











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkBackground
Salt or sodium chloride is probably the oldest spice used by man. Its extraction, distribution, and possession led to commercial trades and wars, to the point that it was known as "white gold". It is possible that primitive man found the properties of salt when he established contact with thin salt deposits left on the beach by the sea water. After that, he created his own sea water ponds that would leave small amounts of salt when water was evaporated by the sun; just as happens naturally in places far from the sea where the salt source was probably springs where briny water rose and left some salt when evaporated. In this way he could supply his own needs. These were also excellent places for hunting because different animal species gathered there with the same urge.1
When more advanced instruments were developed, early civilizations extracted "halite": the solid sedimented form of salt, from mines. Man also created commercial routes to distribute it to a large number of human sites where salt could be well traded for its weight in gold. In Ancient Greece and the Roman Empire, salt could be used to buy slaves, for tax payment, and as a part of the labour payment, which was called salarium and originated the word 'salary'.1-3
Ancient civilizations took advantage of salt's ability to dry out and cure food so that it could then be transported over long distances and rehydrated for consumption; this played a significant role in aiding long-distance travel and exploration.2
Nowadays salt is used as a meat tenderiser, agglutinating agent, and food additive to give a more attractive taste to food in general. In baking, it is used to correct flavour and control dough fermentation. In dairy products, it controls fermentation and enhances the colour, texture and flavour of preparations.
In industrial areas salt is used to produce chlorine (Cl-), caustic soda, and in the manufacture of plastic, colorants, pesticides, and drugs. It has been used in leather because of its disinfectant properties and in energy source exploration, such as oil, gas, and water treatment.
In the human body, sodium is important to maintain fluid balance and blood pressure, muscle contraction, nerve cell transmission, and most cell functions. Its consumption is so extended that it is added to other nutrients with lesser dietary distribution such as iodine, to avoid its deficiency in the general population.1,2
Suggested sodium intake and actual consumption
According to the World Health Organization (WHO) and other international bodies, the Tolerable Upper Intake Level (UL, the highest daily nutrient level intake that is not likely to pose a health risk) is 5 grams of salt ˗one teaspoon˗ or less than 2,300 mg of sodium per day (1 gram of salt = 390 mg of pure sodium) for the general population and less than 1,500 mg of sodium for those who have hypertension (HT), diabetes, chronic kidney disease, and for black ethnic groups.4-7
On the other hand, the Adequate Intake of sodium is smaller and depends upon age (Table 1), being higher in people between 9-50 years old (1,500mg of sodium) and declining as age increases.8 (Adequate Intake, or AI, is the recommended daily intake of a nutrient based on the amount needed to meet the sodium needs of healthy and moderately active individuals, including sodium sweat losses in those exposed to high temperatures).
Table 1. Daily sodium recommended intake according to age
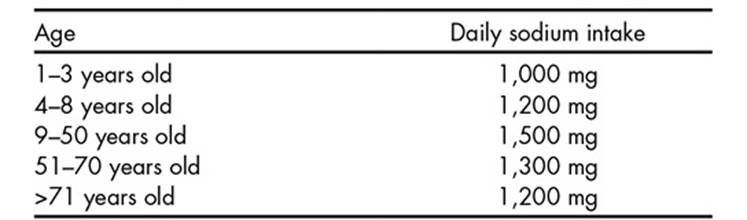
Source: Dietary Guidelines for Americans 2010 USDA.
Studies like Health Canada and INTERSALT were conducted to calculate the amount of dietary sodium in different communities, and even though the salt intake percentages varied between groups, every one of them exceeded the limit for daily ingestion. On the basis of the INTERSALT study, which measured urinary excretion of sodium in 24 hours in men and women between 20-59 years old around the world, it was found that almost 50% of women had 5.9-8.8 grams of salt per day and more than 50% of men consumed 8.8-11.7 grams per day.4,9 The Centers for Disease Control and Prevention (CDC) report an average daily sodium intake of 3,400 mg in the North American diet.5
Main salt sources
The proportion of salt in the diet is as follows: 12% comes naturally in food and only 11% is added by seasoning during cooking or at the table.5,10 Therefore, more than 75% of salt comes from processed food.
In a modern diet, the major proportion of sodium comes from industrialised and processed food (instant soups, junk food, canned and frozen food, sausages, crackers, cereals, sweet beverages, salted meat, pickled foods),10 so adding salt while cooking elevates its already high levels.
The food category with the highest sodium content (Table 2) is processed meat (with an average content of 1,100mg of sodium per 100 grams of meat)11 but the largest amount of sodium in diet comes from food that might not even taste salty: grain-based foods (soups, pastas, breads, cakes, cookies, and crackers) from which the most daily calories are consumed, followed by meats.12
Table 2. Average sodium content in packaged foods

Modified from Korošec Z, Pravst I. Nutrients 2014, 6.
A part of dietary sodium is also found as monosodium glutamate (MSG), which has the property of enhancing food flavour.12,13 It is found naturally in animal products and in a lesser proportion in some vegetables. It is widely used by the food industry in soups and broths, sauces and gravies, and canned or frozen meats, poultry, vegetables, and combination dishes. MSG contains 12.3% of sodium, and as the usual MSG use is around one tenth of that of salt, MSG contributes to 7-8% of dietary sodium.14 Its chronic consumption has been associated to β-amyloid accumulation in the brain, neuropsychiatric disorders, and neuronal loss, while acute ingestion has been related to vomiting, headache, nausea, and chest pain among other symptoms sometimes known as "Chinese restaurant syndrome", but evidence is not totally clear.14-17
Salt perception in the gustatory system
Through chemoreceptors located in taste buds, the tongue is responsible for perceiving flavours along with the olfactory system. The receptor for salty taste is activated by food with ionized salts, especially sodium. The umami ("delicious flavour" in Japanese) taste is perceived by receptors for amino acids like glutamate (in MSG) and aspartate and by nucleotides; it induces a pleasant sensation in other flavours.18
The chorda tympani branch of the facial nerve (cranial nerve VII, CNVII) innervates the anterior two thirds of the tongue, which is the zone with highest sensitivity to sodium because of its large amount of receptors. The glossopharyngeal nerve (cranial nerve IX, CNIX) innervates the posterior third, which is less sensitive to salt. The vagus nerve (cranial nerve X, CNX) innervates taste receptors in the epiglottis epithelium, responsible for regulating diuresis and plasma tonicity. Even though the anterior two thirds are more sensitive to salt, when NCVII is sectioned, the posterior third gets a higher sensitivity to salt perception through neuronal plasticity mechanisms, so salt consumption is always regulated.14,19,20
Gustatory signals pass through a totally ipsilateral pathway through the geniculate (NCVII) and inferior sensory ganglion (CNIX and CNX) to stimulate the second order neurons in the rostral portion of the solitary tract nucleus (the gustatory nucleus of the solitary tract complex) in the lower medulla. These neurons stimulate thalamic nuclei that project to the primary gustatory cortex - the inferior gyrus of the frontal lobe and anterior insula - and secondary gustatory cortex - the orbitofrontal cortex (OFC). As the sensation of flavours results from gustatory, olfactory, and somatosensory inputs, the cerebral cortex mediates the appreciation of tastes.19
Physiological aspects of salt addiction
Flavour information from cortical taste areas exerts strong influence on the lateral hypothalamus (LHT), which has a role in the generation of autonomic responses associated with ingestion and digestion. The taste cortex also projects directly to the amygdala and ventral striatum (nucleus accumbens, NA).19,20
Therefore, salt intake (as with fat, sugar or caffeine intake) induces activation of LHT that releases dopamine and glutamate in the ventral tegmental area (VTA)21 and in turn it stimulates the NA and other limbic system structures provided with dopamine, endogenous opioids, and cannabinoid receptors. Limbic structures feed back to the medial prefrontal cortex and OFC, a pathway traditionally recognised for its role in reward, pleasure, consolidation of habits, learning, and memory22-25 (Figure 1). These observations correlate with the lack of addictive behaviour for food when naloxone or neuroleptics (antagonists of opioid and dopamine receptors respectively) are administered.26,27
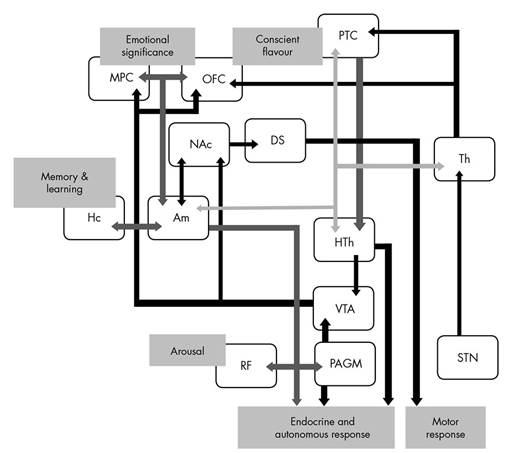
Figure 1. Taste signals from tongue get to the solitary tract nucleus (STN), it stimulates thalamus (Th) that project to primary taste cortex (PTC) and orbitofrontal cortex (OFC). PTC activates lateral nucleus of hypothalamus (Hth) to cause an autonomic response to food intake, it also activates ventral tegmental area (VTA) that releases dopamine in ventral striatum or nucleus accumbens (NAc), which connects to dorsal striatum to produce a motor response to emotions, NAc also stimulate amygdala (Am), that has reciprocal connections with medial prefrontal cortex (MPC), OFC, PFC, hippocampus (Hc), Th, Hth and stimulate inferior structures like reticular formation (RF) and periaqueductal grey matter (PAGM).
Substance-related obsessive thoughts and compulsion to consume are important characteristics of food and drug addictions. The activity of OFC has been implicated in impulsivity and the pathology of obsessive-compulsive disorder.27-30
Many authors are now using the term "food addiction"31-33 because of the similarity of this response and the mechanisms stimulated by drugs of abuse such as amphetamines and cocaine,34-38 which explain or support the hypothesis of an addiction produced by chronic consumption of savoury food. It seems clear that food cravings can occur in the absence of a nutritional deficit and flavour seems to be an important factor in the satisfaction of food cravings.39 Also, it has been found that repeated consumption of a certain food when hungry ˗but not when satiated˗ produces cravings for that substance after its withdrawal,40 suggesting that the gustatory system and learning processes are directly implicated in food addiction.41
Concurrently, excessive ingestion of these foods and obesity are associated with lower expression of dopaminergic D2 and opioid µ receptors,42 consistent with a long-term reduction of sensitivity of reward centres of the brain (down regulation of receptors); this could explain the apparent tolerance due to excessive and continuous intake,23 just like what happens with other addictive substances. The origin of this series of events is not clear; whether desensitization originates from, or is a result of over-stimulation of dopaminergic receptors, due to salt ingestion. It is evident that a greater amount of salty food is progressively needed to get the same gratifying response (tolerance),43 therefore it turns into a vicious circle, requiring larger quantities of food. Eating more food also increments the amount of fats, carbohydrates and other nutrients that favour an increase in obesity.44
Behavioural aspects of salt addiction
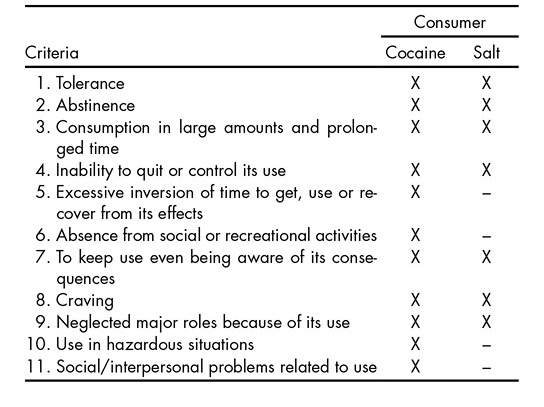
Although sodium intake shares neuronal networks and pathways with drugs of abuse,36,37 it is important to classify salt as a substance of abuse through clinical features in the same way as psychoactive drugs. The Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) identifies substance abuse and dependence as "Substance Use Disorders" (SUDs) and points out that it is necessary to accomplish two or more of 11 criteria within a 12-month period to diagnose it. In most cases, salt consumption fulfils at least seven of these (Table 3).43,45-47
Table 3. Behavioural criteria for Substance Use Disorder (SUD) that compares cocaine and salt consumers according to DSM-5
One of the most important SUD criterion is abstinence that dependent people present when salt is withdrawn from diet; as anorexia, anxiety, slight nausea during meal time, the need for and seeking out of the substance, etc. It is known that patients under hospital assistance present a low acceptance for food,48 often complaining about finding it tasteless and the lack of salt in their diet.
The massive and life-long use of sodium in food and the lack of success in dietary salt restriction despite the many public health campaigns and recommendations supports its classification as a clinical addiction.43,45,46
Craving is the strong urge to consume a certain substance; the most frequently craved food is chocolate, followed by pizza, salty foods, ice cream, and other sweets and desserts.49 The inability to fulfil major social roles (school, work, or home obligations) could happen due to its long-term health consequences (cardiovascular disease, chronic kidney disease, morbid obesity).46
Some criteria refer to significant time invested in seeking, reaching and consuming the substance; however, absence from social activities and interpersonal problems are not likely to be covered by salt addiction due to the easy access to the substance and the social acceptance of its use.43 Use of the substance in hazardous situations is often referred to in substance intoxications, such as driving under the influence of alcohol, which is not seen in this case.46
Health consequences of salt addiction
A high sodium intake increases urinary calcium excretion and bone resorption markers in plasma which is associated with bone loss and a lower bone density, an effect that is more evident in those with a low calcium diet.50,51
Another result of high sodium ingestion is a major consumption of liquids and other nutrients such as carbohydrates and fats, leading to obesity, which is accompanied with a rise in leptin (a satiety inducer hormone) and insulin concentrations.52,53
Insulin and leptin resistance results in an increased salt sensitivity that predisposes a rise in BP due to high sodium intake, probably due to sympathetic and adrenal dysregulation.54-57 Many studies have demonstrated a clear link between high salt intake and increased BP: The INTERSALT study showed a relation between salt and increase in BP, demonstrating that in subjects who ate more than 6 grams of salt per day for more than 30 years, systolic BP was 9 mmHg higher than in people with lower salt intake.9 Another meta-analysis proved that a restriction of salt consumption to less than 6 grams decreased systolic BP in 4-7 mmHg in hypertensive patients and 2-4 mmHg in normotensive patients.10
Lowering dietary sodium is an important part of treatment in HT and helps to decrease the risk of cardiovascular disease such as left ventricle hypertrophy, peripheral arterial damage, cerebrovascular disease and heart failure.5,8
Renal function, responsible for regulating the concentration and intravascular volume of sodium, is impaired in response to large loads of sodium by the effects of angiotensin II, aldosterone, growth factors, reactive oxygen species (ROS), sympathetic hyperactivity, and direct vascular damage due to HT. This has effects throughout the kidney economy (vessels, tubules, juxtaglomerular apparatus, myocytes) impairing its autoregulatory capacity, evidenced by proteinuria, HT and renal fibrosis, becoming a positive feedback pathophysiology.58-60 This is why high sodium diets increase the risk of developing kidney disease, and independently increases mortality rates in patients with kidney disease, and low sodium diets decrease proteinuria in patients with HT.61,62
Salt addiction as a public health problem
The modern world involves a faster pace of life and therefore an increase eating fast food and industrialised food. These are filled with large amounts of sodium and are directly related to an increase in obesity rates, especially in high-income countries.11,63,64 Taking into account the addictive effect, neuronal changes, and other health consequences chronic salt consumption can produce, it can be catalogued as a pandemic.
Excessive salt intake contributes to 10% of cardiovascular disease, it is one of the main causes of increased BP and causes more deaths than other food-related factors, compared to high trans-fat consumption, alcohol ingestion, and low intake of fruits and vegetables.65,66,67 It is also common for young people to prefer salty food, resulting in a major development of HT and other conditions at an early age which, when coupled with the global tendency of greater life expectancy, translates as an important problem for international economy and health professionals.41,68,69
Due to its relation to addictive behaviour, obesity, HT and other conditions, governments around the world and global organisations should give the population clear and practical recommendations about sodium consumption and closely regulate the food industry about salt and monosodium glutamate use, distribution and labelling.69
Discussion and conclusion
There is certainly a need to go into depth about the mechanisms implied in reward pathways that may turn food into addictive substances and methods to effectively stop or revert them.
Currently an important number of researchers consider excessive sodium consumption an addiction.31-33 It is important to assume that salt is categorically an addictive substance just as psychotropic drugs, as they share cerebral pathways that perpetuate their excessive consumption. Salt intake implicates more than just a preference for salty taste but further studies must be conducted in the future to clinically define the precise concept of salt addiction.
The large number of patients with obesity, cardiovascular disease, and renal substitutive treatment is an important warning, because if these diseases do not get appropriate treatment and control, they will continue causing incapacity and death all around the world.
Accomplishing dietary sodium recommendations is a challenge: the population at large is exposed to large amounts of salt and people ignore the amount of sodium in their diet, because most of it is previously added during processing and hidden in non-salty foods like breads, desserts and soft drinks.

