevenson & Eilers, 1992 ; Strauss, Bosworth, Stechuchak, Meador & Butterfield, 2006 ; Wainberg et al., 2008 ).
Most of the research agrees that the level of knowledge of different groups of people with SMI is lower than that of the general population. Two studies were made in the United States, one with a female population ( Aruffo, Coverdale, Chacko & Dworkin, 1990 ) and the other with adolescents ( Katz, Mills, Singh & Best, 1995 ), while two other studies were also made, one with a male population in New Zealand ( Coverdale & Turbott, 2000 ) and one with a mixed population in Italy ( Grassi, Biacosino, Righi, Finotti & Peron, 2001 ). Nevertheless, a study carried out by Cates and Bond ( Cates, Bond & Graham 1994 ) in the United States found no significant differences.
The studies report different factors associated with the lower level of knowledge. One of them was the patients’ kind of mental disorders. For instance, a study made in South Africa found that those with psychotic disorders displayed less knowledge than those with some affective disorder ( Magagula et al., 2012 ). Low educational level and illiteracy made up another factor reported in a study of SMI patients of a psychiatric hospital in Brazil ( Melo et al., 2010 ). Lastly, an additional factor that could partly explain the lower level of knowledge of people with SMI is the limited participation of this population in institutional programs promoting health and HIV/AIDS prevention.
Different studies show the existence of mistaken beliefs about risk, prevention and transmission that could increase the spread of HIV/AIDS among people with SMI. Some found that people with SMI attribute the risk to people with homosexual preferences ( Ngwena, 2011 ; Stevenson & Eilers, 1992 ) and usually say that people with HIV have a sickly appearance due to the fact that they ignore the conceptual difference between HIV and AIDS ( Carey et al., 1997 ; Kloos et al., 2005 ; Strauss et al., 2006 ; Gordon, Carey, Carey, Maisto & Weinhardt, 1999 ).
Other investigations have detected the presence of uncertainty about how the virus is contracted and about the consistent use of condoms as a prevention strategy ( Carey et al., 1997 ; Otto-Salaj et al., 1998 ; Ngwena, 2011 ; Chuang & Atkinson, 1996 ). Lastly, Gordon et al. (1999) reported in the United States that people with SMI thought that the diagnostic test for HIV was a routine measure of their healthcare or psychiatric care, considering that the institutional implementation thereof might violate their human rights. Another investigation presented similar results to the previous results, where individuals with mental illness were more likely to have been tested than those without a mental illness. However, the elevated prevalence of HIV suggests that high levels of testing along with other prevention efforts are needed ( Yehia et al., 2014 ).
Knowledge about HIV and how to prevent it does not necessarily lead to preventive practices, even when people with SMI have suffered a sexually transmitted infection (STI). A study made in the United States shows a significant association between having had a STI diagnostic and having a high knowledge about HIV in this population. Nevertheless, this variable is also significantly associated with risky sexual behavior ( Vanable, Carey, Carey & Maisto, 2007 ). Another study from South Africa detected that despite a good level of knowledge, risky sexual behavior was observed ( Magagula et al., 2012 ).
2. Risky behavior for HIV transmission
Although the scarce sexual activity by people with SMI has been discussed, there is evidence that more than half of them are sexually active ( Abrantes, Strong, Ramsey, Kazura & Brown, 2006 ; Carey et al., 1997 ; Coverdale, Falloon & Turbott, 1997 ; Davidson et al., 2001 ; Guimarães et al., 2010 ). At the same time, a greater frequency of risky behavior for contracting HIV has been found in this population in comparison with the general population ( Bakare et al., 2009 ; Coverdale et al., 2000 ; Dickerson, Brown, Kreyenbuhl, Goldberg, Fang & Dixon, 2004 ; Matsuoka et al., 2003 ; RachBeisel, Scott & Dixon, 1999 ; Tubman, Gi, Wagner & Artigues, 2003 ).
As seen in Table 2, the risky sexual behavior with the highest prevalence in the SMI population is: unsafe sex (9% to 86%); substance use associated with sexual intercourse (23% to 39%); sexual intercourse with multiple partners (11% to 22%) and with a sexual partner who injects drugs (3% to 24%). On the other hand, there is also a high prevalence of injected drug consumption (1% to 24%), which in itself constitutes an additional risky behavior.
Table 2 Studies reporting prevalence of risky behavior for HIV transmission
| Population | Risky behavior during the last year | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lead author and year | Country where study was made | Context | Age | Gender | Unsafe sexual relations | Occasional sexual partners | Multiple sexual partners (ever) | Survival sex | Sexual intercourse with substance use | Sex partner injected drug user | Injected drug user | Sex partner VIH+ |
| Susser, (1995) | United States | Contexts unrelated to mental health care (N = 122) | nd | M | 24% | nd | 21% | 25% | nd | nd | nd | nd |
| Chuang (1996) | Canada | Psychiatric hospital or clinic (N = 151) | 25.6 ± 10.1 | F, M | nd | 16% | 17% | 7% | 23% | 4% | nd | nd |
| Menon (1997) | United States | Psychiatric hospital or clinic (N = 239) | nd | F, M | nd | nd | nd | nd | 32% | nd | nd | nd |
| Thompson, (1997) | Australia | Community center or program (N = 145) | 35.8 ± 1.1 | F, M | 29% | nd | 20% | 12% | nd | 24% | 16% | 3% |
| Carey M., (2001) | United States | Psychiatric hospital or clinic (N = 1558) | 37 ± nd | F, M | nd | Nd | 19% | 3% | nd | nd | 1% | nd |
| Davidson, (2001) | Australia | Community center or program (N = 234) | 20 to 65 years | F, M | 35% | 22% | 22% | nd | nd | 3% | 6% | nd |
| Chandra (2003) | India | Psychiatric hospital or clinic (N = 618) | 32 ± 10.2 | F, M | nd | nd | 61% | 65% | nd | nd | nd | nd |
| Strauss, (2006) | United States | Contexts unrelated to mental health care (N = 353) | 49 ± 9.0 | M | nd | nd | 27% | nd | nd | nd | 17%a | nd |
| 103">Wainberg (2008) | Brazil | Psychiatric hospital or clinic and Community center or program. (N = 98) | 41.8 ± 11.1 | F, M | 44%b | nd | 29%b | 20%b | 39%b | nd | nd | nd |
| Guimarães (2010) | Brazil | Psychiatric hospital or clinic with ambulatory care (N=2475) | 48% older than 40 | F, M | 80% | nd | 61% | 17.% | 24.8% | nd | 3% | nd |
| Himelhoch (2011) | United States | Community mental health clinics (N = 153) | 47 ± 8.1 | F, M | 86% | nd | nd | 27% | nd | nd | 24% | nd |
| Henning (2012) | South Africa | Psychiatric hospital | 39.1 ± 12 | F, M | 39% high risk behavior (without specifying which) | 5% | nd | |||||
| Guimarães (2014) | Brazil | Public psychiatric hospital and public mental health outpatient clinics (N = 2237) | Older than 18 | F, M | 80% | nd | 65% | 26% | nd | nd | 3% | nd |
| Lundberg (2015) | Uganda | Psychiatric hospital. (N = 602) | 18-49 45% 18-29 | F, M | 9% | nd | 11% | nd | nd | nd | nd | nd |
Note: a Behavior for more than one year; b behavior over the past three months; nd = data unavailable; F = female; M = male
Substance use and abuse is more prevalent in this population than in the general population ( Carey, Carey, Maisto, Gordon & Vanable, 2001 ) and it is a risk factor associated with a longer record of risky behavior ( Abrantes et al., 2006 ; Carey, Carey, Maisto, Schroder, Vanable & Gordon, 2004 ; Himelhoch et al., 2011 ; Kalichman, Kelly, Johnson & Bulto, 1994 ; Weinhardt, Carey, Carey, Maisto & Gordon, 2001 ).
Different studies have found significant associations between substance use and unsafe sexual practices ( Coverdale et al., 1997 ; Himelhoch et al., 2011 ; Meade & Sikkema, 2007 ). They have also found a connection between use and a search for multiple sex partners ( Coverdale et al., 1997 ), as well as occasional or unknown sex partners ( Meade, Graff, Griffin & Weiss, 2008 ; Susser et al., 1995 ). A study made in the United States with adolescents undergoing psychiatric treatment where substance use was not the primary diagnosis revealed a close relation between cocaine and crack use with the presence of risky sexual behavior for HIV ( Tolou-Shams, Ewing, Tarantino & Brown, 2010 ).
3. Risky behavior by type of severe mental illness
Some studies made in the United States have found a significant association between the greater severity of symptomatology in people with SMI and the greater amount of risky behavior ( Coverdale et al., 1997 ; Dévieux et al., 2007 ; Heaphy, Loue, Sajatovic & Tisch, 2010 ; Himelhoch et al., 2011 ; Meade & Sikkema, 2007 ; Rosenberg et al., 2001 ).
Different studies that compared the risk of HIV transmission in people with different kinds of SMI found the presence of greater risk in adult patients with some kind of organic mental syndrome ( Hellerstein & Prager, 1992 ) and less use of prevention strategies in people with schizophrenia ( Knox et al., 1994 ). They also found that people with mood disorders were more at risk than those with any other kind of disorders ( Abrantes et al., 2006 ; Guimarães et al., 2010 ; McKinnon, Cournos & Herman, 2001 ; Tubman et al., 2003 ). Patients diagnosed with depression were the ones proving to be more vulnerable to being infected with the virus ( Silberstein, Galanter, Marmor, Lifshutz, Krasinski & Franco, 1994 ). A recent study from the United States found that people with affective disorders were 4.07 times more at risk of contracting HIV in comparison with people diagnosed with schizophrenia ( Wu, Rothbard & Blank, 2011 ).
On the other hand, studies made in the United States and Italy found that people with bipolar disorders were more vulnerable to being infected with HIV than those with other disorders for five reasons: 1. greater frequency of sexual behavior than schizophrenic patients ( Raja & Azzoni, 2003 ) and those suffering from depression ( Sacks, Dermatis, Burton, Hull & Perry, 1994 ); 2. among women, more STI during their lifetime than unipolar depressive patients ( Meade & Sikkema, 2007 ); 3. greater seropositivity ( Henning et al., 2012 ; Volavka, Convit, Czobor, Douyon, O’Donnell & Ventura, 1991 ); 4. among adults of both genders, greater susceptibility to become infected by hepatitis C than people with depression or psychotic disorders ( Carey et al., 2004 ); and 5. a greater number of risk factors associated with HIV risk than people with other kinds of SMI ( Meade, Bevilacqua & Key, 2012 ; Sacks, Silberstein, Weiler & Perry, 1990 ).
A study about HIV transmission risk made in the United States with bipolar people found that less psychiatric severity, the presence of a recent manic episode and a greater frequency in the use of illegal drugs were significant predictor factors ( Meade et al., 2008 ). Another study made with people with bipolar disorders and HIV+ (where 91 had an affective episode before being diagnosed with HIV) reported that the presence of more manic and depression symptoms was significantly associated with unsafe sexual intercourse. Therefore, it is suggested that proper treatment to reduce the recurrence of affective episodes may reduce the frequency of risky sexual behavior ( Meade et al., 2012 ).
Sociocultural factors associated with the risk of HIV transmission
1. Risk vulnerability according to demographic context
Effects of poverty and indigence
Poverty has been researched very little in connection with risky behavior, and the risk differentials of people with SMI from different socioeconomic strata have been compared even less. The connection has epidemiological importance because mental illness has important economic consequences for families given the high cost of treatment and patient control. Furthermore, because it is associated with labor disputes and loss of employment ( Gianfrancesco, Wang & Yu, 2005 ) as well as with the deterioration of couple relationships ( Wright, Wright, Perry & Foote-Ardah, 2007 ).
A study carried out with migrant and non-migrant Hispanics in the United States found that poverty was an independent predictor factor of greater frequency of risky behavior for HIV transmission ( Heaphy et al., 2010 ).
Other studies investigated the risk among people with SMI in urban indigence situations and found a greater frequency of risky behavior among those in the general population ( Klinkenberg et al., 2003 ; Loue & Sajatovic, 2006 ; Susser, Betue, Valencia, Goldfinger & Lehman, 1997 ) as well as a greater probability of HIV infection ( Stewart, Zuckerman & Ingle, 1994 ). They also found that factors associated with HIV seroprevalence varied according to gender: with women it was the use of injected drugs and sex with injected drugs using partners, while in men it was the use of drugs injected with shared needles, sex with injected drugs using partners, and bisexual commercial sex behavior ( Silberstein et al., 1994 ).
Differences between urban and rural settings
Three studies made in the United States on the differences between risky behavior by people with SMI in urban and in rural settings had contradictory results. The first study showed that single men who had sex with men living in urban areas had more risky behavior than other urban and rural residents ( Brunette et al., 1999 ). The second study found that rural residents were more at risk than urban ones ( Rosenberg et al., 2001 ); and the third study found no differences between both settings ( Essock et al., 2003 ).
Differences by age groups
In terms of age groups, young people have been identified as the group most vulnerable to risk ( Brunette et al., 1999 ; Collins, Elkington, Von Unger, Sweetland, Wright & Zybert, 2008 ; Ramrakha, Caspi, Dickson, Moffitt & Paul, 2000 ). Two studies including people from the United States with SMI found that young people tend to be more sexually active and have risky behavior more often ( Hellerstein & Prager, 1992 ; Carey, Carey, Maisto, Gleason, Gordon & Brewer, 1999 ). Another study complementing the former found that risky behavior by teenagers increased as they aged ( Teplin, Elkington, McClelland, Abram, Mericle & Washburn, 2005 ).
Gender inequality and vulnerability
Two studies from the United States have described a greater frequency of risky behavior by men with SMI than by women with SMI even though there is a more frequent use of preventive strategies by men ( Knox et al., 1994 ; Sacks, Perry, Graver, Shindledecker & Hall, 1990 ). In Uganda’s population (18-49 years), females had higher risk of HIV infection than males (OR 2.10) ( Lundberg, Nakasujja, Musisi, Thorson, Cantor-Graae & Allebeck, 2013 ).
Other studies carried out in different contexts propose social factors that contribute to a greater vulnerability in women: unsafe sexual practices ( Guimarães et al., 2010 ), sexual intercourse with concurrent partners ( Chopra, Eranti & Chandra, 1998 ), a coercive context in relations with sexual partners ( Weinhardt et al., 2001 ), a greater prevalence of STI ( Meade & Sikkema, 2007 ), and the influence of conservative beliefs and attitudes towards procedures to modify risky behavior ( Otto-Salaj et al., 1998 ).
The factor dealing with the coercive context in relations with sexual partners is a pertinent condition for risky behavior by women with SMI. Prevalence of sexual abuse of people with SMI varies between 14% and 40% ( Collins et al., 2008 ; Coverdale et al., 1994 ; Coverdale et al., 2000 ; Randolph et al., 2007 ). Besides the inherent risk in sexual abuse that the perpetrators may be infected, studies made with United States adults and adolescents report that sexual abuse during the childhood of people with SMI is associated with a greater number of risky sexual practices and a greater probability of substance use ( Brown, Houck, Hadley & Lescano, 2005 ; Brown, Lourie, Zlotnick & Cohn, 2000 ; Dévieux et al., 2007 ). In Uganda it was reported that women with SMI had more sexual risk behavior and more sexual violence exposure than women in the general population. Sexual risk behavior was associated with HIV infection in men, but not women ( Lundberg, Nakasujja, Musisi, Thorson, Cantor-Graae & Allebeck, 2015 ).
Some studies have found that people experiencing some sort of physical, emotional or sexual abuse during childhood showed a greater probability of experiencing physical and sexual abuse when adults, had a larger number of sexual partners, applied fewer preventive strategies, practiced survival sex (sex in exchange of social and/or economic and/or physical protection benefits) and had a greater prevalence of STI ( Goodman & Fallot, 1998 ; Heaphy et al., 2010 ; Malow, Dévieux, Martinez, Peipan, Lucenko & Kalichman, 2006 ; Meade, Kershaw, Hansen & Sikkema, 2009 ; Théodore, Luna & Díaz, 2006 ).
In the case of men, studies propose different risk factors associated with HIV transmission: a greater number of sexual partners and use of substances during sexual intercourse ( Meade & Sikkema, 2007 ; Otto-Salaj et al., 1998 ), sex with partners who inject drugs ( Susser et al., 1997 ) and sexual intercourse with occasional partners ( Meade et al., 2008 ).
The differences in gender-based risk are influenced by the sexual culture ideology to which people with SMI belong. For example, a study of migrant Hispanic women in the United States showed that most of them described they had been raised in environments where “machismo” was the norm in the socialization of sexual roles, such as creating limiting effects on developing risk-preventive behavior based on interaction with their partner ( Collins et al., 2008 ).
As part of this sexual culture, there is a limited communication among Hispanic couples to agree on the use of condoms as a preventive measure for HIV. Here, there is as well a low assertivity level, especially in the case of women with a severe mental illness ( Gordon et al., 1999 ; Somlai et al., 1998 ).
Generally speaking, the studies show that the gender dimension is a constituent element of social relations based on gender differences ( Scott, 1986 ) and a structural component based on social inequalities ( Cerón-Mireles et al., 2006 ) that contribute to configuring vulnerability factors associated to the risk of contracting HIV, on health conditions, the characteristics of medical service use and commitment the treatment among people with SMI ( Collins et al., 2008 ).
2. Effects of social stigma
Stigma is a mechanism that interferes in social structures constituting communities ( Elgie & Morselli, 2007 ). It is not simply a product of cognitive processes but it rather exists and is perpetuated within a context of social inequality ( Hinshaw & Stier, 2008 ).
In this regard, stigma is a social construct shared by members of a community where it may produce and reproduce relations of power and control, injustice and social exclusion ( Smith, 2007 ). Therefore, stigma is an element that impacts the meaning that people with SMI attach to their daily practices within a sexual and preventive culture.
For people with SMI, the perception of the stigma of mental illness has been related to the development of restrictions to their sexual expression by feeling physically devaluated or undesirable ( Wright et al., 2007 ). There are studies showing a significant association between such perception and the risk of contracting HIV when people with SMI are sexually active.
Two studies made in Brazil and the United States ( Collins et al., 2008 ; Elkington, Mckinnon, Mann, Collins, Leu & Wainberg, 2010 ) agreed in their findings that the stigma of the illness was related to a discrimination process in the sexual behavior of people with SMI. Discrimination is expressed, on the one hand, in the difficulty to establish a stable couple relationship when the ill person feels rejected and devaluated because of his/her symptoms and due to the effects of his/her medicine; and on the other hand, by the tendency to have occasional sexual partners with limited possibilities to talk about using protection.
Despite the fact that discrimination facilitates the development of risky behavior, a study of the Afro-American population of the United States also detected that more empowered women try to lessen the negative effect of stigma. This strategy consists in projecting the image of a woman closely tied to religious values to facilitate a protective effect against risky behavior based on discrimination ( Collins, Von Unger & Armbrister, 2008 ). Another study made with Latina women living in the United States found that religious and spiritual beliefs had a positive influence in reducing risky behavior by providing them with a certain structure of everyday control and prevention when facing the typical disorganization and impulsiveness of people with SMI ( Loue & Sajatovic, 2006 ).
3. Communication about sexuality; a taboo in the institutional context
Sexuality and HIV/AIDS prevention are scarcely addressed by personnel of health institutions caring for people with SMI. Studies made in the United States reported that fewer than 20% gave direct information about this issue and fewer than 10% of the patients had asked for counseling. In a study from England, 40% said they had received information about HIV/AIDS from health providers. Most of the patients interviewed in the aforementioned studies said that they had obtained more information from other sources ( Coverdale & Aruffo, 1992 ; Coverdale et al., 1994 ; Ngwena, 2011 ).
In the context of scarce institutional information about sexuality, one aspect that is rarely addressed in healthcare is the effect of medicine in general and particularly on sexual behavior. A research carried out at United States’ institutions found that the issue was seldom talked about even though 62.5% of the male patients and 38.5% of the female patients reported having had effects from the medicine. The main reasons for not talking about the issue were: lack of confidence in the physician, and the idea that nothing could be done to avoid the effects ( Rosenberg, Bleiberg, Koscis & Gross, 2003 ).
Studies made with healthcare suppliers for men and women with SMI in Africa and the United States ( Pinto et al., 2007 ; Collins, 2001 ) found two obstacles to counseling on HIV/AIDS transmission and prevention: 1. stigmatization of patients’ sexuality as promiscuous and risky behavior; and 2. the idea that risky behavior was only a normal reflex of the illness.
One study in Brazil found a high HIV seroprevalence and correlations of infection were not found to include psychiatric diagnoses or hospitalizations, but instead it reflected marginalized living circumstances and HIV testing history. These adverse life circumstances (history of homelessness, having suffered sexual violence, reporting a sexually transmitted disease, and early sexual debut) may not be unique to people living with mental illness but nonetheless the mental health care system can serve as an important point of entry for HIV prevention in this population ( Guimarães et al., 2014 ).
Discussion and conclusion
Evidence of high HIV infection rates in the population of people with SMI ( Joska et al., 2008 ) has bolstered researches of the factors associated with the risk of transmission in different parts of the world, mainly in more economically developed countries.
This review described findings of individual and sociocultural factors separately. The most noteworthy detected individual factors are: a lower level of knowledge about HIV/AIDS than the general population; the presence of mistaken beliefs about the transmission mechanisms and types of prevention; greater frequency of risky behavior than in the general population; and a greater extent of risky behavior when the person with SMI displays a more severe symptomatology ( Gordon et al., 1999 ; Ngwena, 2011 ; Stevenson & Eilers, 1992 ).
Furthermore, the detected sociocultural factors included: poverty and indigence associated with greater frequency of risky behavior; greater vulnerability of women and young people due to the negative influence of coercive sexual cultures, negative effect of the perception of social stigma of mental illness and unsafe sexual behavior; and scarce institutional coverage in sexual health and HIV/AIDS prevention programs.
The separation enables one to analyze the diversity of results in the reviewed studies, even though they should be considered interrelated for a comprehensive interpretation of the phenomenon of vulnerability to the risk of contracting HIV, as proposed in the synthesis of figure 1.
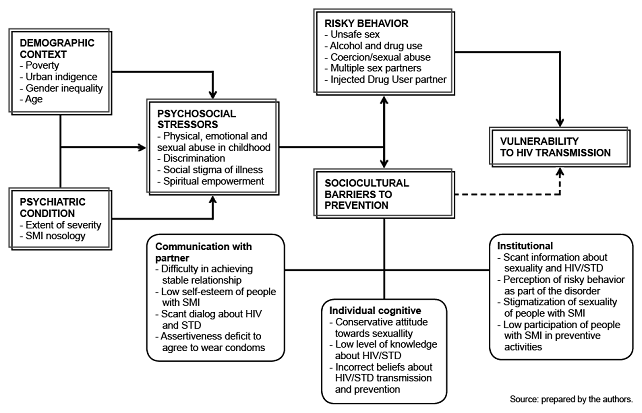
Figure 1 Synthesis of individual and sociocultural factors associated with the vulnerability to the risk of HIV transmission in the Severe Mental Illness population. The arrows indicate the direction in terms of influence of some factors over others and dotted arrows show factors related to sociocultural barriers as indirect determinants of vulnerability. Nevertheless, these barriers also show ties to and determine the context of risky behavior.
As shown in the demographic context and the psychiatric condition –apparently distant factors associated with the risk of contracting HIV– are closely related to the vulnerability of the population at issue. Figure 1 shows how these two factors include some psychosocial stressors identified in the studies and in turn have been associated with sociocultural barriers to prevention, and with the context of risky behavior for HIV transmission.
Based on the findings about risk-related factors, a provisional hypothesis can be made of the greater vulnerability to the risk of contracting HIV/AIDS in people with SMI than in the general population. Also that vulnerability of people with SMI is differential in terms of sociocultural determinants and individual factors associated with HIV transmission.
The hypothesis about the vulnerability of people with SMI can be appreciated in the light of the limitations of the studies included in this review. The main limitation lies in the fact that 88% of the studies were cross-sectional quantitative. In this regard, the main limitation of the studies included is that they approached the subject of their study at one moment in time and lost sight of the longitudinal processes that are fundamental to providing explanations of vulnerability based on the interaction of factors associated with risky practices.
Although most studies included multivariate analyses to evaluate the association hypothesis, their variables dealt with theoretical psychosocial and biomedical approaches emphasizing individual behavioral attributes. In the case of qualitative and combined studies (only 12% of the works included), they were also cross-sectional researches with sociological and anthropological approaches aimed at understanding sociocultural behavioral attributes within specific settings.
The contents of the findings also suggest that there are some aspects that should be investigated more in depth in cross-sectional and longitudinal studies: a) the differences in risk vulnerability in urban and rural settings in several age groups and between genders, implying studies aimed at learning normative constructs of sexuality and risks for the female and male genders, and at different socioeconomic strata; b) the constrictions of sexual culture based on violence and coercion in different social contexts; c) the effects of the perception of stigma and discrimination in the development of risky behavior; and d) the development of social and individual empowerment processes as protectors against risk. Generally speaking, the study of other aspects should combine individual and sociocultural factors and include as well the interaction of sexual partners and substance use as a unit of analysis that transcends the individual level.
With regards to vulnerability differences, it is necessary to underscore the absence of studies focused on the culture that works from a gender perspective. Theoretical studies of male roles and masculinity that have appeared in some of the cases or contemporary feminism propose transcending a monolithic vision that only addresses the study of women and their experience of oppression to an integrating vision that implies studying masculinity ( Gardiner, 2013 ). Olavarria (2003) proposes in turn that masculinity has to be seen as part of gender relations where both categories are heuristic and their study offers the following advantages: it allows one to understand individually as well as socially the history and structures where gender is organized under systems of social differentiation such as class, ethnicity and generation. It is advisable to use qualitative methodologies focused on gender analysis.
These findings have implications on clinical intervention. It should be mentioned that some studies express the need for psychiatrists and other mental health professionals to provide information and training in sex health matters. This will not only have a positive effect on prevention but also on expanding services related to early detection and appropriate care in this population.
Senn and Carey (2008) document that intervention programs implemented to prevent the risk of sexual transmission of HIV in the SMI population have emphasized modifying individual behavioral factors (motivation, attitudes, self-help systems, the ability to wear condoms, and assertiveness). The most efficient programs with this intent were those including attitude, motivation, and skill development components with material written in appropriate language for the group. Nevertheless, a major limitation was a short-term evaluation of change of individual variables by means of nonrandom designs. Due to the limitations of these programs, the authors propose the need to complement them by implementing programs aimed at modifying social prevention norms based on sociocultural factors.
In our review, we found different individual and sociocultural factors associated with risk that should be modified for the purpose of designing and implementing preventive programs under a structural approach: gender inequity, socioeconomic inequality, coercive sexual culture, discrimination, the perception of stigma and the consumption of illegal substances ( Gupta, Parkhurst, Ogden, Aggleton & Mahal, 2008 ).
This review enabled us to identify individual and sociocultural factors associated with the risk of people with SMI contracting HIV. The combination of these factors allows us to conclude that the SMI population is more vulnerable to the risk of contracting HIV than the general population and such vulnerability is differential in terms of closely related individual and sociocultural factors that could be modified by structural preventive programs. Most of the studies reviewed were cross-sectional (88%), and it would be advisable to perform longitudinal or more rigorous design studies to support the hypotheses and conclusions we reached about the vulnerability of people with a severe mental illness from the risk of HIV transmission.

