











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Population-wide patterns of health and mortality in older adults (OA) reflect the summary of the impact of their beneficial and deleterious exposures throughout the life course, and interactions with biological phenomena and social determinants of health (SDH).1The life course model helps to understand why the exposures to social and biological determinants of health during earlier periods of life may manifest some of their effects in later stages of life, and even beyond to future generations.2 For instance, the level of education of the mother may impact the health of her descendants through mechanisms such as the accumulation of risks, chains of risks or transfer of assets.1,2,3
The publication of the SDH conceptual framework by the World Health Organization (WHO),4spurred interest in understanding how socioeconomic status (SES) or social cohesion (SC) impact health. The SDH (through SES and SC, for example) are recognized as “fundamental causes” of mortality patterns despite the fact that mechanisms involved have changed through history.5
Besides social determinants of health, frailty, as a more proximal determinant of health in OA, is understood as a complex entity characterized by a diminished functional reserve, with pathogenic mechanisms including multi-level biological damage of the organism predisposing to outcomes such as disability and mortality.6Complexity in frailty arises not only from biological processes, but also because of the multiple pathways through which the social and ecological events impact biological variables, and result in the expression of health or illness.
Some studies have examined the effects of biologic susceptibility and social vulnerability together on the health of OA.7,8,9The importance of putting both dimensions together is that they exert their effects simultaneously in real life. The study of the relation between the biologic and SDH has yet to be developed, not just to advance science but also to provide knowledge useful to inform sound public policies in health and other sectors.
This study aimed to examine the longitudinal association between the social determinants of health and frailty status with all-cause mortality in a nationally representative sample of older Mexican adults. We also examined whether the mother’s education could modify the association between older adult’s education level and their mortality rate.
Materials and methods
Population and study design. The Study on Global AGEing and Adult Health (SAGE) is a longitudinal multi-country survey with nationally representative samples of adults in China, Ghana, India, Mexico, the Russian Federation and South Africa, meant to increase knowledge about the population-aging process in low and middle-income countries. SAGE has data from: wave 1 in 2009, wave 2 in 2014, and wave 3 was collected in 2018. Details of the design and recruitment were published elsewhere.10
Data were collected using household and individual questionnaires. All individuals aged 50 years and over in selected households were invited to participate. Questionnaires included information about socio-demographics, health status (including anthropometric measurements and blood samples), and indicators of SDH, among others.10
The sampling procedure for SAGE-Mexico has been described elsewhere.11Briefly, SAGE-Mexico was implemented through a partnership between the National Institute of Public Health (Instituto Nacional de Salud Pública, INSP) and the WHO. For the present study, exposures of interest correspond to data from wave 1, collected between August and October of 2009, and mortality was registered according to the vital status of the older adult in wave 2, 2014. Older adults aged 60 and older were included in all the statistical analysis. Wave 1 collected information on 1 873 persons aged 60 and older. After excluding those with incomplete information for all of the variables used to define frailty status (n=25), the sample was 1 848. In wave 2, 320 (17.8%) OA lost to follow-up. There were not statistical differences in the exposure variables between the latter and the participants included in the follow-up. The final analytical sample was 1 519 respondents from whom information was available for all variables (figure 1).
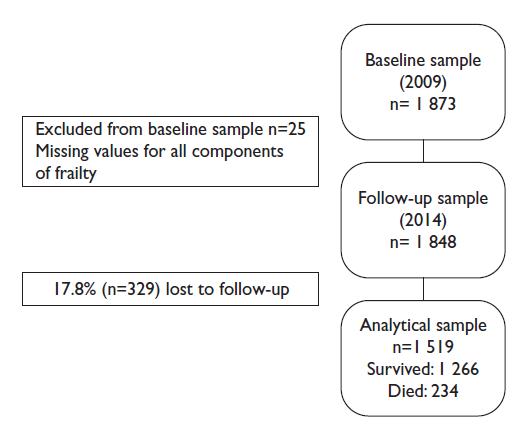
Figure 1 Analytical sample definition of respondents aged 60 years and older. SAGE México, 2009-2014
SAGE-México was approved by the Ethics Review Committee of the INSP. All respondents reviewed and signed a written informed consent form.
Outcome
All-cause mortality. Cause and date of death were obtained from interviews with relatives using a verbal autopsy questionnaire during wave 2. Mortality rate was assessed for four years and five months of follow-up.
Exposures
Social determinants of health (SDH)
Socioeconomic status (SES) and social cohesion (SC) are iconic of structural and intermediate level social determinants of health, respectively,4and were operationalized in a separate way as follows. According to the conceptual framework of the WHO Commission,4SES is explained by: A) education operationalized using milestones of less than primary, primary completed and secondary completed or more; B) active labor status if declared to have had worked for at least two days during the last seven days; and, C) wealth, a hierarchical ordered probit model was used to develop an index of household asset ownership of durable goods, dwelling characteristics, and access to services.12,13Measuring wealth is suitable for material circumstances in OA, rather than income, given the high probability of subjects being retired or lacking a regular income in older age. It also reflects the accumulation of assets over the life course. Higher values in the wealth index indicate better socioeconomic status than lower ones.
Social cohesion (SC) was measured by three components: A) frequency of interpersonal contacts, B) trust, and C) feelings of control over one´s life. For the first component of SC: frequency of inter-personal contacts, nine items were included regarding social activities in table I.
Table I Construction of the frequency of contacts variable. SAGE México, 2009-2014
| Question: In the last 12 months, how often have you… | ||
| 1. | …attended any public meeting in which there was discussion of local or school affairs? | |
| 2. | …met personally with someone you consider to be a community leader? | |
| 3. | …attended any group, club, society, union or organizational meeting? | |
| 4. | …worked with other people in your neighbourhood to fix or improve something? | |
| 5. | … had friends over to your home? | |
| 6. | … been in the home of someone who lives in a different neighbourhood than you do or had them in your home? | |
| 7. | … socialized with co-workers outside of work? | |
| 8. | … attended religious services (not including weddings and funerals)? | |
| 9. | … gotten out of the house/your dwelling to attend social meetings, activities, programs or events or to visit friends or relatives? | |
Item responses were structured on a five-point Likert scale (never=1, once or twice per year=2, once or twice per month=3, once or twice per week=4, daily=5). Each item was summed to get a global score which ranged between nine and 36. Internal consistency of the frequency of contacts score was evaluated, obtaining a Cronbach’s α=0.71. The second component of SC, trust, included one yes/no item “Do you have someone you can trust?”. The third component of SC, control over one’s life, was evaluated by the question, “How often have you felt that you were unable to control the important things in your life?”. Answers were: 1= “never,” 2= “almost never,” 3= “sometimes” and 4= “fairly and very often”.
Life course socioeconomic conditions were approached using the education of the mother, as a proxy of the socioeconomic conditions for early child development, given its relation with child mortality,14,15and was included as the dichotomous variable: mother completed primary or more education? (yes/no).
Frailty status
Frailty was defined according to the five components proposed in the phenotype of the Cardiovascular Health Study6at baseline, namely: 1) Slowness was determined if the respondent was in the highest quintile on the timed four meter walking test adjusting for height and sex. 2) Weakness, if in the lowest quintile of grip strength adjusted for sex and body mass index. 3) Low physical activity, if METS/week were in the lowest quintile, adjusting for sex. 4) Weight loss, if self-report of unintentional weight loss ≥ 5 kg in the last year.16,17 5) Exhaustion, if a positive answer to the question: “During the last 12 months, have you had a period lasting several days when you have been feeling your energy decreased or that you are tired all the time?”. Participants who met three or more criteria were classified as frail; those meeting one or two were classified as pre-frail; and none, as robust.
Covariates
Potential confounders were chosen to account for the effect of variables which have been associated with mortality in OA and thus might interfere in the studied association.18,19,20 From the covariates chosen, we used the ones available in the SAGE dataset: age (60-69 years old, 70-79 years old, and 80 and older); sex (female and male); marital status (married or cohabiting and widowed or separated or divorced or never married); place of residence (rural if population less than 2 500 and urban if population 2 500 or greater), and multimorbidity (presence or absence) defined as the simultaneous presence of two or more non-communicable diseases (NCDs) from the following list: diabetes, stroke, hypertension, angina, chronic obstructive pulmonary disease, depression, and cataracts.
Statistical analysis
In bivariate analysis, the following statistical procedures were used according to the characteristics of each variable: bivariate logistic regression analysis for categorical data and t-test for continuous data. Cumulative survival curves were constructed to display the associated cumulative probabilities of survival among the three levels of frailty.During the exploratory analysis a possible interaction effect was identified between the variables older adults’ education and mother’s education. Therefore, in the final model the interaction between these two variables was assessed.
A Cox proportional hazard model was used to estimate the SDH and frailty-related hazard ratios (HR) for mortality over the study period. The final model was evaluated in terms of collinearity, goodness of fit, and residuals, and included the verification of the proportional hazard assumption. In all the analyses, data were weighted using post-stratified individual probability weights based on the selection probability at each stage of selection. Statistical analyses were performed using STATA 15.1, 95% confidence intervals and p-values were reported. Differences were considered statistically significant ifpvalue < 0.05.
Results
In wave 1 (2009), mean age was 70.4 years (SD=7.7); 55.2% of participants were women, 61% were married or cohabiting, 44% reported multimorbidity, and 26% lived in a rural residence. Baseline frailty prevalence was 11.9%, prefrail 54.9%, and robust 33.2%. Frailty prevalence increased with age, being 8.9, 10.5 and 30.3% of adults aged 60-69, 70-79, and 80 or older, respectively. Also, frailty prevalence was higher among women (13.3%) than men (10.2%).
Overall mortality was 16.9% during the four years and five months study period, with a stepwise trend throughout levels of frailty: 8.5, 17.1, and 39.2% in robust, pre-frail and frail correspondingly, and the mean age of the older adults who died after four years and five months was 74.1 (SD=8.7). Regarding SDH, in comparison with those who survived, participants who died were less educated (p<0.01), more likely to have an inactive labor status (p<0.01), reported a lower frequency of inter-personal contacts (p<0.01), and lower levels of household wealth index (p=0.02) (table II).
Table II Characteristics of respondents by survival status.* SAGE Mexico, 2009-2014
| Survived % (n=1 266) | Died % (n=234) | p value‡ | ||||
| Exposures | ||||||
| Frailty | ||||||
| Nonfrail | 36.52 (462) | 16.79 (39) | ||||
| Prefrail | 54.75 (693) | 55.51 (130) | 0.02 | |||
| Frail | 8.73 (111) | 27.7 (65) | <0.01 | |||
| Socioeconomic status | ||||||
| Education | ||||||
| Less than primary | 65.49 (829) | 65.38 (153) | ||||
| Primary completed | 20.86 (264) | 14.91 (35) | <0.01 | |||
| Secondary or more | 13.65 (173) | 19.71 (46) | <0.01 | |||
| Active labor status | ||||||
| No | 77.18 (977) | 86.83 (203) | ||||
| Yes | 22.82 (289) | 13.17 (31) | <0.01 | |||
| Household wealth index (mean) | 0.007 (sd=0.39) | 0.002 (sd=0.39) | 0.02 | |||
| Social cohesion | ||||||
| Frequency of inter-personal contacts (means) | 15.17 (sd=4.82) | 13.83 (sd=4.23) | <0.01 | |||
| Trust (have someone to trust) | ||||||
| No | 9.06 (21) | 17.49 (221) | ||||
| Yes | 90.94 (213) | 82.51 (1 045) | 0.03 | |||
| Feelings of poor control over one’s life | ||||||
| Never | 38.58 (488) | 28.34 (66) | ||||
| Almost never | 33.33 (422) | 32.07 (75) | 0.47 | |||
| Sometimes | 24.23 (307) | 33.91 (79) | 0.18 | |||
| Fairly-very often | 3.86 (49) | 5.68 (73) | 0.17 | |||
| Life course determinants | ||||||
| Mother with less than primary education | ||||||
| No | 7.87 (100) | 27.32 (64) | ||||
| Yes | 92.13 (1 166) | 72.68 (170) | 0.02 | |||
| Covariates | ||||||
| Age | ||||||
| 60-69 | 52.10 (660) | 48.88 (114) | ||||
| 70-79 | 38.34 (485) | 30.16 (71) | 0.03 | |||
| 80 + | 9.57 (121) | 20.96 (49) | <0.01 | |||
| Female | ||||||
| No | 45.40 (575) | 41.90 (98) | ||||
| Yes | 54.60 (691) | 58.10 (136) | 0.68 | |||
| Married or cohabiting | ||||||
| No | 39.54 (501) | 34.07 (80) | ||||
| Yes | 60.46 (765) | 65.93 (154) | 0.53 | |||
| Rural residence | ||||||
| No | 72.81 (922) | 80.76 (189) | ||||
| Yes | 27.19 (344) | 19.24 (45) | 0.14 | |||
| Multimorbidity | ||||||
| No | 58.20 (737) | 42.84 (100) | ||||
| Yes | 41.80 (529) | 57.16 (134) | 0.08 | |||
*Data are mean (SD) or % (n)
‡Bivariate logistic regression analysis for categorical data and t-test for continuous variables
SAGE: Study on Global AGEing and Adult Health
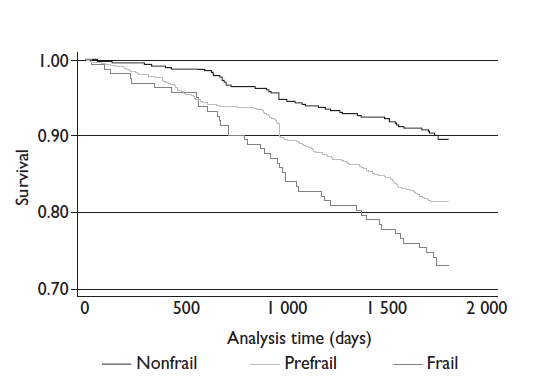
Figure 2 shows the unadjusted association between frailty status and cumulative survival probability in the study period. Frail or prefrail participants at baseline displayed an increased mortality risk compared with non-frails individuals at four years and five months.
SAGE México, 2009-2014
Figure 2 Kaplan-Meier survival curve over four years and five months follow-up by baseline frailty status of older adults. SAGE México, 2009-2014
Table III shows the adjusted association of SDH and frailty with four years and five months mortality using a Cox proportional hazard model.
Table III Cox proportional hazard model for four years and five months mortality in older adults. SAGE Mexico, 2009-2014
| Hazard Ratio | p-value | Confidence Interval (95%) | ||||
| Exposures | ||||||
| Frailty (reference: non-frail) | ||||||
| Prefrail | 1.73 | <0.01 | 1.45-2.06 | |||
| Frail | 2.83 | <0.01 | 2.27-3.53 | |||
| Socioeconomic status | ||||||
| Education (reference: less than primary) | ||||||
| Mother with primary completed | ||||||
| Primary completed | 0.21 | <0.01 | 0.14-0.33 | |||
| Secondary or more | 0.18 | <0.01 | 0.13-0.25 | |||
| Mother with less than primary | ||||||
| Primary completed | 1.07 | 0.54 | 0.87-1.30 | |||
| Secondary or more | 0.78 | 0.10 | 0.57-1.05 | |||
| Active labor status (reference: no) | 0.68 | 0.03 | 0.56-0.83 | |||
| Household wealth index | 1.34 | 0.40 | 0.67-2.66 | |||
| Social cohesion | ||||||
| Frequency of inter-personal contacts | 0.96 | 0.01 | 0.95-0.97 | |||
| Trust (reference: have someone to trust) | 1.59 | 0.03 | 1.27-1.98 | |||
| Feelings of poor control over one’s life (reference: never) | ||||||
| Almost never | 1.02 | 0.82 | 0.87-1.20 | |||
| Sometimes | 1.33 | 0.01 | 1.12-1.58 | |||
| Fairly-very often | 1.88 | <0.01 | 1.39-2.53 | |||
| Covariates | ||||||
| Age (reference: 60-69 years) | ||||||
| 70-79 | 0.76 | 0.36 | 0.42-1.37 | |||
| 80 + | 1.65 | 0.14 | 0.85-3.21 | |||
| Female | 0.85 | 0.47 | 0.55-1.31 | |||
| Married or cohabiting (reference: no) | 1.21 | 0.51 | 0.70-2.07 | |||
| Rural residence | 0.81 | 0.42 | 0.49-1.34 | |||
| Multimorbidity (reference: no) | 1.14 | 0.59 | 0.70-1.86 | |||
SAGE: Study on Global AGEing and Adult Health
Socioeconomic status
Significant reductions in mortality risk were found for several indicators of SES. First, interaction term between older adult’s education and mother’s education was significant (p for interaction <0.05). Results showed that having completed primary (HR=0.21; CI95%: 0.14-0.33) and completed secondary school or a higher level (HR=0.18; CI95%: 0.13-0.25) diminished the risk of dying compared to less than primary completed but only if the mother had a primary education completed; if the mother had less than primary, association between older adult’s education and mortality was not significant. Additionally, reporting an active labor status at the time of the baseline survey reduced the risk of mortality compared to an inactive labor status (HR=0.68; CI95%: 0.56-0.83) (table III).
Social cohesion
A reduction in mortality risk was observed for the frequency of inter-personal contacts (HR=0.96; CI95%: 0.95-0.97). Meanwhile, reporting a poor control over one’s life for categoriessometimes(HR=1.33; CI95%: 1.12-1.58) andfairly/very often(HR=1.88; CI95%: 1.39-2.53) increased the risk of dying compared to never having a lack of control over the important things in their life. Finally, not having someone to trust raised the risk of mortality (HR=1.59; CI95%: 1.27-1.98).
Discussion
This study investigated whether SDH and frailty status were associated with mortality in a nationally representative sample of older Mexican adults. The results showed that higher education, being occupationally active, having a higher frequency of inter-personal contacts, counting on someone to trust, and having a sense of better control over important decisions in life reduced the risk of dying, even after adjusting for potential confounders such as age, sex, and comorbidities. In the same vein, baseline frailty status increased the mortality risk after adjusting for potential confounders.
Higher education has been consistently associated with better health outcomes in older adults.21Education impacts mortality using three main life course pathways: 1) enhancing knowledge, skills, and resources which may help adults find a better job and eventually increasing access to healthcare, 2) improving psychosocial resources such as an increased sense of personal control, closer social relationships and participation related to better health, 3) health behaviors are more likely to be adopted by more educated people than by less educated people.22
Our findings in regard to the interaction between the education of the mother and that of the OA are consistent from the life course perspective, illustrating that good socioeconomic conditions during the early childhood development may provide the children with a higher initial level of intrinsic capacity and material assets which allows them to thrive throughout the life course, and eventually arrive to older age with a higher functional reserve, explaining their lower mortality risk.23,24
Active labor status had a significant protective effect for mortality risk in this study. This result is similar to what have been reported about the beneficial effects of having a paid job on the physical and mental health of the older adults.25Specifically, it is argued that work allows, in addition to having an income, the increase of social relations, as well as the maintenance and development of interpersonal and intellectual skills.25Although in our analyzes we could not distinguish between different types of employment, the protective effect of employment on mortality reported in this study is consistent with the studies of Martikainen and colleagues,26Lundin and colleagues,27and Schinka and colleagues.28While it is true that the mechanisms of this association have not yet been established, Schinka and colleagues28postulates that unemployment has an adverse effect on health in general, and particularly on death, which goes beyond the factors of vulnerability. In this sense, employment can be a proxy for the effect of several factors (measured and not measured), in such a way that the association observed in our work can be the result of indirect benefits for general health through the mental and physical health that comes from having a job.
Social interaction benefits health through psychosocial and psychobiological pathways.4,29 Cassel and Cobb have reviewed the evidence including experimental and non-experimental studies in humans and other animals examining the role of social support in different life stages and several health outcomes such as mortality, including low birth weight, complications of pregnancy, self-reported illness symptoms, blood pressure, chronic conditions, and alcoholism.30,31Findings suggest that social support acts on health directly supplying resolution to day-to-day needs or by buffering mechanisms using neuroendocrine pathways (cortisol, oxytocin and fibrinogen levels) with repercussions on immune and cardiovascular systems32According to our results, the beneficial effects of social interaction on health persist after controlling for frailty status and comorbidities, which to some extent serve as a proxy for the burden of biological insults. Health in aging populations should emphasize strategies to maintain or enhance social networks in older adults and consider creative policies regarding social networking in both urban and rural settings. While the number of virtual interactions grow and have been related to growing self-efficacy and empowerment,33both real and virtual modalities are to be promoted through the life course. Intergenerational clubs,24or gerontological nucleus34are two available models for strengthening social networks of OA in the community setting.
Studies on the health-related effects of a sense of control started in the context of psychosocial working conditions and later expanded to the private life.35,36In this study, the question used for measuring control asked the respondent to consider aspects of life she/he considered important not specific to working or domestic areas. Lachman and Weaver confirmed that sense of poor control was a moderator of the relationship between socioeconomic status and health assessed as self-rated health, the presence of acute symptoms and functional limitations. Participants with low SES but higher levels of perceived control showed health levels similar to those of higher SES.37
We are aware of the limitations of using separate variables to estimate the effect of two constructs such as SES and SC. We agree with the conceptual framework of the WHO commission4in terms of the characterization of structural and intermediate determinants to describe the pathway through which social determination of health impacts health and health inequity. Structural determinants generate forces of social stratification thereby affecting health. Capturing the dynamics of such a process is beyond the scope of this paper, but is an attempt to account for the three main theories about the relation of socioeconomic status and health considered by Grundy and Holt: materialist, behavioural and psychosocial.38We decided to keep all three variables: education, work status and wealth.
Some additional limitations must be mentioned: cautionary conclusions should be drawn about the associations between complex constructs (SES and SC) and mortality in consideration of the topics discussed in the previous paragraph. Integrating multi-level modeling of mortality and other health events will help future studies to understand the aggregation levels individual, social and environmental. These limitations could be tackled by gathering and including aggregate data for capturing the structural and intermediate determinants in regions and communities of the country. The use of an allostatic load39measurement might serve to provide further analytic elements for the sociobiological interaction. Also, the type of death (sudden versus prolonged illness) could be explored in additional analyses with data from the verbal autopsies to find out if it can be taken as an expression of the mechanisms of biosocial interaction in the failure of body systems.
These results have implications for the public health system in low- and middle-income countries with aging and level of development profiles like those of Mexico such as increasing the capacity of communities and health services to identify frail older adults, especially in disenfranchised populations and provide a risk-stratified health care, comprising not only risks related to frailty status but also SDH. Besides, inter-sectorial efforts between the educational, labor, social and health sectors should be fostered to effectively tackle upstream determinants, in harmony with health system interventions. For example, if OA do not feel safe while walking on the streets or using public transportation, their frequency of contacts is likely to be low. Besides, given that long term care is based on family settings in low- and middle-income countries,40strategies to increase control and trust in such settings should be researched and promoted.
Conclusions
These results have shown that a higher level of education, an active labor status, more frequent contact interactions, having someone to trust, and having a sense of better control over one’s life were associated with a reduction in the mortality risk in a nationally-representative sample of OA, even after controlling for biological conditions such as frailty, and comorbidities. Therefore, it is relevant and significant when biological and social perspectives are integrated in the public policies aimed at improving health levels of the aging population. For instance, in the organization of the health system to provide risk-stratified health prevention and care.

