











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The SARS-CoV-2 epidemic in Mexico is growing, with 1 070 487 cases and 103 597 deaths registered by November 25th, 2020.1 In Mexico, on March 23rd (and until May 30th) a call for a nationwide lockdown was made.2,3 On June 1st, Mexico implemented postlockdown mitigation strategies that, depending on community transmission and hospital capacity, eased some of the initial restrictions.4 In order to understand the transmission of SARS-CoV-2 under different mitigation strategies, it is important to study the role that different age groups have played on propagating the spread of the virus. Variations in transmission of SARS-CoV-2 by age may take place during the course of an epidemic due to changing mixing patterns,5 with subsequent implications for epidemic control.
Evidence has accumulated that susceptibility to SARS-CoV-2 infection increases with age.6,7 Yet, this does not suggest that the oldest groups in a population necessarily play the leading role in the spread of SARS-CoV-2 in the community. Actually, several serological studies suggest that adolescents and younger adults often experience the highest cumulative rates of infection.8,9,10,11,12,13,14,15 In England, the highest rates of SARS-CoV-2 infection during the fall of 2020 occurred in individuals aged 13-17y and 18-24y (figure 8 in reference 16).16 Under the physical distancing measures implemented in Mexico, mixing patterns among individuals of different age groups may be quite different from the regular mixing patterns.5,6 Also, similarly to other low- and middle-income countries, a sizeable proportion of Mexico’s population consists of relatively young informal workers who live from day to day, for whom shelter-in-place policies may represent a significant economic burden. The role that older adolescents, younger adults and other age groups play in propagating the SARS-CoV-2 epidemic in Mexico is unknown. In order to address this issue, we estimated temporary changes in SARS-CoV-2 incidence by age group during and after the national lockdown period. We applied the methodology developed previously17,18,19 to assess the temporal changes in the incidence of different age groups of individuals between the ages of 10 to 59 years during the epidemic in Mexico.
Materials and methods
Data sources
Information on daily hospitalized Covid-19 cases by age group was obtained from the General Directorate of Epidemiology (Dirección General de Epidemiología) of the National Epidemiological Surveillance System (Sisver, by its acronym in spanish) in Mexico. We retrieved data on reported hospitalized cases of PCR-confirmed SARS-CoV-2 infection, along with available information on the date of symptom onset (September 28, 2020). We excluded healthcare workers because of the significant non-community transmission in that population group. We also excluded cases from private hospitals because it is unclear how cases were ascertained and whether case-ascertainment has changed over time. Finally, we excluded non-hospitalized cases because testing for non-severe Covid-19 may have changed over time for different age groups, while the criteria for testing of cases requiring hospitalization for SARS-CoV-2 infection have been consistent over time.
Relative change in SARS-CoV-2 infection by age-group
We included laboratory confirmed hospitalizations in ten 5-year age groups: 10-14 years through 55-59 years. Older adults were not included because of potential temporal changes in ascertainment, as well as presence of some hospitalizations stemming from infections that do not reflect community transmission (e.g., infections in long-term care facilities, with rates of infection in those facilities being quite higher than in the corresponding age groups in the community). We also excluded children under 10 years for two reasons: first, ascertainment of infection in those age groups might have changed with time as more severe episodes in younger children appeared as the epidemic progressed; second, there is evidence of lower susceptibility to infection in children aged under 10 years compared to adults and older adolescents,20 so these children are unlikely to play a significant role in the progression of the epidemic.
We selected three periods: April 20-May 3 (early lockdown period; we selected this date because earlier numbers of cases in certain age groups were limited and may have rendered our estimates unstable), 18-31 May (late lockdown period, the end of the national lockdown) and 15-25 June (post-lockdown period, starting two weeks after the national lockdown, in order to detect changes in symptom onset).
We applied a previously described procedure17,18,19 for estimating the age-specific proportion ratios for late lockdown (May 18-31, 2020) and post-lockdown (June 15-28, 2020) periods, relative to the early lockdown (April 20-May 3, 2020), as follows: let E(g) be the number of hospitalization with confirmed SARS-CoV-2 infection in age group g and
That is, the ratio between the proportion of cases in age group g among all cases in the late lockdown period and the proportion of cases in age group g in the early lockdown. The logarithm ln(PR(g)) of the PR(g) is approximately normally distributed21 with the standard error:
We repeated these calculations after substituting the cases in the late lockdown with the cases in the post-lockdown period.
In order to examine whether the PR in certain age groups is significantly higher than in others, we consider the corresponding pairwise odds ratios (ORs). For each pair of age groups g1 and g2, the proportion ratios PR(g1) and PR(g2) are compared using the odds ratio (OR):
It follows from equation 1 that OR(g1,g2) equals:
Which is the OR for a hospitalized case of confirmed SARS-CoV-2 infection occurring in age group g1 vs. g2 for the early lockdown period and the late lockdown period. We repeated these calculations for the comparison of early lockdown to post-lockdown. Estimates for pairwise OR were made using Fisher’s exact test.
Results
Table I shows the number of hospitalizations for confirmed SARS-CoV-2 infection in the different age groups (10-14 through 55-59 years) during the early lockdown (April 20-May 3, 2020), the late lockdown (May 18-31, 2020) and the post-lockdown (June 15-28, 2020) periods, as well as the corresponding estimates of the PR statistic (equations 1,2).
Table I: Number of hospitalizations for confirmed SARS-CoV-2 infection by age groups (10-14 through 55-59 years) and by time period, and estimates of the prevalence ratio (PR) statistic (n=23 013). Mexico, 2020
|
Age Group, y |
Early lockdown period |
Late lockdown period |
Post-lockdown period |
Prevalence Ratio PR (95%CI) |
||||
|
April 20-26 |
April 27 - May 3 |
May 18-24 |
May 25-31 |
June 15-21 |
June 22-28 |
Late vs. early lockdown period |
Post-lockdown vs. early lockdown period |
|
|
10-14 |
9 |
7 |
13 |
16 |
28 |
21 |
1.13 (0.62-2.09) |
1.66 (0.94-2.91) |
|
15-19 |
11 |
12 |
35 |
27 |
45 |
42 |
1.69 (1.05-2.72) |
2.05 (1.30-3.24) |
|
20-24 |
34 |
44 |
87 |
91 |
115 |
100 |
1.43 (1.10-1.86) |
1.49 (1.15-1.93) |
|
25-29 |
103 |
108 |
195 |
179 |
216 |
199 |
1.11 (0.94-1.31) |
1.07 (0.91-1.25) |
|
30-34 |
164 |
186 |
288 |
276 |
347 |
355 |
1.01 (0.89-1.15) |
1.09 (0.96-1.23) |
|
35-39 |
251 |
239 |
385 |
430 |
461 |
454 |
1.04 (0.94- 1.16) |
1.01 (0.91-1.12) |
|
40-44 |
330 |
385 |
559 |
555 |
620 |
587 |
0.98 (0.89-1.06) |
0.91 (0.84-1.00) |
|
45-49 |
465 |
547 |
741 |
747 |
869 |
878 |
0.92 (0.86-0.99) |
0.93 (0.87-1.00) |
|
50-54 |
555 |
581 |
865 |
902 |
1 030 |
957 |
0.97 (0.91-1.04) |
0.95 (0.89-1.01) |
|
55-59 |
544 |
603 |
915 |
968 |
1 114 |
1 123 |
1.03 (0.96-1.10) |
1.06 (0.99-1.12) |
|
Total |
2 466 |
2 712 |
4 083 |
4 191 |
4 845 |
4 716 |
||
For the late lockdown vs. the early lockdown period, the highest PR (95%CI) estimates correspond to individuals aged 15-19 years (PR=1.69 [1.05,2.72]) and 20-24 years (PR=1.43[1.10,1.86]) (table I). The PR estimates in individuals aged over 30 years were significantly lower compared to individuals aged 15-24 years. Table II gives the estimates of ORs for different pairs of age groups (10-14y through 55-59y) for hospitalized cases of confirmed SARS-CoV-2 infection occurring during the period May 18-31 vs. April 20-May 3 (equation 3, 4). Our results suggest that, for individuals aged 15-24y, the corresponding OR relative to any age group over 30y is above 1 (table II).
Table II: Odds ratios for different pairs of age groups for a hospitalized case of confirmed SARS-CoV-2 infection occurring between the late lockdown (May 18-31) vs. the early lockdown period (April 20-May 3). Mexico, 2020
|
15-19 |
20-24 |
25-29 |
30-34 |
35-39 |
40-44 |
45-49 |
50-54 |
55-59 |
|
|
10-14 |
0.67 (0.29-1.58) |
0.79 (0.39-1.66) |
1.02 (0.52-2.06) |
1.12 (0.58-2.25) |
1.09 (0.57-2.17) |
1.16 (0.61-2.31) |
1.23 (0.64-2.44) |
1.17 (0.61-2.31) |
1.10 (0.58-2.19) |
|
15-19 |
1.18 (0.67-2.15) |
1.52 (0.90-2.65) |
1.67 (1.00-2.88) |
1.62 (0.97-2.78) |
1.73 (1.05-2.95) |
1.83 (1.11-3.12) |
1.73 (1.05-2.95) |
1.64 (1.00-2.79) |
|
|
20-24 |
1.29 (0.93-1.79) |
1.42 (1.04-1.93) |
1.37 (1.02-1.86) |
1.46 (1.10-1.97) |
1.55 (1.17-2.08) |
1.47 (1.11-1.96) |
1.39 (1.05-1.86) |
||
|
25-29 |
1.10 (0.88-1.37) |
1.07 (0.87-1.31) |
1.14 (0.93-1.39) |
1.21 (1.00-1.46) |
1.14 (0.94-1.38) |
1.08 (0.89-1.30) |
|||
|
30-34 |
0.97 (0.81-1.16) |
1.03 (0.88-1.22) |
1.10 (0.94-1.28) |
1.04 (0.89-1.21) |
0.98 (0.84-1.14) |
||||
|
35-39 |
1.07 (0.92-1.24) |
1.13 (0.98-1.30) |
1.07 (0.93-1.23) |
1.01 (0.88-1.16) |
|||||
|
40-44 |
1.06 (0.93-1.20) |
1.00 (0.89-1.13) |
0.95 (0.84-1.07) |
||||||
|
45-49 |
0.95 (0.85-1.06) |
0.90 (0.80-1.00) |
|||||||
|
50-54 |
0.95 (0.85-1.05) |
Odds ratios (ORs) for different pairs of age groups (10-14y through 55-59y) for hospitalized cases of confirmed SARS-CoV-2 infection in Mexico occurring during the May 18-31 period vs. April 20-May 3 (equation 4).
For the post-lockdown vs. the early lockdown period, the highest PR estimates (95%CI) corresponded to individuals aged 15-19 years (PR=2.05[1.30,3.24]) and 20-24 years (PR=1.49 [1.15,1.93]) (table I). The PR estimates for individuals aged over 30 years were significantly lower than those for individuals aged 15-24 years. Table III shows the estimates of ORs during the post-lockdown period of June 15-28 vs. the lockdown period April 20-May 3. The corresponding OR for individuals aged 15-24y relative to any age group over 30y is significantly above 1 for the post-lockdown period compared to the early lockdown period. This suggests a relative increase in the incidence of SARS-CoV-2 infection in individuals aged 15-24y, compared to those aged 30-59y for the post-lockdown period relative to the early lockdown period.
Table III: Odds ratios for different pairs of age groups for hospitalized cases of confirmed SARS-CoV-2 infection occurring between the post-lockdown (June 15-18) vs. the early lockdown period (April 20-May 3). Mexico, 2020
|
15-19 |
20-24 |
25-29 |
30-34 |
35-39 |
40-44 |
45-49 |
50-54 |
55-59 |
|
|
10-14 |
0.81 (0.37-1.80) |
1.11 (0.58-2.19) |
1.56 (0.85-3.00) |
1.53 (0.84-2.92) |
1.64 (0.91-3.12) |
1.81 (1.00-3.44) |
1.77 (0.99-3.36) |
1.75 (0.97-3.31) |
1.57 (0.87-2.97) |
|
15-19 |
1.37 (0.79-2.44) |
1.92 (1.16-3.28) |
1.89 (1.16-3.18) |
2.03 (1.25-3.40) |
2.24 (1.39-3.75) |
2.19 (1.36-3.66) |
2.16 (1.34-3.61) |
1.94 (1.21-3.24) |
|
|
20-24 |
1.40 (1.02-1.93) |
1.37 (1.02-1.86) |
1.48 (1.11-1.98) |
1.63 (1.23-2.18) |
1.60 (1.21-2.12) |
1.58 (1.20-2.09) |
1.41 (1.07-1.87) |
||
|
25-29 |
0.98 (0.79-1.22) |
1.05 (0.86-1.29) |
1.17 (0.96-1.42) |
1.14 (0.94-1.37) |
1.12 (0.93-1.35) |
1.01 (0.84-1.21) |
|||
|
30-34 |
1.07 (0.90-1.28) |
1.19 (1.01-1.40) |
1.16 (1.00-1.35) |
1.15 (0.99-1.33) |
1.03 (0.89-1.19) |
||||
|
35-39 |
1.11 (0.96-1.28) |
1.08 (0.94-1.24) |
1.07 (0.93-1.22) |
0.96 (0.84-1.09) |
|||||
|
40-44 |
0.98 (0.87-1.11) |
0.97 (0.86-1.09) |
0.87 (0.77-0.97) |
||||||
|
45-49 |
0.99 (0.89-1.10) |
0.89 (0.80-0.98) |
|||||||
|
50-54 |
0.90 (0.81-0.99) |
Odds ratios (ORs) for different pairs of age groups (10-14y through 55-59y) for hospitalized cases of confirmed SARS-CoV-2 infection in Mexico occurring during the period of June 15-28 vs. April 20-May 3 (equation 4).
Discussion
We applied the previously developed methodology17,18,19 to study changes in the relative incidence of SARSCoV-2 infections in different age groups during national lockdown and post-lockdown in Mexico. Compared with early lockdown, the greatest relative increase in the incidence of infection belongs to persons aged 15-24 years in both the late lockdown and post-lockdown periods. We note that, in England, the highest rates of SARS-CoV-2 infection during the Fall of 2020 are found among individuals aged 18-24y and 13-17y (figure 8 in reference 16),16 consistently with our findings about the epidemiological importance of older adolescents and younger adults during the epidemic.
We hypothesize that there are two potential explanations for the increase in the incidence of SARS-CoV-2 infection in older adolescents and younger adults in Mexico: 1) the need for young informal workers to return to work due to increasing economic burden of physical distancing measures and 2) fatigue from adhering to the physical distancing measures, resulting in less and less adherence. Other explanations, such as changing social responsibilities and increased use of public transportation may also apply, and further work is required to understand those issues in order to better inform future mitigation efforts. A serological evaluation that may confirm our observations is underway.
Our results are consistent with observations carried out in Germany, where, with the same methodology, a higher relative incidence of infection was found in older adolescents and younger adults following the introduction of physical distancing measures.17
In Spain, applying the same methodology that was used in source,17 individuals aged 40-64 years were observed to have a higher relative incidence of infection during the initial lockdown period, when non-essential work was allowed, than in the pre-lockdown period. However, during the later strengthened lockdown, older adolescents and younger adults had an increased relative incidence of SARS-CoV-2 infection.22 Our results, together with these observations, highlight the fact that control measures during a pandemic have differential effectiveness in different age groups.
Our study is not without limitations. However, our study is not without limitations. Our findings may be affected by age-differential changes in case ascertainment, over time, or across regions. However, we restricted the analysis to hospitalized cases, rather than including all confirmed Covid-19 cases in the community, because changes in healthcare seeking behavior (e.g., for ambulatory visits) and changes in testing in the outpatient setting may affect the relation between the incidence of SARS-CoV-2 infection and the rates of detected Covid-19 cases. However, such temporary changes are less likely to occur in hospitalized cases, as uniform guidelines for testing hospitalized cases are applied in Mexico and there is a low likelihood of mild cases resulting in hospitalization during certain time periods. Second, the perception of the potential severity of the disease may have changed over time, and clinicians, even with an existing case definition, may have preferentially tested certain age groups. We explored whether testing for hospitalized patients in all age groups had changed over time and found no evidence for this (figure 1). Third, we used the date of symptom onset to temporally classify cases from an administrative database. Thus, the possibility of error in registration is present; however, this error is probably random and unlikely to affect results. Alternatively, there might be differences across age groups in their recall of the date of onset, yet this seems unlikely. Fourth, it is important to notice that the database from the Ministry of Health is not updated over time. In other words, we do not know whether a case that was originally registered as an ambulatory case was later hospitalized.
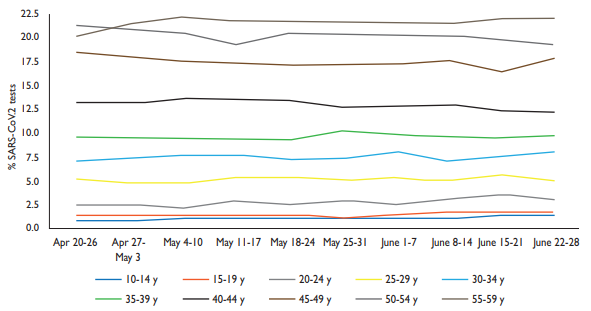
Figure 1 Trends in the distribution of SARS-CoV-2 tests (RT-PCR) by age group among hospitalized individuals. Mexico, 2020
In conclusion, our paper provides evidence for an increased relative incidence of SARS-CoV-2 infection among individuals aged 15-24 years when the lockdown interventions were lifted. Our results suggest that the age structure was an important factor in the effect of lockdown interventions. Multigenerational
household arrangements are common in Mexico. Therefore, efforts aimed at spreading risk awareness in adolescents and young adults and limiting social interactions for members of certain age groups in certain venues may be considered to stem the increase of Covid-19 incidence among the community in Mexico.

