










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkSalud mental
versión impresa ISSN 0185-3325
Salud Ment vol.33 no.3 México may./jun. 2010
Artículo original
Defense mechanisms in cardiovascular disease patients with and without panic disorder
Mecanismos de defensa en pacientes cardiópatas con y sin crisis de angustia
Blanca Patricia Ríos Martínez,1* Enrique Chávez León,2 Gabriela Alejandra Rangel Rodríguez,3 Luis Guillermo Pedraza Moctezuma1
1 Hospital Ángeles del Pedregal, México, D F.
2 Escuela de Psicología, Universidad Anáhuac México Norte.
3 Centro de Apoyo Tecnológico para la Comunicación y el Aprendizaje (CATIC).
*Correspondencia:
Psicóloga y psicoterapeuta Blanca Patricia Ríos Martínez.
Hospital Ángeles del Pedregal,
Camino a Sta. Teresa 1055,
consultorio 306,
col. Héroes de Padierna, 10700,
México, D F.
Tel. (55)5652 4500,
Fax. (55)5652 5985.
E.mail: blanca_rios@hotmail.com
Recibido: 8 de julio de 2009.
Aceptado: 3 de febrero de 2010
Abstract
Introduction
Throughout the investigation of psychosocial factors in cardiovascular diseases, type A personality, anger, hostility, anxiety, and depression have been proved to participate in this kind of sufferings. Cardiac patients exposed more frequently to life stressing events than patients who do not suffer a cardiac disease might lack adaptive coping defense mechanisms to protect them or use maladaptive defense mechanisms that facilitate the pathogenic effects of anxiety. Few studies have been done in Mexico related to psychological defense mechanisms; none of them was related to medically ill patients. In the present study, the use of defense mechanisms by cardiac patients with panic disorder (panic attack) was compared to the use of defense mechanisms by patients that present similar cardiovascular pathologies but without mental disorders.
Material and method
The present investigation was made as a comparative and explanatory study with a nonexperimental design. The sample was constituted by two groups: one of 33 cardiac patients diagnosed with panic attack and another group, used as control, of 30 cardiac outpatients without psychiatric disorder; all attended the Instituto Nacional de Cardiología Ignacio Chávez (Mexico City). The 63 cardiac patients were evaluated using the Structured Interview for the Diagnosis of Axis I, Hamilton's Anxiety Scale, Hopkins's 90 Symptom Checklist and the Defensive Styles Questionnaire, self–report instrument whose reliability and validity has been established for Mexican patients with panic disorder. The statistical analysis was made through chi–square test, Student's t test, Pearson correlation and a gradual multiple regression analysis.
Results
Within the group of cardiac patients with panic attack, 72.73% were female patients and 27.27% male, with an average age of 38.52 ± 14.18 years and 5.73 ± 2.75 years of schooling. The group of cardiac patients used as control was formed by 30 subjects also in its majority female (56.7%), with an age of 45.27 ± 14.51 years and an average of 5.67 ± 3.31 years of schooling. The patients of the group with panic disorder had higher levels of anxiety and used more maladaptive defense mechanisms, such as social isolation and inhibition, tended to use more somatization and less the adaptive defenses (suppression, work orientation, sublimation, affiliation and humor), in comparison to the group without mental disorder. The criteria for panic disorder (DSM–IV) correlated directly with somatization; the ones from major depression correlated directly with regression and inversely with humor and socioeconomical level; the score in Hamilton's Anxiety Scale with maladaptive defenses as social isolation, acting out and somatization; the SCL–90 with the maladaptive defenses acting out, projection and regression. The multiple regression analysis determined that regression and somatization contributed to the panic disorder symptomatology, and leads to major depressive disorder; projection, somatization and social isolation to anxiety's intensity and reaction formation, humor, regression, fantasy, inhibition, projective identification, passive aggression and omnipotence in general to the psychiatric symptoms.
Discussion
The greater use of maladaptive defenses by the cardiac patients group with panic disorder allows to conclude that low level defenses are related to the symptoms of this mental disorder. This group showed relation between levels of anxiety, psychological discomfort and the use of maladaptive defenses such as social isolation, inhibition and somatization, tending to isolate themselves and presenting in a corporal or <<visceral>> form, through somatization, many physical symptoms. The observation of the use by cardiac patients without mental disorder of suppression, work orientation, sublimation, affiliation and humor, all of them adaptive defenses, reinforces this conclusion.
Key words: Defense mechanism, defensive styles, cardiovascular disease, panic disorder, panic attacks.
Resumen
Introducción
Gracias a la investigación de los factores psicosociales de las enfermedades cardiovasculares, se ha demostrado la participación de la conducta tipo A, enojo, hostilidad, aislamiento social, estrés, ansiedad y depresión en este tipo de padecimientos. La depresión asociada con frecuencia al infarto agudo del miocardio incrementa el riesgo de morir; los niveles altos de angustia se asocian al aumento en el riesgo de enfermedad coronaria y muerte súbita. Los pacientes cardiópatas expuestos a sucesos estresantes de la vida con más frecuencia que los pacientes que no padecen cardiopatía pueden carecer de mecanismos de defensa y afrontamiento adaptativos que los protejan o bien usan mecanismos de defensa desadaptativos que facilitan los efectos patogénicos de la ansiedad. En México se han realizado pocos estudios respecto a los mecanismos psicológicos de defensa y no hay estudios acerca del tema en pacientes médicamente enfermos. Conocer la forma en que el sujeto afronta su enfermedad permitiría una intervención psicoterapéutica oportuna en los pacientes médicos con el objetivo de mejorar su adaptación psicosocial y quizás su supervivencia. Por lo anterior, el objetivo del presente estudio es comparar el uso de los mecanismos de defensa de los pacientes cardiópatas con trastorno de angustia (crisis de angustia) con el de pacientes con patología cardiovascular similar pero sin trastornos mentales.
Material y método
Se realizó un estudio de tipo comparativo y explicativo con un diseño no experimental. La muestra estuvo constituida por dos grupos, uno de 33 pacientes cardiópatas diagnosticados con crisis de angustia y otro grupo, utilizado como control, de 30 sujetos cardiópatas sin trastorno psiquiátrico; todos acudían a Consulta Externa del Instituto Nacional de Cardiología Ignacio Chávez. Los 63 pacientes cardiópatas fueron evaluados utilizando la Entrevista Estructurada para el Diagnóstico del Eje I, la Escala de Ansiedad de Hamilton, la Lista de 90 Síntomas de Hopkins y el Cuestionario de Estilos Defensivos, instrumento autoaplicable que evalúa mecanismos de defensa adaptativos y desadaptativos del que se ha establecido su confiabilidad y validez en pacientes mexicanos con trastorno de angustia. El análisis estadístico se realizó a través de la chi cuadrada, t de Student, correlación de Pearson y un análisis de regresión múltiple gradual.
Resultados
Dentro del grupo de cardiopatías con crisis de angustia, 72.73% eran pacientes femeninos y 27.27% masculinos, con edad promedio de 38.52 ± 14.18 años y 5.73 ± 2.75 años de escolaridad. El grupo de pacientes cardiópatas, que se utilizó como control, estuvo constituido por 30 sujetos, también en su mayoría femeninos (56.7%), de 45.27 ± 14.51 años de edad con promedio de 5.67 ± 3.31 años de escolaridad. Los pacientes del grupo con trastorno de angustia tuvieron niveles más altos de ansiedad y utilizaron más mecanismos de defensa desadaptativos como aislamiento social e inhibición, tendieron a usar la somatización y utilizaron menos defensas adaptativas (supresión, orientación al trabajo, sublimación, afiliación y humor), en comparación con el grupo sin trastorno mental. Los criterios del trastorno de angustia (DSM–IV) se correlacionaron con la somatización; los de la depresión mayor, directamente con la regresión e inversamente con el humor y con el nivel socioeconómico; la puntuación de la Escala de Ansiedad de Hamilton, con defensas desadaptativas como aislamiento social, exoactuación y somatización; el SCL–90, con las defensas desadaptativas exoactuación, proyección y regresión. El análisis de regresión múltiple determinó que la regresión y la somatización contribuyeron a la sintomatología del trastorno de angustia, el consumo en el trastorno depresivo, la proyección, somatización y aislamiento social en la intensidad de la angustia y la formación reactiva, humor, regresión, fantasía, inhibición, identificación proyectiva, pasivo–agresividad y omnipotencia en la sintomatología psiquiátrica general.
Discusión
El mayor uso de defensas desadaptativas por parte del grupo de pacientes cardiópatas con trastorno de angustia permite concluir que las defensas de bajo nivel se relacionan con los síntomas de este trastorno mental. Este grupo mostró relación entre los niveles de ansiedad y malestar psicológico y la utilización de defensas desadaptativas como el aislamiento social, inhibición y somatización. Asimismo, tendió a aislarse y a manifestar en forma corporal o <<visceral>>, a través de la somatización, muchos síntomas físicos. La observación de que los pacientes cardiópatas sin trastorno mental utilizaron la supresión, orientación al trabajo, sublimación, afiliación y humor, todas ellas defensas adaptativas, refuerza esta conclusión.
Palabras clave: Mecanismos de defensa, estilos defensivos, enfermedad cardiovascular, trastorno de angustia, crisis de angustia.
INTRODUCTION
In cardiovascular disorders studies, it has been observed that they frequently coexist with different psychiatric disorders.1,2 The investigation of psychosocial, conduct and personality factors in the course and development of cardiovascular diseases has demonstrated the participation of personality characteristics such as Type A personality, borderline personality disorder,3 anger and hostility,4 social isolation, stress, anxiety and depression. These two last components have been the two first consulting causes among the population that assists to the family or medical doctor with physical pain and as the principal factors that contribute to coronary disease.5
Regarding depression and coronary patients, it has been found that psychopathology is often associated to acute myocardial infarction (AMI),4,6,7 with a high risk of cardiovascular mortality.8–10
Although anxiety might be seen as an adaptive psychological mechanism, high levels of anguish (mental stress, panic disorder, phobia and other anxiety disorders) are pathological processes that exceed the physical and emotional coping capacities of the individual, and are associated to an increasing risk of coronary disease and sudden death.11–14 Panic disorder,15 frequent in emergency rooms, can go unnoticed by the specialist doctor;16,17 untrained mental health doctors ought to know anxiety manifestations and should be familiarized with the diagnosis.18
Some cardiac patients display high levels of anxiety throughout almost all of their of lives, specially during the last three to five years before the clinical manifestations of cardiac disorders appear.19 This association seems to be due to the patients' exposure to stressing events of life more frequently than patients who do not suffer cardiac disease; or, although they are exposed to the same stressors than no cardiac patients, they lack adaptive defense and coping mechanisms to protect them from the pathogenic effects of extreme levels of anxiety.20
A revision on related literature indicates that in Mexico few studies have been done on the matter21–24 and there are no studies about defense mechanisms in medically ill patients. In this study, the use of defense mechanisms in cardiac patients with panic attack was compared to the use of defense mechanisms in patients with similar cardiovascular pathology without associated mental disorders. The objective of this investigation was to determine if physical annoyances associated to cardiovascular sufferings and similar to symptoms of panic disorder could influence the use of maladaptive defense mechanisms. If used defenses depend on the presence of physical symptoms, the defense mechanisms used by the group of cardiac patients with panic disorder should be similar to the mechanisms used by the group of cardiac patients who acted as control. On the contrary, it is possible to postulate that patients with panic disorder use maladaptive defenses responsible for the symptoms of the panic disorder.
MATERIAL AND METHOD
Sample
Sixty–three cardiac outpatients of the Instituto Nacional de Cardiología Ignacio Chávez were included. Thirty three were diagnosed also with panic Attacks by the assigned psychiatrist and 30 without psychiatric disorder; this constituted the control group. In order to confirm or to discard the diagnosis, the 63 patients were reevaluated using the Structured Clinical Interview for Axis I Disorders (SCID I),25 in agreement to diagnosis criteria from DSM–IV.26 In order to evaluate the intensity of anxiety and other symptoms, Hamilton's Anxiety Scale (HAM–A) was applied,27,28 as well as the Hopkins 90 Symptoms CheckList (SCL–90).29 Defense mechanisms were evaluated through the Defense Style Questionnaire (DSQ).30,31
Instruments
In this investigation four instruments were used. Structured Clinical interview for Axis I Disorders (SCID–I), which evaluates the criteria of mental disorders, including panic disorder. Hamilton's Anxiety Scale (HAM–A), formed by 14 items that measure intensity of anxiety (it is graded from 0 to 4, 0 being the lowest intensity). Hopkins 90 Symptoms Checklist (SCL–90), self–report instrument of 90 items that evaluates symptoms of diverse psychiatric disorders, composed by 10 subscales (somatization, obsession–compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid thoughts and psychotic tendencies). It is codified according to a Likert scale from 0 to 4: zero being the absence of the symptom and four, the symptom being very serious. Defense Style Questionnaire (DSQ), constituted by 88 phrases that evaluate defense mechanisms seen like series of ideas, attitudes and conducts, conscious manifestations of unconscious processes (that try to reconcile external demands with internal drives). These defense mechanisms are considered as well as the style to handle conflicts and stress under certain circumstances and also reflect the degree of psycho–social development of personality.32 This questionnaire includes adaptive defensive mechanisms (affiliation, altruism, anticipation, reaction formation, humor, orientation to work, sublimation, suppression) and maladaptive (undoing, isolation, social isolation, consume, splitting, acting out, fantasy, idealization, projective identification, inhibition, denial, passive aggression, projection, help rejection, regression, somatization and omnipotence). Its validity and reliability have been established for Mexican patients with panic disorder,21,23,31 which is similar to the observed in other studies.33
Statistical analysis
This is a nonexperimental comparative and explicative study. For the comparison of the demographic variables, nonparametric statistics were used (chi square); for the scores of the different scales, Student t test was used and to establish the relation between continuous variables the Pearson correlation index was used. The weight of defense mechanisms in symptoms of panic attack was determined through multiple regression analysis.34
RESULTS
Sociodemographic and clinical characteristics of the sample
The group of cardiac patients with panic disorder (n=33) was constituted by 24 female patients (72.73%) and 9 men (27.27%), with an average age of 38.52 ± 14.18 years and 5.73 ± 2.75 school years. Most belonged to socioeconomic class 2 (n=18, 54.5%) and to catholic religion (n=31, 93.9%).
On the other hand, the group of cardiac patients without panic disorder, used as control, was constituted by 30 subjects, also in its majority female patients (n=17, 56,7%), of 45.27 ± 14.51 years of age, with an average of 5,67 ± 3,31 school years, belonging mainly to level 2 socioeconomic class (n=18, 60%) and to catholic religion (n=26, 86.7%). Both groups were similar in sociodemographic variables (table 1).

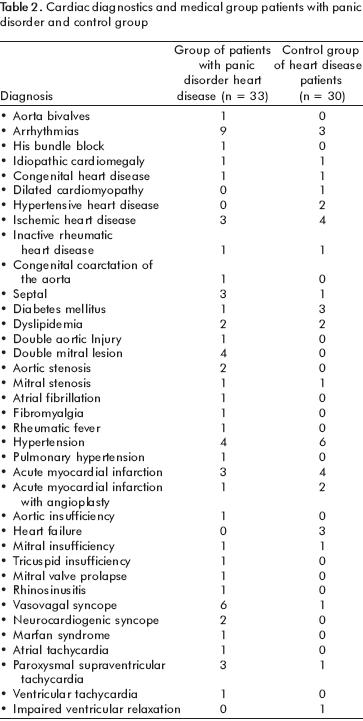
The most frequent cardiovascular disorders for both groups can be appreciated in table 2.
Characteristics of the Group of Cardiac Patients with Panic Disorder
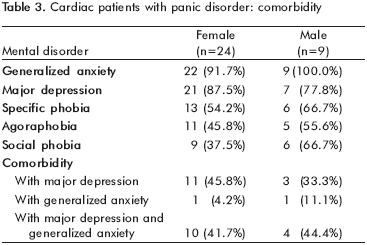
The psychiatric diagnosis of the patients with panic disorder was confirmed with the Structured Clinical Interview for DSM IV Axis I Disorders (SCID–I).25 Some patients displayed other diagnoses (table 3), being the most frequent: general anxiety disorder (91.7% women vs. men 100%), major depressive disorder (women 87.5% vs. men 77.8%) and specific phobia (54.2% women vs. men 66.7%). The coexistence of several disorders (comorbidity) was more frequent in women between panic disorder and major depressive disorder(45.8%), and in men between panic disorder, major depression and generalized anxiety disorder (44.4%). The comparison by gender through X2 was not significant.
Anxiety Intensity and General Psychological Discomfort
The score of the psychopathologic symptoms, measured by SCL–90, was 138.91 ± 52.77. The index of the mentioned instrument (total score divided by the number of items) was 1.62 ± 0.59 in female patients and 1.33 ± 0.56 in male patients. Regarding the level of anxiety, quantified through HAM–A, women and men had similar scores (27.67 ± 9.10, 25.33 vs. ± 8.78, p= n.s.).
Score of the defense mechanisms
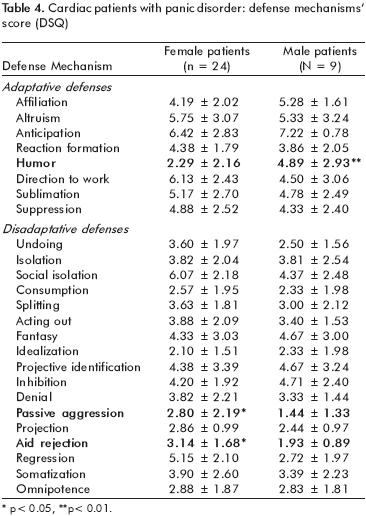
The score observed in the DSQ of defense mechanisms was similar between women and men. Nevertheless, women used more the defense help rejection (3.14 ± 1.68 vs. 1.93 ± 0.89, t 2.04 df 31 p=.013) and passive aggressiveness (2.79 ± 2.19 vs. 1.44 ± 1.33, t 1.72 df 31 p=.043) than men. On the other hand, men scored higher in the defense mechanism of humor (2.29 ± 2.16 vs. 4.89 ± 2.93, t 2.79, df 31, p=.009) (table 4).
Defense mechanisms score according to the presence of mental disorders associated to panic disorder
When the use of defense mechanisms by patients who had only panic disorder was compared to those which presented panic disorder associated to major depressive disorder and agoraphobia and to agoraphobia and major depressive disorder simultaneously, no differences were found, meaning that the presence of other mental disorders did not influence the use of defense mechanisms.
Comparison of the Group of Cardiac Patients with Panic Disorder versus Control Group
Patients with Panic Disorder had higher levels of anxiety in HAM–A, total score of 27.03 ± 8.94 versus 15.40 ± 8.61 (t 5.25, df 61, p=0.000). They also scored higher in SCL–90, well in the total sum, 139.91 ± 52.77 versus 88.77 ± 54.99 (t 3.69, df 61 p=0.000) as in the index, 1.54 ± 0.59 vs. 1.10 ± 0.60 (t 2.92, df 61, p=.005).
In the same way, they used more some mechanisms of defense considered as maladaptive (figure 1). This group scored higher in: social isolation (5.61 ± 2.35 vs. 3.91 ± 2.42; t 2.82 df 61, p=.007), inhibition (4.34 ± 2.04 vs. 3.29 ± 1.74; t 2.19 df 61, p=.032) and tended to use somatization (3.76 ± 2.48, 2.62 vs. ± 2.14; t 1.95, df 61, p=.055). However, they used less psychological defenses considered as adaptive as: suppression (4.73 ± 2.46 vs. 6.35 ± 1.76; t –2.98 df 61, p= .004), orientation to work (5.68 ± 2.67 vs. 7.05 ± 2.23; t – 2.20 df 61, p= .032), sublimation (5.06 ± 2.61 vs. 6.3 ± 2.28; t – 2.0 df 61, p=.050), affiliation (4.48 ± 1.95 vs. 5.80 ± 2.70; t – 2.23 df 61, p=.029) and humor (3.0 ± 2.62 5.33 vs. ± 2.96; t – 3.32 df 61, p=.002), in comparison to the group of cardiac patients without mental disorder. The scores of the rest of the defense mechanisms were similar between both groups.

Correlation between Defense Mechanisms (DSQ) Anxiety Intensity (HAM–A), Psychological Discomfort (SCL–90) and General Psychopathological Manifestations (SCID–I/DSM IV)
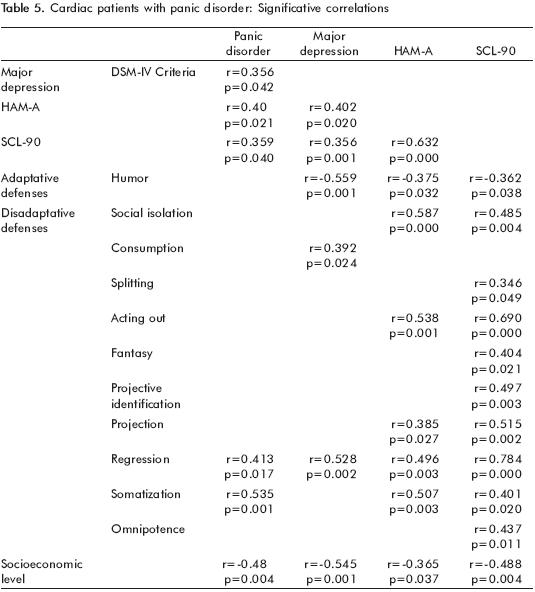
Pearson correlation determined the existing relation between defense mechanisms and panic disorder symptoms (table 5). The number of criteria of panic disorder (DSM–IV) correlated significantly with the maladaptive defense of somatization (r=0.535, p=0.001); the number of criteria of major depression correlated inversely with the maladaptive defense of regression (r=0.528, p=0.002) and inversely with the adaptive defense of humor (r=–0.559, p=0.001) and with socioeconomic level (r=–0.545, p=0.001). The total score of Hamilton's Anxiety Scale correlated with the one of SCL–90 (r=0.632, p=0.000) and with the maladaptive defenses of social isolation (r=0.587, p=0.000), acting out (r=0.538, p=0.001) and somatization (r=0.507, p=0.003); SCL–90 correlated significantly with the mal–adaptive defenses of acting out (r=0.690, p=0.000), projection (r=0.515, p=0.002) and regression (r=0.784, p=0.000). The remaining correlations were not significant.
Weight of defense mechanisms in anxiety intensity and other psychopathological symptoms
A multiple regression analysis was made to determine the degree in which defense mechanisms participated in socio–demographic variables, manifestations of panic disorder and major depressive disorder, anxiety intensity(HAM–A) and general psychopathological manifestations (SCL–90).
Defenses that contributed to the symptomatology of panic disorder (F=8.48, df 2, 30, p=.001), were regression (β=.285, t=1.87, p=.07) and somatization (β=.455, t=2.99, p=.006); these two mechanisms of defense explained 31.9% (R2 adjusted=.319) of the criteria of panic attacks (variance) that the patients displayed.
In the case of the criteria of mayor depressive disorder (F=11.724, df 3, 29 p=.000), the defense mechanism that participated was consume (β=.348, t=2.712, p=.011). However, humor (β=–.316, t=–2.251, p=.032) contributed negatively. Socioeconomic class also had an influence in the presence of depression criteria in this group of cardiac patients ((β=–.432, t=–3.132, p=.004). The three mentioned variables explained 50.1% of the depression variance(R2 adjusted=.501).
In anxiety intensity, evaluated through Hamilton's Anxiety Scale (HAM – A) (F= 9.90 df 4, 28 p=.000), defense mechanisms that contributed were: projection ( β=.465, t=3.30 p=.003), somatization (β=.406, t=3.21 p=.003), and social isolation (β=.305, t=2.37 p=.025). On the contrary, rejection to help (β=–.498, t=–3.46 p=.002) and affiliation (β=–.279, t=–2.27 p=.031) worked in a negative sense. The variance explained by these variables corresponded to 65.2% (R2adjusted=.588).
Hopkins Symptom Checklist 90 (SCL–90) evaluates several symptoms of anxiety, depression, somatization, psychosis and others. The related defense mechanisms were (F=40.461, gl 14.18 p=.000): reactive formation (β=.26, t=4.46, p=.000), humor (β=.18, t=2.72, p=.014), regression (β=.79, t=10.23, p=.000), fantasy (β=.29, t=5.35, p=.000), inhibition (β=.28, t=3.76, p=.001), projective identification (β=.24, t=4.01, p=.001), passive aggressiveness (β=.31, t=6, p=.000), omnipotence (β=.31, t=4.98, p=.000), orientation to work (β=–.20, t=–3.65, p=.002), idealization (β=–.18, t=–3.17, p=.005), denial (β=–.25, t=–4.80, p=.000) and projection (β=–.14, t=–2.21, p=.041). Also, it was demonstrated that age (β=.22, t=3.79, p=.001) and years of school (β=.41, t=6.83, p=.000) are variables that contribute to the psychological discomfort evaluated by the SCL–90. These 14 variables explained 94.5% of the variance (R2 adjusted=.945).
When these two variables were eliminated (age and years of school), the defense mechanisms that contributed importantly for the score of SCL–90 (F=49.32, df2.30, p=.000) were projective identification (β=.39, t=4.42, p=.000) and regression (β=.73, t=8.17, p=.000) that explained 75.1% of the variance (R2 adjusted=.751), this is, a little more than three fourths of the score of this instrument.
DISCUSSION
The greater use of maladaptive defenses by the group of cardiac patients with panic disorder in contrast to the use of adaptive defenses by the group of cardiac patients without an associated mental disorder allows us to assure that low level defenses are related to the symptoms of this mental disorder. That group showed higher levels of anxiety and psychological discomfort due to the presence of the panic disorder and to a greater use of maladaptive defense mechanisms such as social isolation, inhibition and somatization; this is, against stressing events. Participants of this group tend to isolate and to maintain ideas, feelings, memories, desires or fears out of conscience, showing them physically or <<viscerally>> through somatization (expression of repressed conflicts through physical symptoms). On the other hand, cardiac patients without mental disorder used suppression, orientation to work, sublimation, affiliation and humor, all of them adaptive defenses; patients of this group look for help or support in others (affiliation), avoid intentionally to think about unpleasant experiences (suppression) and will try to canalize their maladaptive feelings or impulses through socially accepted behaviors (sublimation), as focusing themselves to work and seeing amusing and ironic aspects in their own problems (humor).35
The use of maladaptive mechanisms of defense is related to the psychopathological degree as the direct correlation between some defense mechanisms (regression, acting out and somatization) and the intensity of anxiety measured through HAM–A as well as with psychological discomfort registered by the SCL–90. Clinically, one of the most obvious defense mechanisms in patients with panic disorder is somatization; in this study a direct correlation between the score of this mechanism in DSQ and the number of DSM–IV diagnoses criteria for panic disorder was observed: the greater use of this defense, the higher the number of criteria for panic attack.
The results leave no doubt of the relation between defense mechanisms and symptomatology and intensity of the panic disorder, as well as with other psycho–pathological symptoms occurring and associated to comorbidity, as it has been reported previously.21,23
The multiple regression analysis allowed determining the percentage of the variance of DSM–IV criteria, Hamilton´s Scale of Anxiety and SCL– 90 explained by different mechanisms from defense. For example, it was found that regression and somatization contribute in the disorder's criteria (SCID–I); regression and projective identification explain psychopathological manifestations of SCL–90; projection, somatization and social isolation of anxiety intensity (HAM–A). On the opposite, using affiliation and help rejection determines lower scores in HAM–A, meaning that if these mechanisms are reinforced, the intensity of anxiety diminishes.
The greater frequency of panic disorder in women agrees with previous investigations.17 The comorbidity of the panic disorders with other mental disorders has also been reported in the literature.18 Using a structured clinical interview to establish diagnoses, after each patient had been evaluated clinically, allowed observing the existing relation between cardiovascular diseases, panic disorders and other psychical dysfunctions (major depression, agoraphobia, general anxiety disorder, among others). Women cursed simultaneously with major depressive disorder and men mainly with general anxiety disorder, although these differences were not significant. It was also observed that patients with more than one disorder use similar ways to confront conflicting situations (defense mechanisms) than those who only suffer panic disorder.
Patients with panic disorder presented some differences and similarities when compared by gender. It was demonstrated that men and women show the same levels of anxiety, psychological discomfort, as well as the use of some defense mechanisms. Nevertheless, humor is associated closer to men, while the mechanisms of help rejection and passive–aggression were characteristic of women. These differences can be due to the preservation of the stereotype of man with <<emotional force>> in Mexican Culture, which explains why the use of humor is reinforced as part of the method for handling their emotions; on the other hand, women adopt an abnegation attitude that might conceal aggression.36
One of the greatest challenges that can be found in a hospital medical practice is to be able to establish a differential diagnosis between a primary cardiovascular disorder and a psychiatric disorder.16 The symptomatology of panic attack includes precordial oppression, an increase on heart rate, respiratory difficulties and weakness, as well as other symptoms that the physically healthy patient frequently relates to a serious cardiac problem. In patients with cardiovascular disorders, the coexistence of symptoms associated to the physical disorder and panic attack symptoms difficults the diagnosis of the mental disorder. The results of this study support the possibility of diagnosing and evaluating through structured interviews and measuring instruments of psychopathological symptoms intensity, panic disorder and other major mental disorders. Although the sample was obtained by quotas and establishing the association frequency between panic disorder and cardiovascular diseases was not possible, other studies have demonstrated the coexistence in both groups of pathology.18,37
The results of this study indicate the importance of the psychological intervention in the field of cardiology, especially in cardiac disorders accompanied by mood and anxiety disorders, including panic disorder. These pathologies have been related to the use of maladaptive defense mechanisms.38
The current psychotherapeutic approach for panic disorder is cognitive behavioral therapy (CBT);39 nevertheless it is possible that defense mechanisms are also related to patients with panic disorder personality.40 It might be useful to apply a line of psychological intervention directed to the recognition of use, evaluation, factors related to the presence and modification of defense mechanisms with the purpose of equipping the patient with more adaptive options and improving life quality.41–44
ACKNOWLEDGEMENTS
We thank for the support offered by the Instituto Nacional de Cardiología Ignacio Chávez and Anáhuac México Norte University.
REFERENCES
1. Sadock BJ, Sadock VA. Kaplan & Sadock's Synopsis of Psychiatry. Behavioral sciences/clinical psychiatry. Tenth edition. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2007, pp.818–819. [ Links ]
2. Pelle AJ, Denollet J, Zwisler AD, Pedersen SS. Overlap and distinctiveness of psychological risk factors in patients with ischemic heart disease and chronic heart failure: Are we there yet? J Affect Dis 2009;113:150–156. [ Links ]
3. Dammen T, Ekeberg O, Arnesen H, Friis S. Personality profiles in patients referred for chest pain: Investigation with emphasis on panic disorder patients. Psychosomatics 2000;41:269–276. [ Links ]
4. Friedman H, Booth–Kewley S. Personality, type a behavior, and coronary heart disease: the role of emotional expression. J Pers Soc Psychol 1987;53:783–792. [ Links ]
5. Weeke A, Juel K, Vaeth M. Cardiovascular death and manic–depressive psychosis. J Affect Disord 1987;13:287–292. [ Links ]
6. Ladwig KH, Röll G, Breithardt G, Budde T, Borggrefe M. Post–infarction depression and incomplete recovery 6 months after acute myocardial infarction. Lancet 1994;343:20–23. [ Links ]
7. Strik J, Honig A, Lousberg R, Denollet J. Sensitivity and specificity of observer and self–report questionnaires in major and minor depression following myocardial infarction. Psychosomatics 2001;42:423–428. [ Links ]
8. Furlanetto L, Von Ammon S, Romildo D, Creech S, Powell L. Association between depressive symptoms and mortality in medical inpatients. Psychosomatics 2000;41:426–432. [ Links ]
9. Sheps DS, Sheffield D. Depression, anxiety, and the cardiovascular system: the cardiologist's perspective. J Clin Psychiatry 2001;62:12–18. [ Links ]
10. Borowicz L, Royall R, Grega M, Selnes O, Lyketsos C et al. Depression and cardiac morbidity 5 years after coronary artery bypass surgery. Psychosomatics 2002;43:464–471. [ Links ]
11. Kawachi I, Sparrow D, Vokoneas P, Weiss S. Symptoms of anxiety and risk of coronary heart disease. Circulation 1994;90:2225–2229. [ Links ]
12. Frasure–Smith N, Lespérance F, Talajic M. The impact of negative emotions on prognosis following myocardial infarction: Is it more than depression? Health Psychol 1995;14:388–398. [ Links ]
13. Frasure–Smith N. In hospital symptoms of psychological stress as predictors of long–term outcome after acute myocardial infarction in men. Am J Cardiol 1991;68:31–34. [ Links ]
14. Januzzi J, Stern T, Pasternack R, DeSactis R. The influence of anxiety and depression on outcomes of patients with coronary artery disease. Arch Intern Med 2000;160:1913–1921. [ Links ]
15. Asociación Psiquiátrica Americana. Manual Diagnóstico y Estadístico de los Trastornos Mentales. Texto revisado. DSM–IV–TR. Barcelona: Masson; 2002. [ Links ]
16. Fleet R, Dupuis G, Marchand A, Burelle D, Arsenault A, et al. Panic disorders in emergency department chest pain patients: prevalence, co–morbidity, suicidal ideation and physician recognition. Am J Med 1996;101:371–380. [ Links ]
17. Jeejeebhoy F, Dorian P, Newman D. Panic disorder and the heart: a cardiology perspective. J Psychosom Res 2000;48:393–403. [ Links ]
18. Chávez–León E. Trastornos de ansiedad. En: PAC psiquiatría–5. Libro 8. Trastorno de angustia (trastorno de pánico, panic disorder). México D.F.: Intersistemas; 2004. [ Links ]
19. Dupont MA. Manual clínico de la ansiedad. 1era Ed. México: JGH Editores; 1999. [ Links ]
20. Laplanche J, Pontalis J. Diccionario de psicoanálisis. Barcelona: Labor; 1987. [ Links ]
21. Chávez–León E, Ontiveros–Uribe MP, Lara–Muñoz C. Defense mechanisms in anxiety disorders. American Psychiatric Association 2001 Annual Meeting. New Orleans: New Research Abstracts; 2001; pp.162–163. [ Links ]
22. López–Ramírez ME, Chávez–León E. Relationship between defense mechanisms and personality disorder. American Psychiatric Association 2004. Annual meeting. New York: New Research Abstracts; 2004; p.101. [ Links ]
23. Chávez–León E, Lara–Muñoz C, Ontiveros–Uribe MP. An empirical study of defense mechanisms in panic disorder. Salud Mental 2006;29(6):15–22. [ Links ]
24. Benitez–Camacho E. Los mecanismos de defensa presentes en los niveles de funcionamiento psicológico. Un estudio empírico. Tesis de maestría en psicología clínica y psicoterapia. México: Universidad Anáhuac; 2007. [ Links ]
25. First MB, Spitzer RL, Gibbon M, Williams JBW. Structured clinical interview for DSM–IV Axis I Disorders clinical version (SCID–IV). Washington: American Psychiatric Press; 1997. [ Links ]
26. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. DSM–IV. Fourth edition. Washington: American Psychiatric Association; 1994. [ Links ]
27. Hamilton M. Development of a rating scale for primary depressive illness. B J Soc Clin Psychol 1967;6:278. [ Links ]
28. Lara M, Ontiveros M, Berlanga C, De la Fuente J. Diferencias entre crisis de angustia y ansiedad generalizada en la Escala de Hamilton de ansiedad. Salud Mental 1988;11:7–10. [ Links ]
29. Bech P, Allerup W, Maier M, Albus P, Lavori P et al. The Hamilton scales and the Hopkins symptom checklist (SCL–90): A Cross–national validity study in patients with panic disorders. Br J Psychiatry 1992;160:206–211. [ Links ]
30. Andrews G, Singh M, Bond M. The defense style questionnaire. J Nerv Ment Dis 1993;181:246–256. [ Links ]
31. Chávez–León E. Relación de los mecanismos de defensa con los trastornos de angustia. Tesis de maestría en psiquiatría (psicología médica). México: UNAM/Instituto Mexicano de Psiquiatría; 1998. [ Links ]
32. Bond M, Gardner ST, Christian J, Sigal JJ. Empirical study of self–rated defense style. Arch Gen Psychiatry 1983;40:333–338. [ Links ]
33. Rutherford MJ, McDermott PA, Cacciola JS et al. A psychometric evaluation of the Defense Style Questionnaire in methadone patients. J Personal Dis 1998; 12: 119– 125. [ Links ]
34. Hernández–Sampieri R, Fernández C, Baptista P. Metodología de la investigación. México: Mc Graw Hill Interamericana; 2003. [ Links ]
35. Ríos B. Los mecanismos de defensa en pacientes cardiópatas con y sin crisis de angustia, su trascendencia para la intervención psicoterapéutica. Tesis de maestría en psicología clínica y psicoterapia. México: Universidad Anáhuac; 2004. [ Links ]
36. Lawrence M, Maguire M. Psychoterapy with women. New York: Routledge; 1999. [ Links ]
37. Starcevic V. Treatment of panic disorder: recent developments and current status. Expert Rev Neurother 2008;8:1219–1232. [ Links ]
38. Bond M. Empirical studies of defense styles: Relationships with psychopathology and change. Harv Rev Psychiatry 2004;12:263–278. [ Links ]
39. Barlow DH. Clinical handbook of psychological disorders. A step–by–step manual. Fourth edition. New York: Guilford Press; 2008. [ Links ]
40. Sinha BK, Watson DC. Personality disorder cluster and the Defense Style Questionnaire. Psychol Psychother Theory Res Pract 2004;77:55–66. [ Links ]
41. Cramer P. Defense mechanisms in Psychology today. Am Psychol 2000;55:637–646. [ Links ]
42. Norem JK. Why should we lower our defenses about defense mechanisms? J Personal 1998;66:895–917. [ Links ]
43. Milrod B, Leon AC, Busch F et al. A randomized controlled clinical trial of psychoanalytic psychotherapy for panic disorder. Am J Psychiatry 2007;164:265–272. [ Links ]
44. Hales R, Yudofky S, Talbott J. Tratado de psiquiatría. Tomo I. DSM IV. 3ª Ed. México: Masson; 2001. [ Links ]
NOTA
* Artículo sin conflicto de intereses

