











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Since 2008, U.S. immigration policies have emphasized deportation, a type of forced return migration of unauthorized and criminal aliens.(1) Between 2008-2011, 1 million Mexicans have been deported.(2) Most migrants deported from the U.S. are Mexican nationals (86% in 2010),(3) and many are returned to border cities such as Tijuana, Baja California, adjacent to San Diego, California. Tijuana is a major deportee receiving community: more than 100 000 persons are annually returned to Mexico via this border city.(4,5)
Despite the high volume of deportees returned to Mexico, little is known about the health consequences of this type of forced migration. This situation creates an opportunity for studying the conditions of deportation,(6) and by extension, the post-deportation experience.
Migrants may be deported from the U.S. for numerous reasons: some are detained while crossing the border, whereas legal permanent residents who violate immigration laws or have legal offenses may be expelled after many years of U.S. residence.* Ruben et al.(7) conceive return migration as a complex multidimensional process that may be equivalent to arriving in a new place, so the need to acculturate to a new context. Acculturation is considered to be a multi-dimensional process in which individuals and groups undergo stages of adjustment in several domains: language, socioeconomic status, social networks, cultural orientation and status, as they adapt to a new cultural environment.(8) This process may result in a phase of acculturative stress,(9,10) which is conceptualized as the sum of factors that contribute to the subjective experience of this transition.**,(11,12)
Prior studies have documented an association between higher acculturative stress and a poor health status (e.g., anxiety, depression, feelings of marginalization and alienation, increases in psychosomatic symptoms, identity confusion).(9,13-15)
Different pathways have been identified as migrants cope with the demands resulting from adaptation to a new environment.(16) Early acculturation research focused on studying the individual characteristics,(17,18) while recent research considers eco-developmental contextual variables (e.g., social networks, neighborhood resources, racial/ethnic discrimination),(19) which can greatly influence an individual's acculturative trajectory.(20) Thus, some(21) suggest analyzing not only individual-level influences (e.g., psychological well-being, perceived discrimination), but also contextual-level factors, including social capital.(22) Social capital refers to all cooperative, trusting and reciprocal social relationships, and community resources,(23-26) which promote sociocultural adjustment and thus relieve the acculturative stress.(23-27)
Given the dearth of research on deportation and its implications for the health and well-being of migrants, this exploratory qualitative study describes women's experiences in and adaptation to the post-deportation environment; we propose these are their "acculturative trajectories". We also describe instances in the post-deportation environment that may reflect a vulnerability to risk behaviors. Our study may inform areas for future research in a larger population of female deportees.
Methods
Study population & recruitment
The present study is a secondary analysis of the longitudinal cohort study "Proyecto El Cuete" (cuete is 'slang' for syringe in Tijuana, and it also means to be drunk or high) of HIV-related risk behaviors and co-morbidities among IDUs living in Tijuana, Mexico. As previously described,(28) participants ≥18 years old with evidence of recent injection drug use were recruited into a prospective study using respondent-driven sampling.(29) For this cross-sectional sub-study focused on deportation and potential implications for drug use and HIV risks, we first generated a list of IDUs in the prospective study which reported deportation from the United States. Of the 1 056 study participants, <15% (N = 157) were women, 36 of whom reported being deported from the U.S. In October 2008, outreach workers invited all women who were not lost to follow-up (i.e., moved away, deceased, or could not be located) to participate in the study (n = 12). After undergoing voluntary and informed consent, 12 women underwent one-time qualitative interviews and were reimbursed U.S. $20 for their time. The Human Research Protections Program of the University of California, San Diego, and the Ethics Board of the Tijuana General Hospital approved the study protocols.
Research design
The design was based on constructivist epistemology where a feminist theoretical perspective was adopted. Constructivism states that meaning is constructed not discovered; thus, subjects construct their own meaning in different ways, even in relation to the same phenomenon. Hence, multiple, contradictory but equally valid accounts of the world can exist. Secondly, using gender perspective as an analytic tool(30) (not as substitute for women's history), allows us to better understand women´s experiences and testimonies from their standpoint.(31,32)
Qualitative interview data collection
Between October and November 2008, trained bilingual interviewers conducted semi-structured interviews in private interview rooms in Tijuana's zona roja (red light district). Interviews were conducted either in English or Spanish according to women's preferences and lasted 1-2 hours. Women were queried on their migration, deportation, drug and sex experiences in the United States and Mexico, and they responded to a broad range of questions such as: "Please, tell me why you were deported from the United States," "Tell me about your drug use in the United States," "Describe what happened the last time you were deported" and "What has your life been like in Tijuana?" Interviewers asked women to focus on their most recent deportation because many experienced multiple deportations. Questions were generated in part based on published studies with Mexican migrants in the U.S.(33,34) Interviews were digitally recorded and transcribed. All transcripts were analyzed in the language of interview in order to preserve participants' means of expression, which was often bilingual and contained terminology specific to the local economic and drug subculture of Tijuana.
Approach to qualitative data analysis
The interview data was analyzed using grounded theory methods(35) and context-driven methodology(36) to discover underlying concepts and to understand or interpret each participant's narrative.
A list of codes that would enable the researchers to categorize the interview data based on topics included in the interview guide (i.e., a priori codes) was developed. The list of codes also included emergent codes which were created based on the reading of the transcripts and which were reflective of acculturative stress and social capital concepts. Specifically, based on previous literature,(22) a consensus list of codes for acculturative stress indicators was built and included: lack of control, financial stress, feelings: depression, loneliness, frustration; lack of social support; and lack of formal ways to earn a living. The same procedure was followed to identify post-deportation social capital resources; these included the following codes: family bonding, social support, community resources. Next, the researchers read several cross-sections of interviews, revising the coding scheme as necessary. The first author, co-author, and Principal Investigator discussed and resolved discrepancies by refining code definitions. Throughout the analysis, emergent themes were discussed and illustrative quotations of key concepts were compiled. All coding of transcripts was done by hand. All Spanish language quotes were translated into English by the first author for brevity.
Results
Participant's characteristics
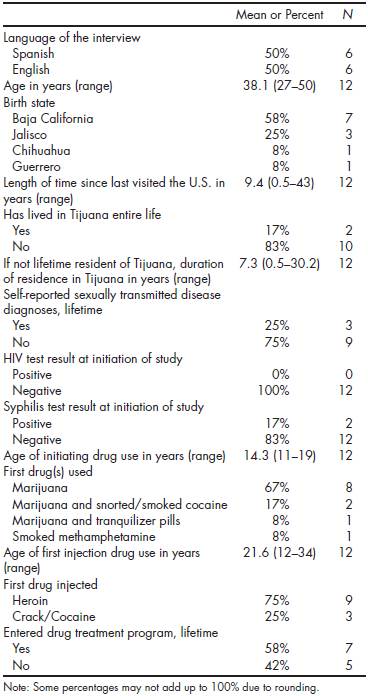
The participants' ages ranged from 29 to 53 years, with a median of 38 years at the time of the interview; six women were interviewed in English; and the other six in Spanish. The age in which women migrated to the U.S. ranged from <1 year to 20 years; the median age of U.S. migration was 10 years. Interviews occurred four to 10 years since women's last deportation; on average, participants resided in Tijuana for five years since their last deportation. All participants used drugs in the U.S.; 83% started to inject drugs in the U.S. between the ages of 17 and 27 years. None of the study participants tested positive for HIV at the time of the parent study's baseline interview. All participants had felonies or misdemeanors related to their drug use, as well as other felonies/misdemeanors (e.g., illegal residence in the U.S., drug dealing, armed robbery, domestic violence and murder). Most women spent time in jail and were deported soon thereafter. Three-quarters of participants reported any lifetime experiences in drug rehabilitation programs, with an abstinence period that varied from three months to 10 years (Table 1).
Acculturative stress post-deportation
On average, the 12 women resided in the U.S. for 25 years; the range of residence in the U.S. was from nine to 35 years. Women reported limited contact with Mexico prior to their deportation. Below, we discuss emergent themes related to acculturative post-deportation stress that were identified in women's narratives, highlighting several examples using women's voices. Generally, women experienced an overwhelming affective experience (e.g., intense and painful emotions, such as anxiety, fear, sadness) that may have interfered with their problem-solving and judgment capabilities and which may have made them vulnerable to abusive experiences. For all women, the immediate experience after being released in a Mexican border city was overwhelming, as one expressed: "[...]when I saw myself in Tijuana, it drove me crazy!!! [...]It really messes with your mind 'cause what am I gonna do, how am I gonna pay this?" (41 years old, resided in the U.S. since age 10, was deported three months prior to the interview). The affective experience appeared to interfere with female deportees' capacity to solve problems and seek alternatives; most participants expressed that they felt paralyzed and found drug use to be their only option: "I got drunk [...] I was paranoid. I was scared, so I just stayed there (in a hotel in Tijuana)[...]" (36 years old, resided in the U.S. since age two, was deported four years prior to the interview). Another participant recalled: "I was very scared, a guy offered me drugs so that I could calm down" (53 years old, resided in the U.S. since age three, was deported two years prior to the interview). The emotional impact of the deportation process also seemed to increase female deportees' vulnerability to abusive experiences, as one woman narrated: [...]after being deported I felt sad and scared, an old man approached me and told me he was going to help me[...] but he kidnapped me[...] he started to inject heroin in my arm so that I could be sold as a prostitute" (31 years old, resided in the U.S. since age 15, was deported six years prior to the interview).
Social and economic adaptation to deportation
Following their deportation, women generally reported a dearth of social and economic resources. Six female deportees stayed with other female deportees following their repatriation and rented a room; other three were homeless and stayed on the streets as they waited for their families to send them money; three accepted shelter from men who offered them assistance. Women often found themselves in Tijuana, a foreign city, and Mexico, a country where they had not lived for many years. Women reported that the stigma of being a deportee was equal to being perceived as a criminal; feelings of stigmatization were amplified by the track marks (i.e., injection stigmata) resulting from their drug use. These factors reportedly made that our sample of female deportees who are IDUs vulnerable to discrimination and constant police harassment.
The lack of financial resources following their deportation became an important stressor. Most women had limited amounts of money at the time of deportation and some were helped by their families. However, over time, they found that employment in the formal economy and, more generally, income-generating opportunities were limited. One factor that complicated women's access to employment opportunities and their integration to the Mexican society was their lack of access to an official government identification. Notably, most participants lacked legal documents to establish their identity as Mexican nationals. Consequently, women typically worked in the informal economy as waitresses, dancers, shoe shiners, and some women established relationships with people who took care of them. All participants engaged in sex-work in order to earn money: "[...]I had to sell myself because I didn't have money to survive" (52 years old, resided in the U.S. since age 10).
Long-term adaptation: developing post-deportation social networks
Following their deportation, female deportees described building social networks, mainly with other IDUs in Tijuana. Nearly all women (92%) established romantic relationships with other drug users in the immediate post-deportation period. As one woman narrated: "In the border I met a guy who offered me drugs[...] he became my partner, we have fought for drugs, he even has sent me to other males in order to bring him drugs" (39 years old, taken to the U.S. by her husband at age 20, was deported 10 years prior to the interview). Another participant expressed: "[...]I got involved with this guy, as addicted as me to drugs, and it has been a life of suffering, he messes with my plans, and I can't get rid of him, because he threatens me[...]" (40 years old, migrated to the U.S. at age 12, was deported three years prior to the interview).
Chronic mental health problems
Women's narratives suggest that their mental health was compromised, since all women reported "negative affectivity" (i.e., a general disposition to experience negative mood states: fear, sadness, guilt, hostility, fatigue, shame, irritability, distress)* that contributes to their cycling between sobriety and drug addiction. As one narrative exemplifies: "[...]the more sober you are, the more pain you feel in your heart, and by using [drugs], it numbs the pain" (38 years old, taken to the U.S. at one month, was deported five years prior to the interview).
Sex work further compounded women's negative affectivity: "[... ]I felt dirty, because I was selling my body, I never thought that I was going to do this, I had a perfect life, and that's one of the reasons why I started using heroin: To deal with the fact that I have to have somebody getting on top of me for money" (36 years old, taken to the U.S. at age two, was deported four years prior to the interview). We found also a pattern of negative self-criticism and shame related to their drug use that in turn influences their social relationships: [...]You know, I could get in touch with my family, but I feel so ashamed if they found out that I'm in heavy drugs" (39 years old, taken to the U.S. at age 20 by her husband, was deported 10 years prior to the interview).
Social capital
Loss of family networks
All participants belonged to an extended family (i.e., husband, children, parents, uncles, cousins) that lived in the U.S. All women had trouble with their family members while they lived in the U.S. due to their drug use. Nevertheless, women's families continued to support them in their daily living (e.g., paying rent, taking care of their children, bailing them out of jail, enrolling or financing rehabilitation programs, among others). All participants' families were interested in helping them in the post-deportation period: some sent money or searched for them in Tijuana and helped to situate them in a safe place. As one woman narrated: "My family came to look for me, they had flyers with my picture everywhere in Zona Norte [Tijuana's red light district near the U.S.-Mexico border], and they actually found me that same day" (53 years old, resided in the U.S. since age three, was deported two years prior to the interview). However, when women got involved in drugs and sex-work, most female deportees became isolated from their families: "When I started using [drugs], what my mom used to send me wasn't enough, I started working in bars, and then I lost communication with my family, I don't know where they're at, they don't know where I'm at" (36 years old, taken to the U.S. at age two, was deported four years prior to the interview). Negative affectivity in relation to women's drug use was reported as a central factor leading to women's isolation from family networks:
Post-deportation access to non-governmental and governmental programs
Women knew of some programs that provide condoms, HIV testing, or syringe exchange. Other non-governmental programs provide women with shelter and food, and one participant reported that an organization had helped her to re-establish contact with her family and supported her with employment options: "I was in this shelter where I felt safe; they provided me with food and employment options, and also were interested in locating my family again to remain in touch" (53 years old, resided in the U.S. since age three, was deported two years prior to the interview).
Discussion and conclusion
This exploratory qualitative study describes women's experiences in adapting to the post-deportation environment, specifically in the U.S.-Mexico border city of Tijuana. While none of the participants in this study tested positive for HIV at the baseline interview, the data nevertheless provide insight into moments in the post-deportation environment that may rise female deportees' risk for HIV. To understand Mexican women's post-deportation experiences, we found that participants' acculturative trajectories(20) to life in Tijuana are complicated by several issues, including affective reactions to the deportation process and social barriers to resettlement. These women's local and personal experiences should be seen as both global and political experiences.(31,37)
Our data suggest that the deportation experience creates an affective reaction that may increase the likelihood that women will engage in high-risk behaviors (e.g., drug use, unprotected sex), as documented elsewhere.(38-41) Studies with refugees have identified a relationship between depressive symptomatology and cognitive impairment that makes the acculturation process difficult.(42-48) High-risk behaviors have also been associated with the dissolution of family support networks, homelessness, long-term unemployment and poverty.(49-52) We found that women's reduced access to social capital resources, including their social networks, may have played a role in their engagement in unsafe behaviors. Our findings also underscore the need for epidemiological data on the mental health status of female deportees, particularly among those affected by substance dependence. Mental health services are scarce in Mexico.(53) However, additional studies of the impact of mental health services on deportees' health outcomes are needed as targeted programs may serve to reduce deportees' participation in high-risk behaviors. We utilized a feminist perspective and believe that the testimonies are not simply anecdotal evidence, a perspective which would minimize the significance of these events. Instead, through their testimonies it can be seen how women live the phenomenon of deportation.(31,37)
Analyzing the risk environments where deportation and (re)acculturation to Mexican society occur, we found that being deported is a reason for being discriminated, victimized and stigmatized; these social responses are exacerbated by women's drug use and the resulting stigmata (i.e., injection marks) from injecting drugs. Tijuana's Secretary of Government recently stated: "It is a constant problem, when they [deportees] come back, they are in an unknown place, with no acquaintances, no money, so they are easy prey for the mob who has been recruiting them".(54) In our study, deportation and drug use challenge women's post-deportation relationships with their families and society and contribute to their marginalization, thus reducing deportees' access to social capital and related resources. Others have documented that drug use and incarceration are frequently stigmatized,(55,56) although the degree of stigma is greater for women because of gender-based stereotypes that hold women to different standards.(57,58) Stigma may result in prejudice and discrimination that can be direct, structural or internalized,(59) the latter may be expressed as "shame and guilt" that limits help-seeking intentions and compromises access to health care, drug treatment, employment and housing. Thus, the possibility of drug use relapse and individuals' mental health problems may be exacerbated by stigma experienced by deportees. These behaviors and conditions were observed in our participants' narratives. Participants engaging in undesirable activities (e.g., drug use, deportation) are often punished,(60) which may increase the risk of victimization or exploitation or may force individuals to return to dangerous situations.(61) Stigmatizing experiences were reported by all participants and have been previously documented in Tijuana.(62)
Community responses to the influx of deported migrants merit consideration as they may affect policy development and resource allocation at local, state and federal levels.(63) The number of deportations of unauthorized and criminal aliens has increased annually since 2008(1) and includes 1 million Mexican deportees in the 2008-11 period.(2) The large volume of deportees (300 to 500 daily) arriving to Tijuana(54) may overwhelm governmental and non-governmental agencies' capacities to meet their needs. In response, Mexico's National Institute of Migration recently implemented a program that enables deportees to return home. Yet, this service may be limited to those carrying an official government identification. Thus, for example, few migrants (<400) arriving to Baja California utilized this service during the first six months of 2011.(64) The well-being of deportees will remain a significant issue for Tijuana and other border communities especially as many deportees stay in Tijuana to await U.S. re-entry or form new lives.(63) A combination of macro- and micro-level interventions may be warranted in order to aid deportees' reintegration into Mexican society and ensure their health and well-being. In particular, mechanisms that enable deportees' to re-establish their identity appear to be needed; access to these documents may reduce social and economic vulnerabilities post-deportation.
Our findings must be interpreted in the light of the following limitations. We selected participants based on self-reported deportation and cannot confirm removal events. The small sample did not permit us to achieve saturation of themes. The self-reported data may have been affected by recall bias. Participants' lengthy histories of drug use could compromise their capacity to recall the chronology of life events. This exploratory study is a secondary analysis and the interviews were not addressed to inquire about their mental health or risk behaviors in specific. Data on factors that limited women's access to a government identification are unavailable as we did not probe for this topic. However, we are exploring this issue in ongoing studies given the importance of legal documentation to resettlement experiences.
Given the pilot nature of this study and its focus on understanding the deportation process and its health and social implications, we were unable to conduct additional HIV testing to assess seroconversion; the data suggest that longitudinal studies with deportees are needed. Although we did not assess participants' mental health status, women's narratives suggest that their mental health is compromised. Future studies should assess the mental health status of deportees to determine the nature and scope of services needed; such services may potentially reduce opportunities for illicit drug use but this requires further study. Despite these limitations, our participants' stories provide a compelling view of the diverse challenges female migrants face in a post-deportation society as they attempt to re-establish their lives. Our study provides important novel data that can inform the development of additional studies examining the psychosocial impacts associated with deportation, particularly vis-à-vis HIV risk behaviors and transmission.
Our preliminary findings suggest that following deportation female deportees are in need of organized assistance which may help them reduce their engagement in HIV risk behaviors (e.g., sex work). Ruben et al.(7) argue that the forced return can only become sustainable when returnees are provided with possibilities to become re-embedded in terms of economic, social network and psychosocial dimensions. In working with refugees, Ruben et al. find that post-return assistance by a non-governmental organization was particularly helpful when financial support is combined with human guidance and practical information.(7) Without access to post-deportation health, social, and economic services, deportees in border communities, such as Tijuana, may continue to be stigmatized and marginalized.(65) Deportees may benefit from programs that aid them in accessing social capital resources in Mexico and the U.S. as social capital may be important in mitigating the negative effect resulting from deportation and may limit deportees' engagement in high-risk behaviors that may contribute to their acquisition of blood-borne infections.
This research gave voice to women who are marginalized in our society. It shows the multidimensional problems they face. Also, most of the women no longer identify themselves as Mexican or as Americans. We might say they feel they belong to non-place, and society itself considers them neither from here nor from there, a situation which Mark Augé describes as "if a place can be defined as relational, historical and concerned with identity, then a space which cannot be defined as relational, or historical or concerned with identity will be a non-place".(66) Additional qualitative research with a larger sample of female deportees is needed to understand these complex issues. We suggest that this population would be an excellent group to include in future research that focuses on the concept of intersectionality, which has been posed more as a nodal point than as a closed system, a gathering place for open-ended investigations of the overlapping and conflicting dynamics of race, gender, class, sexuality, nation, and other inequalities.(67)

