











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The A(H1N1) influenza pandemic began concurrently in Mexico and in the United States in 2009, but was widely referred to as the Mexican influenza. Eleven years later, Mexico had its first case of Covid-19 on February 28, 2020, 57 days after the first case of the disease was reported in Wuhan, China.1 As one of the first countries to be hit by the A(H1N1) virus, the experience of the epidemic for Mexicans was very different than for many other countries.2 Amid closed schools and universities, an online survey was conducted in May 2009 to determine the opinions, experiences, perception of risk, and impact on daily life that the A(H1N1) influenza epidemic had on the National Autonomous University of Mexico (UNAM, in Spanish)) community.3
The nature and scale of the Covid-19 epidemic, and the magnitude of its effects on multiple dimensions of daily life, lack of treatment and vaccine, among many other factors, is in stark contrast with the A(H1N1) pandemic. The comparison between the attributions, perceptions, and impact of the two pandemics on members of the same university community is relevant both to identify the differences and similarities on how the pandemics have been experienced and to be able to devise preparedness and responsiveness strategies for ongoing and future epidemic outbreaks in the largest university in Mexico, which is highly regarded and commonly taken as the benchmark for many others within and outside the country.
The objective of this study was to compare early phase pandemic perceptions and experiences of the influenza A(H1N1) in 2009 and the current Covid-19 (SARS-CoV-2) epidemic in the university population based on the analysis of their opinions, their knowledge of each epidemic, how they perceive the risks, their emotional reactions, the family, social and economic impact, preventive, information and social interaction practices, the implications that these factors had and are having on their daily lives, as well as their views on returning to work and study in both epidemics.
Materials and methods
Two surveys were conducted online: one during the A(H1N1) epidemic, from May 15 to 27, 2009 (22 days after the CDC confirmed the Mexican first case of the novel strain of influenza A[H1N1]), and the other during the Covid-19 pandemic, from April 6 to May 26, 2020 (37 days after the first case of Covid-19 was identified in Mexico). Students, academic and administrative staff from the university community were invited to participate and voluntarily agreed to respond to the survey published on the website of the UNAM. Located in Mexico City, UNAM is the most important university in Mexico, with more than 360 000 students from throughout the country.4 The difference in the online time duration of the two surveys was due to the fact that in the A(H1N1) one, the responses were faster because there was a greater availability of email addresses, and in the Covid-19 survey, there was a special interest in reaching a greater representativeness of the administrative staff which was more difficult to contact.
The A(H1N1) survey was conducted in two phases: the first phase consisted of the development and validation of the questionnaire titled Opinions of university students on the ‘new human influenza virus’ and its social effects (UNIV-Influenza).5 The second phase, which involved the collection of information from the questionnaire published on the UNAM home page, was initiated in May 2009. To conduct a comparative study between the two epidemics, we developed the UNIV-Covid-19 questionnaire in the first phase based on the adaptation of the UNIV-Influenza questionnaire, followed by a new validation.6 Additionally, some questions from previous studies conducted in China (Hong Kong) and the United Kingdom on the public response to the UK government recommendations on Covid-19 were included.7 Authorization was obtained in writing from the authors of both questionnaires. The questions were translated and adapted to the Mexican context following the methodology by Beaton, et al., who defines cross-cultural adaptation as a process that observe both parts of language and cultural adaptation in the process of preparing a questionnaire for use in other contexts.8
The UNIV-Covid-19 questionnaire includes 11 sections with 55 questions organized as follows: 1. Sociodemographic characteristics of the population (7 questions); 2. Knowledge of the epidemic (6 questions); 3. Means of information (3 questions); 4. Perception of risk and severity of the epidemic (5 questions); 5. Effects on mental health (20 questions); 6. Impact on mental health (2 questions); 7. Anxiety and Depression Scale (ADS, 15 questions); 8. Effects of the epidemic at the personal and family level (3 questions); 9. Current state of health, comorbidities and Covid-19 disease self-reported (4 questions); 10. Communication and relations with the university community (4 questions); 11. Preventive behaviors (6 questions). Seven of the eleven domains were analyzed for this study. Neither the anxiety and depression scale nor the health section were included; these will be reported in another paper. The internal consistency as evaluated by Cronbach’s alpha was reported in the different domains in a range of 0.89-0.67. In order to timely contribute with UNAM authority’s decision-making, a preliminary report was published where the content of all dimensions was specified.9
The questionnaire, including the explanation of the study objectives, was made accessible through a link from the landing page on the UNAM website. Emails were sent to available addresses of the university community asking to complete the questionnaire. The questionnaire was designed using free LimeSurvey software.
Ethical aspects
This project was approved by the UNAM authorities and by the ethics, research, and biosafety committees of the Hospital General de México Dr. Eduardo Liceaga under registration number DI/20/301/03/22. Recommendations of the Pan American Health Organization (PAHO) for research on the Covid-19 pandemic were also followed.10
Statistics analysis
A descriptive analysis of the demographics of the respondents who completed the entire questionnaire was carried out. Central tendency and dispersion measures were described for continuous variables and measurements of frequency for categorical variables. The normality of the variables was confirmed by the Shapiro-Wilk test. Inferential statistics tests were conducted to determine differences between the A(H1N1) and Covid-19 groups, including chi-square tests for nominal sociodemographic variables, and the Student’s t-test for continuous sociodemographic variables.
Results
A total of 24 998 participants from the UNAM community were recorded for the two pandemics: 12 840 (51.4%) for the first A(H1N1) survey in 2009 and 12 158 (48.6%) for the Covid-19 pandemic. We only analyzed the complete questionnaires that were approximately 60% in both surveys. Incomplete questionnaires were analyzed in order to identify potential biases among the participants considering age and gender (information available in 100% of the questionnaires).
Of the total number of participants in the A(H1N1) influenza and Covid-19 epidemics surveys, 7 432 (58%) and 7 497 (62%), respectively, were women; the average age was 33.1 (SD 1.9). The three groups of the university community were distributed as follows in the two epidemics A(H1N1) vs. Covid-19: students accounted for 64.7% of the sample (65.0 vs. 64.4%), academic staff 27.8% (30.6 vs. 24.8%) and administrative staff 7.4% (4.3 vs. 10.7%).
The highest level of age participation overall was in the range of 19 to 29 (28 vs. 48%) and 30 to 54 (29 vs. 32%) years of age, respectively, for each of the epidemics studied, with differences between the two surveys and within the three subpopulations. In the A(H1N1) survey the largest participation among students was in the group under the age of 18 (52%) compared to Covid-19, where the 19-29 age group predominated (71%). In the academic (69 vs. 59%) and administrative groups (79 vs. 74%), the age group with the highest level of participation was 30-54 years in both surveys but slightly higher for A(H1N1). In summary, with an 11-year difference between the A(H1N1) and Covid-19 surveys, the same university community had similar participation patterns.
Attribution of pandemic origin
In terms of the opinions on the origin attributed to the A(H1N1) and Covid-19 epidemics, the surveyed population was heterogeneously distributed across the three participating subpopulations. Opinions attributing the origin to human interventions in nature dominated the Covid-19 survey (25 vs. 18%), while biological changes were most often cited in the A(H1N1) survey (24 vs. 20%), especially in the academic staff group (29 vs. 23). Lack of hygiene was stated as the origin of the Covid-19 epidemic more frequently than that of influenza A(H1N1) (18 vs. 13%), and was particularly notable in the student group (20 vs. 14%). Genetic manipulation as a source was attributed more frequently to the A(H1N1) epidemic (29 vs. 12%) and was similarly distributed in all groups. Bioterrorism, climate, and social changes, as well as poverty, were mentioned by 7% of the participants.
We observed significant differences (p=0.000) in how the severity of the epidemics was perceived in Mexico and globally. Greater severity (very severe and severe) is perceived in the Covid-19 pandemic (83% for Mexico and 96% worldwide) compared to the A(H1N1) pandemic (55% for Mexico and 43% worldwide), with a similar frequency distribution pattern in the three university community groups (table I).
Table I Description of the attributed origin and severity of the epidemics A(H1N1) influenza and Covid-19 in a university community. Mexico City, 2009-2020
|
Students |
Faculty and Academic staff |
Administrative staff |
Total |
|||||||||
|
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
|
|
Total |
n=8 348(%) |
n=7 834(%) |
n=3 940(%) |
n=3 021(%) |
n=552(%) |
n=1 303(%) |
n=1 2840(%) |
n=12 158(%) |
||||
|
Origin of the Outbreak |
||||||||||||
|
Human interventions in nature |
491(16) |
1 891 (24) |
267(20) |
837(28) |
44(21) |
335(26) |
802(18) |
3 064 (25) |
||||
|
Biological changes |
671(22) |
1 534 (20) |
392(29) |
681(23) |
38(18) |
249(19) |
1 101 (24) |
2 464 (20) |
||||
|
Poor hygiene |
426(14) |
1 565 (20) |
139(10) |
396(13) |
26(13) |
173(13) |
591(13) |
2 134 (18) |
||||
|
Genetic manipulation |
899(30) |
927(12) |
368(27) |
339(11) |
64(31) |
224(17) |
1 331 (29) |
1 490 (12) |
||||
|
Bioterrorism |
211(7) |
581(7) |
39(3) |
162(5) |
10(5) |
119(9) |
260(6) |
862 (7) |
||||
|
Climate change |
221(7) |
466(6) |
61(5) |
251(8) |
19(9) |
91(7) |
301(7) |
807 (7) |
||||
|
Social changes |
27(1) |
478(6) |
11(1) |
187(6) |
0(0) |
72(6) |
38(1) |
737 (6) |
||||
|
Poverty |
39(1) |
392(5) |
66(5) |
169(6) |
6(3) |
39(3) |
111(2) |
600 (5) |
||||
|
Severity of the epidemic in Mexico |
||||||||||||
|
Very severe |
574(7) |
1 848 (24) |
269(7) |
891(29) |
55(10) |
448(34) |
898(7) |
3 187 (26) |
||||
|
Severe |
3 818 (46) |
4 505 (58) |
2 070 (53) |
1 673 (55) |
295(53) |
701(54) |
0.888 |
6 183 (48) |
6 879 (57) |
|||
|
Not very severe |
3 125 (37) |
1 461 (19) |
1 382 (35) |
451(15) |
168(30) |
152(12) |
4 675 (36) |
2 064 (17) |
||||
|
Not at all severe |
831(10) |
20(0) |
219(6) |
6(0) |
34(6) |
2(0) |
1 084 (8) |
28 (0) |
||||
|
Severity of the epidemic globally |
||||||||||||
|
Very severe |
550(7) |
4 596 (59) |
165(4) |
1 908 (63) |
54(10) |
876(67) |
769(6) |
7 380 (61) |
||||
|
Severe |
2 945 (35) |
2 834 (36) |
0.234 |
1 590 (40) |
998(33) |
233(42) |
378(29) |
4 768 (37) |
4 210 (35) |
|||
|
Not very severe |
3 624 (43) |
389(5) |
1 817 (46) |
112(4) |
218(39) |
49(4) |
5 659 (44) |
550(5) |
||||
|
Not at all severe |
1 229 (15) |
15(0) |
368(9) |
3(0) |
47(9) |
0(0) |
1 644 (13) |
18(0) |
||||
Chi-squared (χ2) test 44
* p<0.05, ‡ p<0.01, § p<0.001 (differences for influenza and Covid-19)
H0: p1=p2 vs. H1: p1≠p2
Reactions to the pandemic
Significant differences were observed in terms of the reactions to the pandemics. The interest in knowing more about the pandemic was the only reaction with a higher proportion for A(H1N1) influenza compared to Covid-19 (50 vs. 23%); worry (24 vs. 27%) and uncertainty (18 vs. 22%) were the predominant ‘initial’ reactions of the participants, and to a lesser extent anxiety (11 vs. 1%), alarm (5 vs. 9%), and fear (3 vs. 8%). Significant differences were also observed between perceived feelings ‘during’ the pandemics; worry was reported in a greater proportion during the A(H1N1) epidemic than during Covid-19 (41 vs. 18%), followed by anxiety (18 vs. 13%) and being alert (21 vs. 19%) (table II).
Table II Description of the emotions and first reaction expressed to epidemics A(H1N1) influenza and Covid-19, by groups in the university community. Mexico City, 2009-2020
|
Students |
Academic staff |
Administrative staff |
Total |
|||||||||
|
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
-value |
|
|
Total |
n=8 348 (%) |
n=7 834 (%) |
n=3 940 (%) |
n=3 021 (%) |
n=552 (%) |
n=1 303 (%) |
n=1 2840 (%) |
n=12 158(%) |
||||
| First reactions | ||||||||||||
|
Interest in knowing more about the problem |
3 029 (49) |
1 628 (21) |
1 763 (52) |
849 (28) |
214(47) |
307(24) |
5 006 (50) |
2 784 (23) |
||||
|
Worry |
1 230 (20) |
1 897 (24) |
1 029 (30) |
936(31) |
167(36) |
411(32) |
0.584 |
2 426 (24) |
3 244 (27) |
|||
|
Uncertainty |
1 381 (22) |
1 820 (23) |
421(12) |
637(21) |
53(12) |
277(21) |
1 855 (18) |
2 734 (22) |
||||
|
Anxiety |
60(1) |
979(12) |
12(0) |
219(7) |
2(0) |
101(8) |
74(1) |
1 299 (11) |
||||
|
Alarm |
332(5) |
824(11) |
118(3) |
195(6) |
15(3) |
91(7) |
465(5) |
1 110(9) |
||||
|
Fear |
209(3) |
687(9) |
35(1) |
185(6) |
8(2) |
116(9) |
252(3) |
988(8) |
||||
| Feelings during the pandemic | ||||||||||||
|
Worried |
2 504 (36) |
1 248 (16) |
1 861 (51) |
659(22) |
278(53) |
246(19) |
4 643 (41) |
2 153 (18) |
||||
|
Anxious |
1 527 (22) |
1 098 (14) |
421(12) |
339(11) |
0.477 |
55(11) |
147(11) |
0.405 |
2 003 (18) |
1 585 (13) |
||
|
Alert |
1 248 (18) |
1 200 (15) |
0.514 |
1 027 (28) |
796(26) |
0.790 |
129(25) |
281(22) |
0.392 |
2 404 (21) |
2 277 (19) |
0.991 |
|
Confused |
921(13) |
761(10) |
180 (5) |
178(6) |
31(6) |
99(8) |
0.126 |
1 132 (10) |
1 038(9) |
0.434 |
||
|
Fearful |
188(3) |
635(8) |
58(2) |
241(8) |
16(3) |
125(10) |
262(2) |
1 002(8) |
||||
|
Alarmed |
73(1) |
792(10) |
37(1) |
297(10) |
6(1) |
135(10) |
116(1) |
1 224 (10) |
||||
|
Isolated |
591(8) |
1 187 (15) |
70(2) |
387(13) |
8(2) |
183(14) |
669(6) |
1 757 (14) |
||||
|
Bored |
913(12) |
123(4) |
86(7) |
1 122(9) |
||||||||
Chi-squared (χ2) test
* p<0.05, ‡ p<0.01, § p<0.001 (differences for influenza and Covid-19)
H0: p1=p2 vs. H1: p1≠p2
Effects of the pandemics
The Covid-19 pandemic has had a greater impact on the family economy compared to A(H1N1) (53 vs. 41%), with higher proportions observed in the student group (61 vs. 48%), followed by administrative staff (47 vs. 37%), and academic staff (34 vs. 27%). The impact on family life is similarly distributed across the options of ‘none,’ ‘positively,’ and ‘negatively’ in the Covid-19 group. This pattern differs from that reported in A(H1N1), in which 55% reported having had no family impact and 6% reported that it had a negative effect (data not shown).
Type of support received
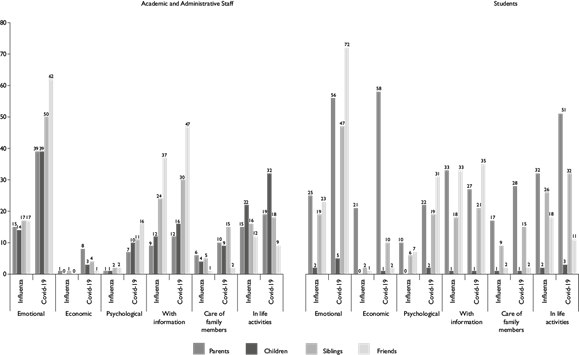
Figure 1 illustrates the support received by groups of participants in both surveys. Academic and administrative staff and students received more support of different type (emotional, economic, psychological, information, family care, and daily life activities) in the Covid-19 epidemic, specifically in emotional, psychological, and informational support, with the latter coming mainly from friends, while support in finances, family care, and daily life activities came from family members (parents, children, siblings).
Preventive measures
The rate of preventive behaviors increased during the Covid-19 pandemic. The most frequently and differentially reported actions in Covid-19 compared to A(H1N1) were: frequent hand washing (98 vs. 91%), avoiding gathering in groups (91 vs. 54%), not greeting with a handshake or a kiss (88 vs. 47%), avoiding public places (87 vs. 66%), avoiding public transport (75 vs. 38%), avoiding touching the face (75 vs. 47%), and cleaning surfaces (58 vs. 33%). The use of face masks was similar in both pandemics (68 vs. 65%) (table III).
Table III Comparison of preventive measures and actions by the group to address the Covid-19 and influenza A(H1N1) epidemics in the university community. Mexico City, 2009-2020
|
Students |
Academic staff |
Administrative staff |
Total |
|||||||||
|
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
|
|
Total |
n=8 348 (%) |
n=7 834 (%) |
n=3 940 (%) |
n=3 021 (%) |
n=552 (%) |
n=1 303 (%) |
n=12 840 (%) |
n=12 158 (%) |
||||
|
Preventive measures during the pandemic |
||||||||||||
|
Frequent hand washing |
7 381 (88) |
7 631 (97) |
3 770 (96) |
2 970 (98) |
534(97) |
1 277 (98) |
0.102 |
11 685 (91) |
11 878 (98) |
|||
|
Avoiding gathering in large groups |
3 879 (46) |
7 097 (91) |
2 737 (69) |
2 822 (93) |
358(65) |
1 180 (91) |
6 974 (54) |
11 099 (91) |
||||
|
Avoiding greeting with a handshake or a kiss |
2 699 (32) |
6 686 (85) |
2 888 (73) |
2 864 (95) |
408(74) |
1 199 (92) |
5 995 (47) |
10 749 (88) |
||||
|
Avoiding closed or open public spaces |
4 846 (58) |
6 776 (86) |
3 133 (80) |
2 668 (88) |
440(80) |
1 129 (87) |
8 419 (66) |
10 573 (87) |
||||
|
Avoiding public transport |
2 448 (29) |
5 743 (73) |
2 154 (55) |
2 350 (78) |
267(48) |
974(75) |
4 869 (38) |
9 067 (75) |
||||
|
Avoiding touching the face (eyes, nose, and mouth) |
3 374 (40) |
5 575 (71) |
2 322 (59) |
2 486 (82) |
339(61) |
1 064 (82) |
6 035 (47) |
9 125 (75) |
||||
|
Using face mask or cover |
5 327 (64) |
5 239 (67) |
2 620 (66) |
1 983 (66) |
0.454 |
359(65) |
1 027 (79) |
8 306 (65) |
8 249 (68) |
|||
|
Cleaning surfaces (handrails, doorhandles, etc.) at home |
2 425 (29) |
4 222 (54) |
1 592 (40) |
1977 (65) |
273(49) |
902(69) |
4 290 (33) |
7 101 (58) |
||||
Chi-squared (χ2) test
* p<0.001 (differences for influenza and Covid-19)
H0: p1=p2 vs. H1: p1≠p2
Following and trusting sources of information about the pandemic
Variations between epidemics were found on the primary sources of information for A(H1N1) and Covid-19: 1. television, 42 vs. 55%; 2. internet sites, 14 vs. 54%; 3. UNAM website, 11 vs. 44%; 4. press, 8 vs. 41%; 5. social media, 0 vs. 65%; 6. Ministry of Health press conferences, 0 vs. 60%. The sources that participants trusted most during the A(H1N1) and Covid-19 epidemics were respectively: 1. UNAM website, 58 and 76%; 2. internet sites, 23 and 30%; 3. newspapers, 20 and 20%; 4. radio news, 16 and 17%.
Uncertainty and preparation for return
Participants reported greater uncertainty about potential infection when returning to classes in the current pandemic compared to A(H1N1) influenza (47 vs. 8%), being slightly higher in the administrative staff group. A similar response was observed in the perception of the university’s preparedness for the return to classes (Covid-19, 32% vs. A(H1N1), 63%) (table IV).
Table IV Comparison of preparation for the return to the university by the group to address the Covid-19 and influenza A(H1N1) epidemics in the university community. Mexico City, 2009-2020
|
Students |
Academic staff |
Administrative staff |
Total |
|||||||||
|
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
Influenza |
Covid-19 |
p-value |
|
|
Total |
n=8 348 (%) |
n=7 834 (%) |
n=3 940 (%) |
n=3 021 (%) |
n=552 (%) |
n=1 303 (%) |
n=1 2840 (%) |
n=12 158 (%) |
||||
|
Uncertainty about the return to the university |
||||||||||||
|
Very high and high |
630 (8) |
3 491 (46) |
413 (8) |
1 358 (47) |
48 (9) |
680 (54) |
1 091 (8) |
5 529 (47) |
||||
|
Moderate |
2 268 (27) |
2 904 (39) |
1 663 (32) |
1 027 (35) |
223 (40) |
398 (32) |
4 154 (32) |
4 329 (37) |
||||
|
Low |
3 277 (39) |
767 (10) |
1 393 (38) |
260 (9) |
189 (34) |
105 (8) |
4 859 (38) |
1 132 (10) |
||||
|
None |
1 823 (22) |
69 (1) |
312 (17) |
17 (1) |
66 (12) |
12 (1) |
2 201 (17) |
98 (1) |
||||
|
Don’t know |
350 (4) |
293 (4) |
0.141 |
159 (4) |
239 (8) |
26 (5) |
58 (5) |
0.806 |
535 (4) |
590 (5) |
||
|
The university is prepared for the return |
||||||||||||
|
Yes |
5 559 (67) |
2 115 (28) |
2 131 (63) |
1 099 (38) |
375 (68) |
570 (45) |
0.000 |
8 065 (63) |
3 784 (32) |
|||
|
No |
1 037 (12) |
2 992 (40) |
890 (16) |
816 (28) |
100 (18) |
309 (25) |
2 027 (16) |
4 117 (35) |
||||
|
Don’t know |
1 752 (21) |
2 415 (32) |
919 (21) |
985 (34) |
77 (14) |
374 (30) |
2 748 (21) |
3 774 (32) |
||||
Chi-squared (χ2) test
* p<0.01, ‡ p<0.001 (differences for influenza and Covid-19)
H0: p1=p2 vs. H1: p1≠p2
Discussion
This is the first reported study from a major public university in Mexico comparing the experiences of the university community during the A(H1N1) influenza pandemic immediately after it was originated in Mexico and the early months of the Covid-19 pandemic. In light of the anthropological interpretive approach, differences between pandemics were expected, since experiences encompass the interpretation, meaning and values of an event at a particular time and context.11 In this sense, in the event of a pandemic, the perceived risk plays a key role in the experience since it involves the resources and the individual’s ability to cope with events.12
The comparison reveals greater impact of the Covid-19 pandemic on all explored aspects, i.e., the perception of severity, the attributed origin, reactions, effects, types of support, uncertainty, and lack of confidence in safe reopening, as well as on trusting and following sources of information. These differences can be explained by diverse reasons, history, the properties of the viruses, the rapid evolution of the Covid-19 pandemic and its greater case-fatality rate as well as longer duration, as the pandemic thus far has been going on for one year after the first case in Mexico. It is important to consider that part of the academic and administrative staff that participated in the A(H1N1) survey may have also participated in the Covid-19 survey. However, the experience of the first pandemic is not reflected in important differences between the two surveys. Hence, there seem to be no effects due to the accumulated experience of living both pandemics. This cannot be directly documented with this study.
The perception of risk and experiences concerning SARS-CoV-2 virus differs widely among individuals and places.13 However, the history of 11 years ago with the A(H1N1) influenza seems to have repeated itself in the Covid-19 epidemic.
More women than men (59.2 vs. 40.8%) participated in the two surveys analyzed here; this is in line with other Covid-19 surveys, e.g., among medical and high school students (69.6%).14,15 Similar findings were reported in the survey administered to the Mexican population to estimate the stress levels during the Covid-19 pandemic, in which female participation was 72%,16 and 65.7% in an open population.17 During the A(H1N1) influenza (48.2%) this participation was lower.18 However, gender differences in the perception of severity or preventive actions are inconclusive. In their study Taghrir, et al.14 found that women reported a lower perception of risk compared to men; for instance, Pérez-Gay, et al.16 reported that women expressed having higher levels of stress during the Covid-19 pandemic, while in Cao, et al.15 no gender differences were identified. Despite discrepancies in publications about differences in the perception of severity by women and men during the pandemics, it is important to highlight the greater psychosocial impact experienced by women due to confinement during Covid-19 that has resulted in a negative impact on their well-being and safety globally,19 in Mexico,20 and specifically in the university population survey here analyzed.21
As was observed above, the origin of the pandemics described by the participants is associated with a loss of the relationship between humans and nature (an ecological sense), to the extent that this loss is what has conditioned the onset of these epidemics; however fewer participants related the pandemics to social aspects and natural factors predominated.
The perception of severity in the early stages of both epidemics was high, although it was higher in the Covid-19 pandemic (83 vs. 55%); this is partly due to the time and manner in which the epidemics appeared in Mexico. On April 12, 2009, Mexico reported an outbreak of respiratory diseases to the PAHO and on April 17, Mexican authorities issued an epidemiological alert after sending samples to the CDC, which on April 23 confirmed the novel A(H1N1).22 Mexico had a timely response: on that same day Mexico reported it to the World Health Organization (WHO), declared a national health emergency and suspended activities including classes at UNAM.23 On April 30, WHO declared it a public health emergency of international concern and on June 11 it was declared a pandemic.24
The UNIV-Influenza survey was conducted in the days leading up to the WHO declaration of the pandemic. This is in contrast to the UNIV-Covid-19 survey, which was conducted at the time when it was assumed that Mexico had reached a peak in cases after the virus was first reported in China in December 2019 with the declaration of pandemic by WHO on January 30, 2020.1,2,24 Several factors that may explain the perception of severity of pandemics include knowledge, visibility, trust, catastrophic potential, equity, immediacy of danger, and controllability.13 The knowledge and control of A(H1N1) influenza developed much more rapidly than with Covid-19; these factors, along with differences in mortality, visibility of risk, and confidence in its controllability explain a higher perception of the risk of returning to classes for Covid-19 (47%) compared to A(H1N1) influenza (7%).
The fatality from Covid-19 globally and to a greater extent in Mexico due to comorbidities among other factors,25 is one of the mechanisms associated with the perception of severity of this virus. In this study the controllability associated with trust was observed in the participants’ perception of risk of infection in returning to classes, which was higher for Covid-19 (47%) compared to A(H1N1) influenza (7%), largely due to knowledge of the virus propagation rate and the availability of treatment and vaccine, hence, a higher sense of control.
As expected, the main sources of information changed for Covid-19 pandemic, mainly due to the increase in the diversity and availability of sources for real-time interactions, e.g., social media vs. newspapers and radio; these results are consistent with the use of the internet and social media as the main sources of information for the university students, followed by radio and television.26
In the university community studied, the university website was mentioned as the most reliable source of information for both pandemics, more so in Covid-19. This is in stark contrast with findings in the general population as illustrated by the results in Hong Kong, where the most reliable sources of information were physicians (84%) and radio broadcasts (57%).27
Anxiety about the Covid-19 pandemic has been reported in 24.9% (13), and 37.4% (27) of high school students in China,28 higher than that observed in this study, where only 13% overall mentioned feeling anxious, although almost half of the students reported a high degree of anxiety.9 The COVIDiSTRESS Global Survey of 52 countries reports that the first source of stress in Mexico was the national economy, followed by the risk of Covid-19 infection, and to a lesser extent hospitalization.16 The adverse psychological effects, including symptoms associated with stresses, from secondary quarantines to infectious diseases, is a phenomenon documented in the past. However, when compared to students who were quarantined against those who were not, no significant differences in mental health symptoms were observed; the difference in quarantines from this Covid-19 pandemic and the previous ones (N1H1, SARS in others) is the duration of it, and this would potentially explain the different impact on students’ mental health.29
The impact at both the individual and family levels has been felt to a greater extent during the Covid-19 epidemic; this situation indicates an economic precariousness experienced by the students of the largest public university in the country when facing critical situations such as pandemics which again is consistent with the results of the COVIDiSTRESS study.
For members of the university community, the negative impact on family life has been greater in the Covid-19 pandemic than during A(H1N1) influenza. The stricter and more extended confinement policies of the current epidemic have encouraged closer family coexistence with more positive (38%) than negative (25%) effects reported.9 Studies have documented a sharp increase in domestic violence during the lockdown,19 although at the same time a positive coexistence has been identified in both epidemics. The complexities of fast-paced life often leave little time for the family; in contrast, moments of crisis can increase family solidarity and reinforce family ties. Epidemics underscore family complexity within the context of today’s world, especially in times of uncertainty and vulnerability.29
Overall, in both epidemics, the prevention measure to which respondents most adhered was handwashing, being lower for the A(H1N1) epidemic (91%) vs. Covid-19 (98%), a result that is similar to other studies where 88% was reported.18,30 Some differences were observed among subpopulations within the university community.
The COVIDiSTRESS survey reports that in Mexico most have done their best to respect social distancing in public spaces.16 In this respect there is a marked difference between the two epidemics. Social distancing (avoiding group gatherings and crowded places) has been greater for the Covid-19 epidemic, similar to that reported in a Chinese study (96.4%);17 however, for the influenza epidemic A(H1N1) it was lower in Mexico (54%) than that reported in another study in students in the United Kingdom (65%).31
Face masks are reported as one of the measures followed by about 60% of the respondents. This differs from that reported in other studies of university students in relation to the Covid-19 epidemic, where this measure is reported less frequently,26 but is higher in the Chinese population where 98% reported using face masks,17 and what has been documented for the A(H1N1) influenza epidemic, in which only 31.8% reported using face masks.18 Cultural, social, and political variations account for differentials in adherence to public health measures.
Limitations
This study has several limitations, from the cross-sectional design where causal associations cannot be described. The problems of the online nature of the surveys, together with the differences in the length of time online of the two surveys, could have had a potential participation bias due to accessibility and use of technology, among others factors, and memory bias. Generalizations for other non-university populations cannot be made.32 The online time of the Covid-19 survey was prolonged as the participation of administrative staff was slow at the beginning.
Strengths
This study has a large sample, analyzed with a similar methodology and taken from within the same university community that did not varied across the demographic spectrum, with a difference of 11 years, thus allowing for comparability between the A(H1N1) influenza pandemic (that began almost simultaneously in Mexico and the United States) and the Covid-19 pandemic. As a university community preparedness strategy to guide actions for future pandemics, it provides a validated questionnaire that may be reproduced in Mexico and Latin America to timely collect the information from early or later phases of an epidemic.30,33,34,35 In addition, a therapeutic effect and community connection may be identified by means of the opinions expressed in the questionnaire’s open question.
Conclusions
The perceptions and experiences of the influenza A(H1N1) and Covid-19 pandemics were similar; however, the impact of the Covid-19 pandemic has been much greater, especially in terms of the perception of severity, adoption of preventive measures, impact on the family economy, anxiety, and uncertainty regarding the safe return to school. Pandemic preparedness and responsiveness in universities must include research on the agenda of strategies.

