











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
In Mexico, the first initiative on sexual education in schools dates from more than 80 years ago. Since then (1934),1several actions, reforms and evaluations have been the subject of constant debate.2Explicit acknowledgment of adolescent sexuality and the right to practice it has required an arduous effort of advocacy, which has not always achieved uniform results.1,3,4
In the country, one of the most tangible and operative means by which advances in sexual education have been implemented involves including mandatory curricular content; however, free official textbooks and standardized content are provided only in primary school.5In secondary and high school years, authorities of each state control this curriculum.6,7 It is diversified through the inclusion of courses and textbooks from various publishers, and as a result, teachings on sexuality may follow different approaches and the clarity of the information and concept integration could vary.7
We know that even when adolescents have insufficient knowledge to adopt healthy patterns of behavior, information is a significant starting point for guidance when they have acquired the appropriate competencies. A lack of precise knowledge or acquiring inaccurate information can undermine efforts to encourage desirable behaviors for prevention,8,9 in this case, of undesired pregnancies. Here it is also important to emphasize that, in addition to books, adults have participated in transmitting specific content that is shaping adolescent sexuality. However, adults are constantly misinformed, uninterested or reluctant to discuss significant issues surrounding sexual and reproductive health (SRH),4,10,11which in turn influences the information adolescents receive and how and when it is offered.12,13
Although Mexican Sexual Education Program has been derived from a biomedical approach,5,14 it is common to find that adolescents have an imprecise and vague grasp of even basic concepts of how their bodies function. Nationwide, surveys which have gathered fundamental information on adolescents’ knowledge of the subject provide clues on the level of understanding that segments of the population have regarding the functions of the human body and reproductive system. A look at the data shows that their knowledge on fundamental issues is weak; for example, in 2003, it was found that only 49% of Mexican women ages 15 to 19 have an accurate knowledge of when a woman is most likely to conceive if she engages in sexual intercourse,15,16 and this knowledge decreased to 27.2% in 2014.16Among the student population, it was reported that only around 10% correctly identified the time of highest fertility in the menstrual cycle17 and 12% of males did not know that a woman can get pregnant from the first time she has sexual relations.18Another study in eleven secondary schools of two states of central Mexico shows that 90% of males have an incorrect answer about the time of highest fertility in the menstrual cycle and 45% did not know that women could conceive since the sexual debut.19It bears mention that a 2015 nationwide survey asked adolescents if, during their elementary, junior high, or high school years, anyone at school had spoken to them about the reproductive system, in particular where the eggs and sperm are formed and in general how pregnancy occurs.20A majority of the subjects answered affirmatively; however, the survey does not allow us to recognize the level of understanding and clarity adolescents possess on these subjects.
In summary, results like previous mentioned serve to confirm that adolescents have some knowledge of the physiological processes involved in reproduction, but these are not always thoroughly interrelated. This level of partial or incorrect understanding is cause for concern given that, for decades, such information has been part of the curriculum of primary education, with direct implications for the development of students’ skills and alternatives for prevention of unwanted pregnancy.21,22
Based on this incomplete or confused idea that adolescents have, and seeking to contribute to this discussion from the essential factors which may affect to Mexico’s high rate of adolescent pregnancy (85 per 1 000 women of reproductive age),23our analysis seeks to measure the impact of a community intervention in sex education in a rural context on adolescents’ knowledge regarding the phase of the menstrual cycle with more likelihood of pregnancy, identifying, in turn, the factors associated with this subject.
Our interest in focusing this analysis on that relatively fundamental and simple question was to see if providing adolescents with specific, objective and precise information enhances their knowledge of the biological functioning of their own and their partners’ bodies and, in turn, improves their understanding of the egg-sperm fusion and the recognition of higher and lower risk of fertilization as an elementary, but not exclusive, foundation for prevention of unwanted pregnancy.
Materials and methods
Population and sample
This study used a quasi-experimental design. We selected the state of Morelos where the proportion of pregnancy adolescent (2011) was higher than the national average (58 vs. 52%).24There, we selected a municipality with a low Human Development Index.25Then, we selected two communities with a high or very high marginalization level,26both geographically accessible and far enough apart to avoid spillovers effects.
The survey was designed to estimate the difference of proportions in key concepts of reproductive health knowledge. We assumed that at least 84% of rural adolescents would know the number of times a condom can be used, based on the last National Health Survey.24We undertake a proportions difference of 5% such as the ability of IG and CG to know this information. The sample size was 578 (289 per group), this would be adequate to detect differences of proportions with 90% power and a significance level of 0.05.
We conducted a household census to identify all the adolescents in each community. We performed the baseline survey, the intervention and the followed-up between May 2016 and March 2017 (figure 1).21,27For the data collection, first, we applied in secondary and high schools of both communities. Later, based on census list we went to adolescent’s homes to complete the sample. We excluded from the study those who have a disability, refused to participate, temporarily absent or moved to another community.21,27
Variables
Dependent variable (DV):Adolescents’ knowledge of the phase of the menstrual cycle with highest likelihood of pregnancy. Evaluated with the question: At what time in the menstrual cycle is a woman most likely to conceive? (right=0/wrong=1).
Independent variables (IV):The following sociodemographic factors were included: age (11-15=0/16-20=1), sex (male=0/female=1), marital status (unmarried=1/formerly or presently married=0), household composition (nuclear family=1/extended family=2/other=3), socioeconomic level constructed from a predefined index28(level A=1-low-/level B=2 -middle-/level C=3-high), occupation (attends school only=1/ attends school and works=2/no school=3), sexual debut (no=0/yes=1), identifies as religious (no=0/yes=1), lives in the locality (no=0/yes=1), and survey application site (home=1/school=2).
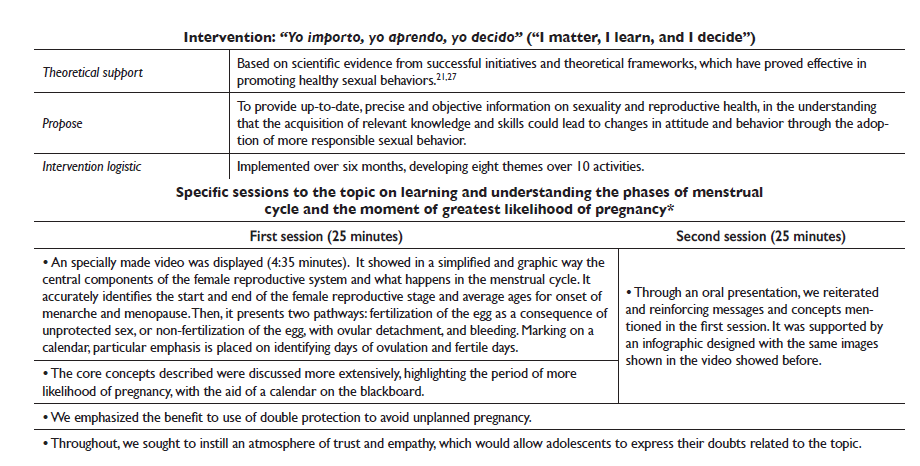
Considering that the theory shows that pregnancy is linked to multiple factors, including knowledge, attitudes, expectations and self-efficacy in sexual and reproductive health,21,27 six additive indices were constructed: a) considers himself/herself unlikely to marry and have children before age 20; b) knows his/her right to receive education and information on SRH; c) his/her perspective of equality in gender roles; d) he/she knows the correct use of the condom; e) he/she identifies as self-efficacy in use of the condom; and f) he/she knows the adequate way of taking the emergency contraceptive pill (ECP) and birth control pills (BCP) (figure 2). The cutoff point for each index was the mean plus a standard deviation (no=0/yes=1).
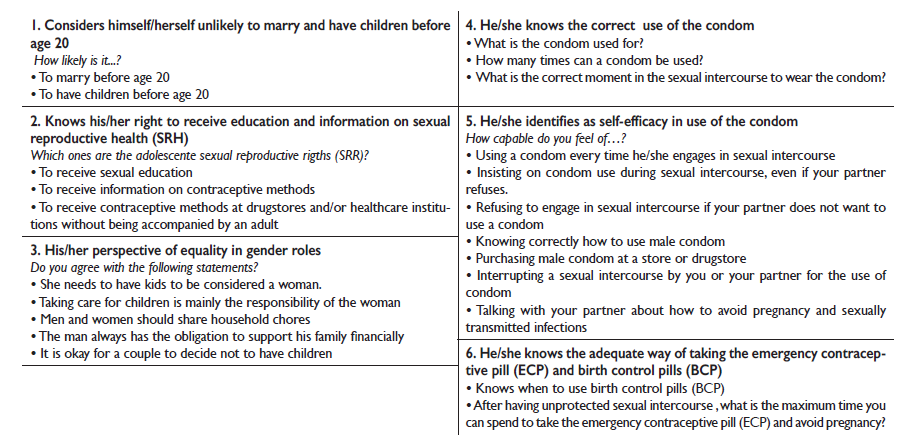
Source: Own elaboration from impact evaluation data “Yo importo, yo aprendo, yo decido” (2016-2017).
Figure 2 Additive indices description. Intervention in adolescents from rural context in Morelos, México, 2016-2017
Exposure level to the intervention: Based on this attendance count, an additive index was constructed that measures the levels of exposure to the intervention. This considers the exposition to the main and reinforcement activities: none (no activity), low (0-3 main activities plus 0-1 reinforcement activities; range 1-3); medium (1-5 main activities plus 1-5 reinforcement ones; range 4-8); and high (4-5 main activities plus 4-5 of reinforcement; range 9-10).
Analysis
All the variables were described by percentages. Chi-squared tests were performed to compare baseline characteristics between groups. Also, Chi-squared test were performed to compare sociodemographic characteristics and indices based on groups (IG and CG) and measurements (baseline and follow-up). To estimate the impact attribution to the intervention on knowledge of the phase of the menstrual cycle with more likelihood of pregnancy and to identify the factors associated with such knowledge, difference-in-differences29analyses with fixed effects models were performed (between stages and groups). Two models were constructed: for global effects and for exposure level (adjusted by sociodemographic variables). We verified that the model complied with the statistical assumptions and diagnosed the goodness of fit and multicollinearity. Effects were considered significant whenp<0.05 and 95%CI. All the analyses were performed using Stata V.12.0.
Results
We analyze the information of 747 adolescents who respond both questionnaires pre and posttest (397 IG and 350 CG) with 79% IG retention and 73% CG.
There were significant baseline differences between adolescents in the IG versus the CG, in relation to age, socioeconomic level, occupation, religiosity, and survey application site (table I).
Table I Baseline sociodemographic adolescent characteristics. Morelos, México, 2016-2017
| Variables | Total (n=747) % | Intervention group (n=397) % | Control group (n=350) % | p value* | ||||
| Age (mean) | 15.3 | 15.5 | 15.1 | <0.001 | ||||
| Sex | ||||||||
| Male | 48.2 | 47.6 | 48.9 | |||||
| Female | 51.8 | 52.4 | 51.1 | 0.733 | ||||
| Marital status | ||||||||
| Single | 90.0 | 89.2 | 90.8 | |||||
| Once or currently married | 10.1 | 10.8 | 9.2 | 0.451 | ||||
| Household composition | ||||||||
| Nuclear family | 57.3 | 55.9 | 58.9 | |||||
| Extended family | 41.9 | 43.3 | 40.3 | |||||
| Other | 0.8 | 0.8 | 0.9 | 0.700 | ||||
| Socioeconomic level | ||||||||
| Level A | 13.4 | 16.1 | 10.3 | |||||
| Level B | 69.1 | 70.0 | 68.0 | |||||
| Level C | 17.5 | 13.9 | 21.7 | 0.003 | ||||
| Occupation | ||||||||
| Attends school only | 77.2 | 82.5 | 72.5 | |||||
| Attends school and works | 14.1 | 10.9 | 16.9 | |||||
| No school | 8.7 | 6.6 | 10.6 | 0.005 | ||||
| Sexual debut | ||||||||
| Yes | 16.6 | 15.9 | 17.5 | 0.568 | ||||
| Religiosity | ||||||||
| Yes | 53.2 | 58.4 | 47.1 | 0.002 | ||||
| Lives in the locality | ||||||||
| Yes | 72.0 | 71.3 | 72.9 | 0.633 | ||||
| Survey application site | ||||||||
| Home | 49.5 | 53.2 | 45.4 | |||||
| School | 50.5 | 46.8 | 54.6 | 0.035 | ||||
* p values were calculated using Chi-square
Source: Own estimates from impact evaluation data “Yo importo, yo aprendo, yo decido” (2016-2017).
Differences between groups in relation to sexual and reproductive health indexes
About knowledge of phase of the menstrual cycle with more likelihood of pregnancy, we found that on the baseline both groups started similarly, but on follow-up, there were significant differences between them. On the CG had a higher percentage of adolescents who reported lacking such knowledge (83.7 vs. 57.2%,p<0.001) (table II).
Table II Adolescents’ knowledge of the phase of the menstrual cycle with highest risk of pregnancy and indices constructed about sexual and reproductive health at baseline and follow-up by intervention and control groups. Morelos, México, 2016-2017
| Baseline | Follow-up | |||||||||||||||||
| Total (n=747) | Intervention group (n=397) % | Control group (n=350) % | p-value* | Total (n=747) | Intervention group (n=397) % | Control group (n=350) % | p-value* | |||||||||||
| Knowledge of the phase of the menstrual cycle with more likelihood of pregnancy | ||||||||||||||||||
| No | 82.1 | 81.1 | 83.1 | 0.47 | 69.6 | 57.2 | 83.7 | <0.001 | ||||||||||
| Yes | 17.9 | 18.9 | 16.9 | 30.4 | 42.8 | 16.3 | ||||||||||||
| Indices‡ | ||||||||||||||||||
| Considers himself/herself unlikely to marry and have children before age 20 | ||||||||||||||||||
| No | 26.2 | 29.5 | 22.6 | 0.032 | 22.4 | 25.2 | 19.1 | 0.048 | ||||||||||
| Yes | 73.8 | 70.5 | 77.4 | 77.6 | 74.8 | 80.9 | ||||||||||||
| Knows his/her right to receive education and information on SRH | ||||||||||||||||||
| No | 24.2 | 27.2 | 20.9 | 0.043 | 17.4 | 21.7 | 12.6 | 0.001 | ||||||||||
| Yes | 75.8 | 72.8 | 79.1 | 82.6 | 78.3 | 87.4 | ||||||||||||
| His/her perspective of equality in gender roles | ||||||||||||||||||
| No | 20.6 | 27.0 | 13.4 | <0.001 | 13.9 | 18.6 | 8.6 | <0.001 | ||||||||||
| Yes | 79.4 | 73.1 | 86.6 | 86.1 | 81.4 | 91.4 | ||||||||||||
| He/she knows the correct use of the condom§ | ||||||||||||||||||
| No | 63.6 | 69.4 | 57.1 | 0.001 | 47.9 | 47.0 | 48.8 | 0.628 | ||||||||||
| Yes | 79.4 | 73.1 | 86.6 | 86.1 | 81.4 | 91.4 | ||||||||||||
| He/she identifies as self-efficacy in use of the condom | ||||||||||||||||||
| No | 39.5 | 43.8 | 34.6 | 0.010 | 29.5 | 32.8 | 25.7 | 0.035 | ||||||||||
| Yes | 60.5 | 56.2 | 65.4 | 70.6 | 67.3 | 74.3 | ||||||||||||
| He/she knows the adequate way of taking the ECP and BCP§ | ||||||||||||||||||
| No | 87.6 | 86.4 | 88.9 | 0.302 | 73.1 | 64.0 | 83.4 | <0.001 | ||||||||||
| Yes | 12.4 | 13.6 | 11.1 | 26.9 | 36.0 | 16.6 | ||||||||||||
SRH: sexual and reproductive health; ECP: emergency contraceptive pill; BCP: birth control pills
*p values were calculated using Chi-square
‡For more detail see figure 2.
§Percentage calculated from baseline data (n): Total=725, baseline: intervention group=382 and control group=343 / follow-up: Total=733, intervention=389 and control=344.
Source: Own estimates from impact evaluation data “Yo importo, yo aprendo, yo decido” (2016-2017).
Significant differences were found between groups in subjects who considered themselves unlikely to marry and have children before age 20, in both baseline (29.5 vs. 22.6%,p=0.032) and follow-up (25.2 vs. 19.1%,p=0.048) measurements: in both, the percentages were higher in the IG compared with the CG (table II).
Similarly, differences were found in knowledge of the right to receive education and information on SRH, between the IG and CG, and in both measurements, baseline (72.8 vs. 79.1%,p=0.043) and follow-up (78.3 vs. 87.4%, p=0.001); the percentage of adolescents who lacked knowledge of this right was higher in the CG (table II).
About the percentage of adolescents who lack a perspective of equality in gender roles, we found difference between the IG and CG was significant in baseline (27.0 vs. 13.4%,p<0.001) and follow-up (18.6 vs. 8.6%,p<0.001) figures; in both, the percentage of adolescents who lacked an equitable vision of gender was higher in the IG (table II).
Also, significant differences were found between groups on lack of perception of self-efficacy in use of the condom, which was higher among adolescents in the IG compared with the CG, in both baseline (43.8 vs. 34.6%,p=0.010) and follow-up (32.8 vs. 25.7%,p=0.035) measurements (table II).
As regards knowledge of proper use of the condom, significant differences between groups were found only in the baseline measurement, where the percentage of adolescents lacking such knowledge was higher in the IG than the CG (69.4 vs. 57.1%,p<0.001) (table II).
Finally, regarding knowledge of adequate use of the ECP and BCP, significant differences between groups were found only in follow-up, where the CG had a higher percentage of adolescents who reported lacking such knowledge (64.0 vs. 83.4%,p<0.001) (table II).
Interventions effects related to knowledge of the phase of the menstrual cycle with more likelihood of pregnancy
The intervention had a significant effect on knowledge of the phase of the menstrual cycle with more likelihood of pregnancy, reducing 22.1% the percentage of incorrect answers in adolescents who took part in the intervention vs. those who did not (p<0.001). It is noteworthy that the effects of the intervention were different depending on level of exposure; among adolescents with high exposure it was 35.1% (p<0.001) and in those with medium exposure, the average drop in lack of knowledge was 24% (p<0.001) compared with adolescents who were not exposed (table III).
Table III Differences in difference analysis for factors associated with knowledge of the phase of the menstrual cycle with highest risk of pregnancy, effects by global amd exposure level*. Morelos, México 2016-2017
| Exposure levellevel‡ | ||||||||||||||||
| Change % | p-value | Change % | p-value | Change % | p-value | Change % | p-value | |||||||||
| Dependent variable | ||||||||||||||||
| Knowledge of the phase of the menstrual cycle with more likelihood of pregnancy | -22.1§ | <0.001 | -35.1 | <0.001 | -24.0 | <0.001 | 3.33 | 0.526 | ||||||||
| Indices | ||||||||||||||||
| Considers himself/herself unlikely to marry and have children before age 201# | -30.5 | <0.001 | -43.6 | <0.001 | -32.5 | <0.001 | -5.2 | 0.380 | ||||||||
| Knows his/her right to receive education and information on SRH# | -32.2 | <0.001 | -44.9 | <0.001 | -33.8 | <0.001 | -6.5 | 0.258 | ||||||||
| His/her perspective of equality in gender roles# | -28.9 | <0.001 | -42.1 | <0.001 | 31.0 | <0.001 | -3.7 | 0.516 | ||||||||
| He/she knows the correct use of the condom# | -27.0 | <0.001 | -39.6 | <0.001 | -28.5 | <0.001 | -1.2 | 0.834 | ||||||||
| He/she identifies as self-efficacy in use of the condom# | -27.8 | <0.001 | -40.9 | <0.001 | -29.8 | <0.001 | -2.5 | 0.668 | ||||||||
| He/she knows the adequate way of taking the ECP and BCP# | -41.1 | <0.001 | -51.7 | <0.001 | -41.5 | <0.001 | -14.2 | 0.020 | ||||||||
*Adjusted by age, socioeconomic level, occupation, religiosity, and survey application site.
‡The reference category is “No-exposure”.
§Compared with the control group
#The reference category is “No”.
SRH: sexual and reproductive health; ECP: emergency contraceptive pill; BCP: birth control pills
Source: Own estimates from impact evaluation data “Yo importo, yo aprendo, yo decido” (2016-2017).
The average significant effect of the intervention on reduction of lack of knowledge of the phase of the menstrual cycle with more likelihood of pregnancy was different depending on the relationship shown with each of the indices. Thus, at global level we found that this lack of knowledge was 30.5% lower among adolescents who took part in the intervention and considered themselves unlikely to marry and have children before age 20 compared with adolescents who considered those events likely (p<0.001). By levels of exposure, the reduction was significant at the high and medium levels, 43.6 (p<0.001) and 32.5% (p<0.001), respectively (table III).
Among adolescents who took part in the intervention and knew their right to receive education and information on SRH, we observed at global level a significant reduction in lack of knowledge of the phase of the menstrual cycle with more likelihood of pregnancy of 32.2% (p<0.001). By exposure level, the reduction was significant at the high and medium levels, 44.9 (p<0.001) and 33.8% (p<0.001), respectively (table III).
Related to adolescents exposed to the intervention who had a perspective of equality on gender roles, we found at global level a significant average reduction of 28.9% in dependent variable compared with adolescents who lacked such perspective (p<0.001). The reduction was significant at the high and medium levels of exposure to the intervention, 42.1 (p<0.001) and 31% (p<0.001), respectively (table III).
Also, in the IG, adolescents who knew proper use of the condom showed a reduction in lack of knowledge of the phase of the menstrual cycle with more likelihood of pregnancy of 27% compared with adolescents who did not know proper use of that method (p<0.001). Differentiating by level of exposure to the intervention, the reduction was significant at the high and medium levels of exposure, 39.6% (p<0.001) and 28.5% (p<0.001), respectively (table III).
On the other hand, in the IG, the reduction in dependent variable was 27.8% among adolescents who identified as self-efficacy in use of the condom compared with those who did not (p<0.001). This reduction was significant at different levels of exposure to the intervention, 40.9% (p<0.001) for high exposure and 29.8% (p<0.001) for medium exposure (table III).
Finally, the intervention had a significant impact in reducing lack of knowledge of the phase of the menstrual cycle with more likelihood of pregnancy by 41.1% in adolescents who had correct knowledge of the ECP and BCP compared with adolescents who knowledge (p<0.001). This reduction was significant at the high 51.7% (p<0.001), medium 41.5% (p<0.001), and low 14.2% (p=0.020) levels of exposure to the intervention (table III).
Discussion
This study shows the effects of an intervention with adolescents in rural communities, incorporating knowledge of fundamental biological factors related to sexuality and reproduction among others. The purpose of the intervention was to enable adolescents to identify preventive elements, which help them avoid an unwanted/unplanned pregnancy, by recognizing the menstrual cycle and the moment of greatest likelihood of pregnancy. Knowing the body functions in reproduction could improve a better understanding of healthy sexual behavior. We believe that taking this knowledge for granted might be one of the reasons why teenagers are not acting more accurately to protect themselves and to avoid unwanted pregnancies.
This analysis considered the initial differences between the IG and CG, finding a positive impact regarding reduction of the lack of knowledge of the phase of the menstrual cycle with more likelihood of pregnancy, and its association with knowledge of birth control methods, self-efficacy, gender, and rights. The findings obtained in this study show that adolescents who achieved more right answers regarding the factors evaluated, also gave the correct answer to our question of interest. The inclusion and integration of SRH30 content as part of the community intervention was a key tool in achieving these results.
In addition, to conduct a more specific study of the achievements made, in this analysis, we distinguish the effects of exposure at four levels. Our findings confirm that high exposure to the intervention significantly improved adolescents’ knowledge of the menstrual cycle and its association with other vital issues for prevention of pregnancy. In other words, subjects who received greater contents through the intervention had an opportunity to internalize a systemic understanding of the topic of interest.
It is noteworthy that although in Mexico sex education has focused primarily on biologiscist orientation5,6,31,32our results and prior studies show that adolescent population has a limited understanding of this basic subject.15,16,17,18,19While the progress made through the intervention is encouraging, it also suggests that linking the process involving the male and female reproductive system with the possibility of fertilization is complex and confusing for some adolescents.
The literature reports that when adolescents understand the functioning of the female and male reproductive system and incorporate other fundamental topics of comprehensive sex education, they more easily overcome the limitations on practicing healthy sexuality.30,33Some investigations report that exposure to this curriculum -where reproductive biology is part of it- may influence attitudes, beliefs, and behaviors,20as well as the development of skills for decision-making in sexual practice.34,35Further, it has been seen that at this age, empowerment (for example appropriation of the body as a sexual right), entails substantial benefits for adolescents’ development in several areas of their life.36,37
Our intervention “Yo importo, yo aprendo, yo decido” emphasized describing and assessing specific content in reproductive biology, including the likelihood of pregnancy as a dependent variable. Internationally, early motherhood has also been a matter of interest. Various strategies and actions have been directed toward addressing it; notwithstanding, interventions do not always provide details of their curriculum, and less still do they analyze the likelihood of pregnancy as a dependent variable, providing limited evidence with which to compare our results. A recent systematic review27reports that only some evaluations include the components of menstrual cycle. Our analysis emphasizes that making such content explicit represented a real contribution to adolescents’ learning, mainly in rural context.
The results derived from this study with adolescents show that using relatively simple, specific, and comprehensive strategies, it is possible to explain the reproductive process to them in an understandable manner, and at the same time support them in appropriating necessary information on the functioning of their own and their partners’ bodies. Sex education for adolescents requires the incorporation of key thematic content, innovative, and attractive methodologies and materials. To stimulate their attention and interest in learning, it is important to use schematic resources, suited to adolescents’ thought structures.
It bears note that, as mentioned in the methodology (figure 1), this article describes only one component of the intervention. Notwithstanding, replicating it to achieve positive results on the pregnancy knowledge would require jointly implementing other actions, such as strengthening self-efficacy, thinking about the future, sexual and reproductive rights, and gender equality. Addressing those issues will help adolescents to gain information in favor of their SRH.
It is relevant to emphasize the effect produced by one of the control variables included in the analysis; adolescents’ gender was associated with lack of knowledge of the time of the menstrual cycle with the highest probability of pregnancy, with a greater reduction in women (31.28%) than in men. This situation may be due to the scant interest males show in a biological process which does not occur in their bodies. Moreover, it is common to find that the information provided to both men and women on what happens in men and women’s bodies during fertilization is fragmented. This situation hinders visualization of the process of formation, fusion, and interrelationship of egg-sperm, and therefore prevents adolescents from anticipating the potential consequences of unprotected sex.38,39
As we have remarked, possible reasons behind the difficulty adolescents have learning about this reproductive process involves the poor understanding also found among adults in charge of transmitting such knowledge.12,40As long as parents and teachers do not understand it clearly, they will have a hard time explaining it in simple and explicit terms.
Regarding parents in semirural contexts, a recent study in Mexico reports that when asked at what phase of the menstrual cycle a woman has more likelihood of pregnancy, less than half (42%) claimed to know well, and nearly a third (28%) claimed to know little or nothing.10These findings are surprising since one might assume that mothers and fathers, at least based on their own reproductive experience, would have accurate idea on the subject. For teachers, no similar studies were found; however, when asked how well informed they feel to provide sex education, data often report that they have a lack of adequate training.5Observers have also identified pedagogical deficiencies in their teaching skills.5,7
In Mexico, not too long ago discussing menstruation was taboo, and while adolescents today tend to be more familiar with it and open to the subject,10 our results show that their knowledge of the menstrual cycle does not necessarily cover the component of the potential for reproduction. In part, that may be due to adults’ fear of adolescents engaging earlier in sexual relations as a consequence of them gaining a greater understanding of the subject.11,31In this intervention, we maintained a commitment to the recognition of sexual and reproductive rights and prevention of pregnancy at early ages.
The findings described above should be interpreted with some limitations. One is due to the significant differences found between the study groups, based on which we cannot assure that they are equivalent; nevertheless, the limitation is partial, since those differences were controlled in our analyses. Moreover, the impact seen on change of knowledge may be affected by external factors like the presence of other actions paralleling the intervention, particularly in the control group. Likewise, because this study focused only on rural areas, its impact can just be extrapolated to populations with similar characteristics.

