











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
The Covid-19 pandemic is the worst global public health crisis in the past hundred years. Staggering morbidity and mortality rates and a costly burden for the most affected countries’ health systems clearly illustrate the magnitude of the emergency.1,2 the first half of 2020, the rapidly increasing number of severe cases required governments to shift existing healthcare personnel, hospitals, and clinics, and secure additional equipment and supplies to provide care to Covid-19 patients. Consequently, the pandemic disrupted routine medical services swallowing supplies, human resources, and infrastructure hitherto devoted to other health problems.3,4 Furthermore, people’s perceptions and mobility restrictions may have also resulted in reduced decisions to seek healthcare.
An online survey conducted in Singapore found that 40% of the participants with self-reported chronic conditions missed at least one appointment in the last two months during the Covid-19 epidemic because it was canceled either by the provider or by themselves due to fear of contracting Covid-19.5 A telephone survey conducted in Hong Kong found that 30% of respondents avoided medical consultations during the Covid-19 outbreak.6 The study showed that being female, married, highly educated, and having Covid-19-related mental health problems were factors associated with missing appointments. A study in the Netherlands found that health services for prevention, acute, and chronic conditions decreased significantly from 2019 to 2020 and experienced, in contrast, increasing telephone-, email-, or video-consultations of 22.7 percentage points in the same period.7 A study in Germany showed reductions in consultations and hospitalizations for the elderly and fewer diagnoses of diabetes, dementia, depression, cancer, and stroke during the lockdown, compared to the same period in 2019.8
By March 2021, Mexico accumulated more than 2.2 million cases of Covid-19 and over 200 000 confirmed deaths.9 Early in 2020, the country converted hospitals, partially or entirely, to provide care to Covid-19 patients.10 Medical personnel and hospitals shifted their focus to face the challenge of the epidemic. However, it is unclear to what extent health care for acute and chronic conditions was either postponed or entirely forgone because of the pandemic and for how long.
This analysis aims to describe health care utilization patterns in primary health facilities during the Covid-19 epidemic in Mexico. We first present facility level, national trends in diabetes screening, and detection rates between January 2014 and December 2020, using monthly data from the Ministry of Health (SS), the healthcare system for the Mexican population who have no access to social security because of their employment status. We then present the cascade of care that identifies the proportion of the population that sought and received care in public or private facilities, using the National Health and Nutrition Survey Covid-19 2020 (Encuesta Nacional de Salud y Nutrición Covid-19 2020, Ensanut Covid-19 2020). We document the reasons for not seeking care, highlighting those most likely associated with Covid-19. We also investigate public and private coverage and the distribution of health problems. Finally, we estimate the factors associated with the probability of receiving care in public health facilities. To our knowledge, this is the first study on health care utilization and displaced health care associated with Covid-19 in Mexico.
Materials and methods
To understand the disruption of health care caused by the Covid-19 pandemic, first, we estimated diabetes screening and detection rates using data from the SS Health Information Systems (HIS).11 Screened and diagnosed patients are reported monthly by the SS primary health facilities. We estimated rates per 100 000 population at the municipality level.12 We conducted piecewise regressions to assess the effect of the pandemic on the production of these services.13 We fitted independent models before and after the “stay at home” government advice to test the hypothesis that Covid-19 care displaced diabetes services.14 We selected diabetes as an example because of the volume of services devoted in Mexico to this disease, one of the leading causes of mortality and morbidity.15
After establishing the effect of the pandemic on primary services from the perspective of the SS, we explored the health care utilization patterns from the perspective of the households. We used data from the Ensanut Covid-19 2020 collected in a sample of 10 216 households between August 18th and November 13th, 2020.16 The Ensanut Covid-19 2020 is representative nationally, regionally (for nine geographical regions), and for urban and rural areas. The survey’s objective was to estimate the seroprevalence of Covid-19, the prevalence of diabetes, hypertension, and obesity, and to document the population’s and the health system’s response to the Covid-19 pandemic.
We used the “cascade of care” framework.17 The cascade starts with the population that reports experiencing a health need within the past three months. We defined a health need as any health-related motive to contact the health system, including acute infections, chronic diseases, injuries, preventive and mental health services, or any programmed visit. Among the population who reported a health need, the cascade follows the shares that sought care, received care, and received care in the public sector. We document reasons for not seeking care, distinguishing those most likely associated with Covid-19.
As for the population who did receive care, we analyzed the distribution of their health providers and contrasted it with the patients’ affiliation to social security institutions. We followed the standard classification of social security affiliations according to the population’s employment status. Mexican Institute for Social Security (Instituto Mexicano del Seguro Social, IMSS) covers employees in the private sector, and Institute of Social Security and Services for State Workers (Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, ISSSTE) covers government workers. We classified other government employees in specific sectors, such as the army or navy, as “Other Public.” A small proportion of the population purchases private health insurance, but we included them as a single group, under “private health insurance”. People in the informal sector of the economy or unemployed have no affiliation, and we classified them as “uninsured.”
Concerning health care provision, people in the social security systems are entitled to receive care by the same institutions’ network of health care facilities (IMSS, ISSSTE, or Other Public). People with no affiliation receive care in facilities of the SS. Regarding private providers, we distinguished medical offices in pharmacies (MOF) from others.
We displayed the distribution of health needs by seeking behavior and for those who received care in public or private facilities
Finally, we ran a probit regression model to assess the probability of receiving care in public facilities vs. private providers and the probability of receiving care in public facilities vs. not receiving care. The analyses included the following sociodemographic variables. Age group (20-39, 40 to 59, or more than 60), sex, education (no education, primary, secondary, high school, college, or more). Socioeconomic status (low, middle, high), based on a wealth index estimated applying principal component analysis. The index included household durables (TV, fridge, washing machine, computer), housing characteristics (floor, wall, ceiling, and roof materials), and services (electricity, water, fuel, sewer system, toilet); a binary variable for employment status -currently working (worked during the last week at least one hour) versus not working-, and a binary variable for social security -uninsured versus insured. We also added a binary variable for urban vs. rural.
Results
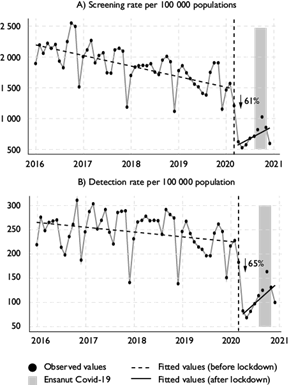
Figure 1 shows trends in diabetes screening and detection rates between January 2016 and December 2020. Panels A and B show a pre-Covid downward trend; however, both rates fell sharply --61 and 65% respectively-- after the “stay at home” recommendation in April 2020. Although by the time of the Ensanut Covid-19 2020 survey (grey strips), both screening and testing had improved, they were still far from their pre-pandemic levels.
Notes:
1) Screening rate is the total number of tests performed per month per 100 000 population without social security.
2) Detection rate is the total number of positive tests of diabetes per 100 000 population without social security.
3) The gray region Ensanut Covid-19 represents the data collection period of the survey.
4) The dotted vertical line indicates the beginning of the “stay at home” in Mexico.
Figure 1 Trends in diabetes screening and detection rates between January 2014 and December 2020, Mexico
Figure 2 shows the cascade of care in which 18.6% of the population had a health need within three months before the survey (panel 1). Of these, 82% sought health care, 81% received care, and only 34% received care in a public health facility. The main reason for not seeking care was that the ailment was mild (55%), 12% reported economic constraints, 11% reported fear of contracting Covid-19, and 4% had their appointment rescheduled (panel 2). The reasons for not seeking care most likely associated with Covid-19 include fear of contracting Covid, no clinic available, and rescheduled appointments (20%).

Figure 3 shows the distribution of health care providers for the population who reported a health need and received care, according to the patients’ affiliation. Overall, 42.5% received care in public health facilities (22.6% in IMSS, 14.7% in SS, 4.2% in ISSSTE, and 1.1% in other public health facilities.) Of the 57.5% seen by private providers, 18% received care in MOF, and 39.5%, in other private facilities.
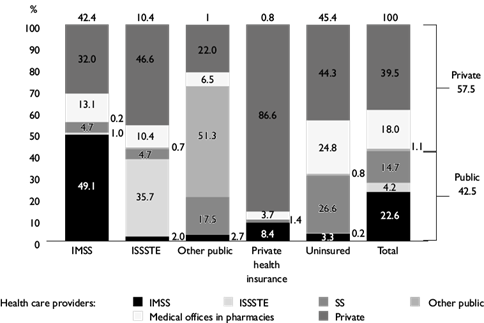
Note: Own estimations using data from the Encuesta Nacional de Salud y Nutrición Covid-19 2020 on July 2021. Descriptive statistics used the complex survey design. Each column groups the population by their primary health insurance affiliation. Within each column the distribution of health care providers used for the last health need experienced in the last three months is displayed. The top of the column shows the proportion affiliated to the primary health insurance institution. IMSS: Instituto Mexicano del Seguro Social, ISSSTE: Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, SS: facilities of the Ministry of Health.
Figure 3 Distribution of health care providers and affiliation of the population who received care. Mexico, 2020
Among IMSS affiliates (42% of the total), only 49.1% received care at IMSS facilities, and 45.1% received care from private providers (13.1% in MOF). For ISSSTE affiliates (10% of the total), 35.7% received care from ISSSTE providers, and 57% from the private sector (10.4% in MOF). As for the uninsured population (45% of the total) with access to facilities of the SS, only 26.6% received care in such facilities, while 69.1% went to private offices (23.8% in MOF). Among the beneficiaries of other public institutions (1% of the total sample), 51.3% received care from their providers’ facilities, 17.5% at SS, and 28.5% in private facilities (6.5% in MOF). The population with private health insurance (1%) received care mostly from private providers (90.3%).
Figure 4 shows the distribution of health needs. As for the population that received care, 37% of their needs were acute; 26% were chronic; 13% were acute non-infectious; 15% sought preventive services; 3% sought mental health services, and 6% sought others (panel 2). Private and public facilities received different types of patients; private providers received more than twice the number of patients with acute illnesses (48%) than public providers (22%). However, chronic conditions were relatively rare in the private sector (18%) compared to the public health system (36%). Public facilities offered more preventive services (22%) than private ones (10%).
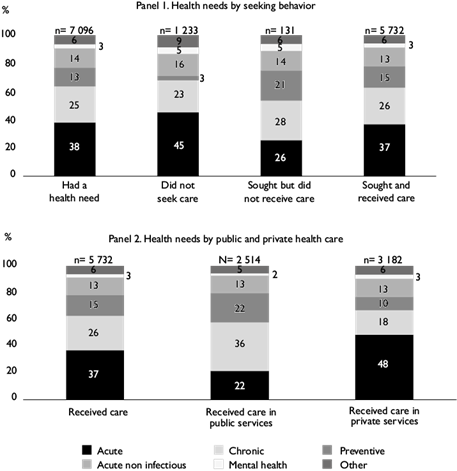
Note: Own estimations using data from the Encuesta Nacional de Salud y Nutrición, Covid-19 2020 on July 2021. Descriptive statistics used the complex survey design.
Figure 4 Distribution of health needs for different subgroups of the cascade of care
The distribution of the total population’s health needs differed from that of those who did not seek or receive care but was similar to that of those who received care (figure 4, panel 2.) People who did not seek health care had a higher percentage of acute conditions (45% vs. 38%) and lower preventive needs (3% vs. 13%). In contrast, those who sought but did not receive care had a lower percentage of acute needs (26%) and higher preventive needs (21%).
Table I shows the results of the probit regression models. In model 1, we estimated the association between receiving care in public health facilities (private as the reference) with sociodemographic characteristics. We found a negative association with being younger, with a 9% higher probability among people between 20 and 39 than among those aged 60 years or more. Those in secondary school had an 11% higher probability than people with no formal education. In contrast, we found a lower probability of receiving care in the public sector than in private clinics among the uninsured (29.6%) and among people in the high (11.5%) and medium (6.9%) socioeconomic tertiles compared to low SES. Finally, people currently employed were less likely (10.9%) to receive care in the public sector than the unemployed. We identified similar associations in model 2, in which we modeled the probability or receiving care in public health facilities versus receiving care in private care facilities or not receiving care at all.
Table I Probit regression models on sociodemographic factors associated with the probability of receiving care in public health facilities. Mexico, 2020
|
Variable |
Model 1. Receiving care in public vs. private facilities |
Model 2. Receiving care in public vs. private facilities or not receiving care |
|
Age (ref: 60+) |
||
|
20 to 39 |
-0.090* |
-0.074* |
|
[-0.136, -0.045] |
[-0.113, -0.036] |
|
|
40 to 59 |
-0.011 |
-0.016 |
|
[-0.051, 0.029] |
[-0.049, 0.018] |
|
|
Sex (ref: men) |
0.013 |
0.020 |
|
[-0.018, 0.045] |
[-0.007, 0.047] |
|
|
Education |
||
|
Primary school |
0.044 |
0.048 |
|
[-0.018, 0.106] |
[-0.005 - 0.101] |
|
|
Secondary school |
0.111‡ |
0.117* |
|
[0.043, 0.179] |
[0.058, 0.177] |
|
|
High school |
0.064 |
0.067§ |
|
[-0.012, 0.140] |
[0.001, 0.133] |
|
|
University or more |
-0.033 |
-0.007 |
|
[-0.106, 0.039] |
[-0.068, 0.055] |
|
|
Uninsured |
-0.296* |
-0.269* |
|
[-0.327, -0.264] |
[-0.295, -0.242] |
|
|
Socioeconomic level (ref: low) |
||
|
Medium |
-0.069* |
-0.033 |
|
[-0.110, -0.028] |
[-0.067, 0.001] |
|
|
High |
-0.115* |
-0.067* |
|
[-0.160, -0.070] |
[-0.105, -0.029] |
|
|
Currently employed |
-0.109* |
-0.093* |
|
[-0.142, -0.076] |
[-0.121, -0.064] |
|
|
Urbanicity (ref: urban) |
0.003 |
0.014 |
|
[-0.039, 0.044] |
[-0.021, 0.049] |
|
|
Observations |
4 632 |
5 785 |
Estimations by the authors using data from the Encuesta Nacional de Salud y Nutrición, Covid-19 2020 in July 2021. Confidence intervals in brackets.
*p<0.001
‡p<0.01
§p<0.05.
The estimations used the complex survey design.
Discussion
The Covid-19 pandemic disrupted the utilization of health care services in Mexico, as in other countries heavily hit by the SARS-CoV-2 virus. Our paper showed a drastic decrease in diabetes screening (61%) and testing (65%) in April 2020, for example. Even though these services slowly recovered during 2020, the coverage rates were still far from pre-pandemic levels by the end of the year.
Our paper focused mainly on the perspective of the households. We used data from the Ensanut Covid-19 2020, a nationally representative survey. Our analysis used the “cascade of care” framework to research the health issues experienced by the Mexican population and their choices to address them amid the Covid-19 pandemic. We found that 18.6% of the population reported health needs three months before the survey, and only 34% received care in public health facilities. The use of private health services was extensive even among the population with social security. Chronic conditions, particularly diabetes and hypertension control, were overrepresented among people who did not seek or receive care.
We cannot identify the magnitude of the displaced health care utilization due to Covid-19. The survey captures self-reported reasons not to seek or receive care, and it is difficult, if not impossible, for people to state how their decisions changed because of the pandemic. However, comparisons with previous years provide valuable insights. For example, the proportion of the population who received care in public health facilities was lower (34%) than in 2018 (41%).18 Furthermore, the proportion of the population with social security (affiliated to IMSS, ISSSTE, or other public institutions) that used the healthcare facilities of their affiliated institutions was lower in 2020 than in 2018 (28% vs. 29%).18 Lower utilization of health care in public facilities could be the consequence of some public hospitals being partially or fully dedicated to Covid-19 during the outbreak. Another possibility is that people were reluctant to attend public facilities for fear of getting infected. As in other studies in Mexico, we found that the uninsured population and those with high and medium socioeconomic status had a lower probability of using public health facilities,17,18 which suggests that people who had the means to use private services chose to do so.
Another insight into the displacement of health care utilization stems from the analysis of reasons behind the decision not to seek or receive care. For example, 55% of the people who did not seek care reported that their health condition was not severe --a significantly higher percentage than the 49% registered in 2018. Other people (3%) reported that the service was not available, which is possibly related to Covid-19, as explained above. Similarly, some of the reasons reported for not receiving care, such as “services not available” or the providers indicating that “the problem was not urgent” may also have been associated with a lack of resources to provide care for non-Covid-19 patients.
Moreover, we found reasons for not seeking or not receiving care more clearly linked to the Covid-19 pandemic. For example, “fear of contracting Covid-19” (11%), on the demand side, or the fact that the facilities “receive only Covid-19 patients” (19%), on the supply side (for those who did not received care, results not shown). There were also financial reasons from both the demand and the supply sides - “did not have money” and “unable to cover the cost,” respectively, which may or may not have been linked to the pandemic, although the economic impact of the epidemic in Mexico has been extensively documented.19
As for Mexico, studies from other countries show reductions in health care utilization of various services during the Covid-19 outbreak. Germany experienced reductions in outpatient services and hospitalization among older adults and decreases in the diagnosis of diabetes,8 similarly to our findings. In Singapore, a study showed reductions in medical outpatient visits associated with the fear of contracting Covid-19 at hospitals.5 The Netherlands experienced a decrease in preventive services in 2020 compared to the same period in 2019.7 Decreases in other types of resources for emergency care have been documented, such as the reduction in the use of medical ambulances for respiratory and trauma conditions in New Zealand.20
To our knowledge, our study is the first to document the status of health care utilization in a nationally representative sample of Mexicans within the context of the Covid-19 epidemic. Our results strongly suggest that the pandemic exacerbated problems and limitations of the public health care system in Mexico, which resulted in unequal access. Furthermore, our results document the extensive use of private services, some of them -provided by CAFs- of documented suboptimal quality and linked to higher out-of-pocket expenditures.18,21,22

