











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Despite being modifiable risk factors, overweight and obesity remain an international public health problem. The prevalence of obesity has more than doubled since 1980,1and by 2014, over 1.9 billion, or 39% of adults (those 18 years old and older) were overweight. Of these individuals, 600 million (13%) were obese.2If this trend continues, it is estimated that by 2025, the prevalence of global obesity will reach 18% in men and exceed 21% in women.3
In the LAC region, the figures vastly exceed global averages. For the same year (2014), it is estimated that about 58% of the population (about 360 million people) were overweight and that 23% (140 million) were obese.4 In addition, it is expected that more than 50% of men and 60% of women will be overweight or obese by 2030.5
Overweight and obesity increase the burden of non-communicable diseases (NCDs). In the LAC region, NCDs are among the major causes of death and generate large economic costs for the public health system. It is estimated that between 2006 and 2015, NCDs cost low- and middle-income countries around 84 billion US dollars,6 and the World Health Organization has claimed that the burden of NCDs will increase by 17% in the next ten years.7
Globalization, which is considered a process broader than a simple measure of trade openness, involves an integration of economic, technological, sociocultural, political, and biological factors8 that affect people’s diets and lifestyles.9 The following mechanisms could explain a link between globalization and dietary patterns: (1) international food trade; (2) foreign direct investment; (3) global advertising and promotion; (4) the restructuring of food retailing; (5) the emergence of agribusiness and transnational food corporations; (6) the development of global rules and institutions that govern the production, trade, distribution, and marketing of food; (7) urbanization; and (8) cultural changes.10 These factors partly explain the changes in dietary patterns and lifestyles that have led to a rapid rise in the rates of overweight and obesity in developing countries.11,12
Figure 1 presents four KOF globalization indices (total, economic, political and social) that are widely used in existing literature and for which positive trends can be observed for most LAC countries included in the analysis between 1995 and 2013.
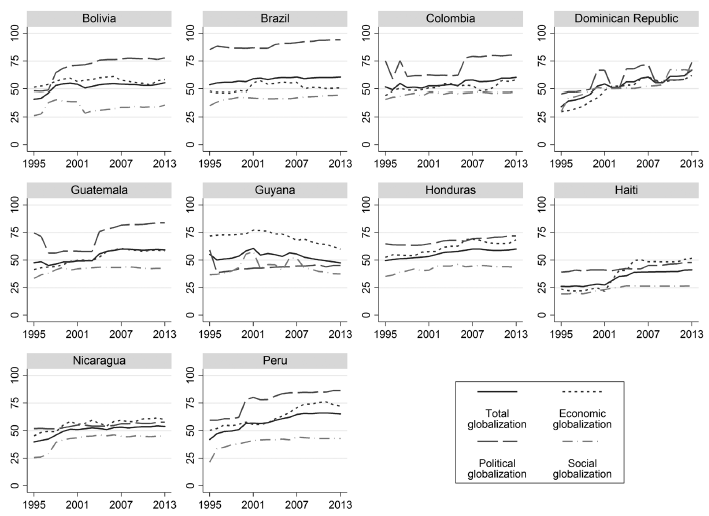
Figure 1 Trends of total, economic, political and social globalization in Latin America and the Caribbean countries. 1995-2013
Although the association between globalization and overweight/obesity has not been studied extensively, some work has been done.13,14However, most research has taken the form of ecological studies that analyze the link between some measure of globalization and a risk factor at the aggregate level. Furthermore, to our knowledge, no previous studies have focused specifically on LAC countries, despite their alarming figures related to overweight and obesity.
This paper analyzes the economic, political and social dimensions of globalization using the KOF indices, which are widely used in this type of analysis and are linked to the Demographic and Health Surveys (DHSs) for 10 LAC countries (Bolivia, Brazil, Colombia, Dominican Republic, Guatemala, Guyana, Honduras, Haiti, Nicaragua and Peru) between 1995 and 2013. This presents several advantages over other types of analysis. First, it allows the use of body mass index (BMI) at the individual-level, which guarantees an objective measure of overweight and obesity. It is also controlled by relevant confounding factors at an individual-level (e.g. age, education, marital status and number of children), which reduces the possibility of bias due to the omission of relevant factors15 and allows heterogeneity to be explored at the individual-level, analysis that could not be performed if only country-level data were used.
Materials and methods
Data source
Globalization
The phenomenon of globalization cannot to be measured unidimensionally because it is a product of multiple interaction factors. Consequently, this study uses the KOF index,16which has been used in several previous studies14,15and is composed of three dimensions (economic, political and social), which are further disaggregated into 23 subcomponents: the economic dimension comprises international trade (percentage of GDP), foreign direct investment (percentage of GDP), financial investments (percentage of GDP), foreign currency payments (percentage of GDP), hidden import barriers, average tariff rate, taxes on international trade (percentage of current revenues) and capital account restrictions. The political dimension incorporates the number of embassies per country, membership in international organizations, participation in United Nations Security Council missions and the number of international treaties signed. The social dimension includes outgoing telephone traffic (in minutes per 1000 inhabitants), transfers (percentage of GDP), international tourism (proportion of population), foreign population (percentage of total population), international charters (per capita), television users (per 1 000 inhabitants), Internet users (per 1 000 inhabitants), newspaper trade (percentage of GDP), book trade (percentage of GDP), number of Ikea stores (per capita) and number of McDonald’s restaurants (per capita).
Nutritional status
Individual data were extracted from DHSs for 10 LAC countries in the years 1995-2013. The country-year coverage was as follows: Bolivia (1998, 2003, 2008), Brazil (1996), Colombia (1995, 2000, 2005, 2010), Dominican Republic (1996, 2013), Guatemala (1995, 1999), Guyana (2009), Honduras (2005, 2012), Haiti (2000, 2005, 2012), Nicaragua (1998, 2001) and Peru (1996, 2000, 2004, 2009, 2010, 2011, 2012). The choice of countries and the periods of analysis were based on the availability of anthropometric data. The DHSs were designed to collect information on fertility, population health and nutrition in a target population of women aged 15-49.17 These surveys present representative and repeated sampling across a large group of countries with high response rates and provide objective information on the heights and weights of the persons interviewed using a standardized protocol.18 The DHS uses probabilistic sampling with a two-stage cluster stratified design, which has a given probability of selection.19 In the first stage, the sampling frames were developed using enumeration areas with a probability proportional to the size of the area. Subsequently, within each enumeration area, a household register was generated through field visits to select a fixed proportion of the households through systematic sampling. From each selected household, all women aged 15-49 with children aged 5 and under were invited to participate in the interviews and perform anthropometric measurements. Overall, the household response rates to the DHSs exceeded 90%.
Study population and sample size
The population included in this study was restricted to non-pregnant women aged 20-49 (n= 1 320 873) in 10 LAC countries for the period 1995-2013. Overall, values that did not present measurements of anthropometric data (height and weight, n = 328 817, or 24.89% of the sample) were eliminated. Of the observations that presented anthropometric data, observations that had extreme BMI values (less than 14 or greater than 50) defined through percentiles (<1st percentile or >99th percentile) were excluded. Finally, the values in which the covariables presented lost data were eliminated, resulting in an analytical sample of 848405 observations.
Outcome
BMI (kg/m2) was calculated by dividing weight (kg) by the squared height (m2) for the women of each country. For the subsequent statistical analysis, a dummy variable taking the value of 1 for individuals with a BMI ≥25 and 0 for everything else was used as an outcome variable. Previous works have used continuous BMIs as a dependent variable;13,20however, this approach does not capture the marginal changes between BMI and a particular covariate at the desired BMI value (e.g. when BMI ≥25).15
Independent variables
The main variables of interest were the aggregated KOF total globalization index and its subcomponents (economic, political and social). Other confounding factors at the individual-level were identified in similar studies and included to control regressions by relevant socioeconomic and demographic characteristics: (1) age (20-29, 30-39, 40-49), (2) type of residence (urban, rural), (3) level of education (no education, primary education, secondary education, higher education), (4) number of children, (5) marital status (married, living together) and (6) occupational status.14,21 Finally, to control for characteristics at the country-level, the following variables used in previous studies were included:15 GDP (at constant prices, 2010) as a proxy measure of market size, the human development index and the index of economic freedom.
Analysis
The micro data from the DHSs were downloaded for each country and the selected years and combined into a single database. Subsequently, the KOF indices were downloaded into MS Excel, converted into an appropriate format and linked to the previous database to create a pooled cross section at the individual-level for the studied countries for 1995-2013. All statistical analyses were performed using Stata software, version 14.0.
Empirical approach
First, a fractional polynomial prediction was made to evaluate the association between overweight and obesity proportion and the different dimensions of globalization (figure 2). This model allows adjusting to nonlinear functions and is more flexible than other polynomial models.
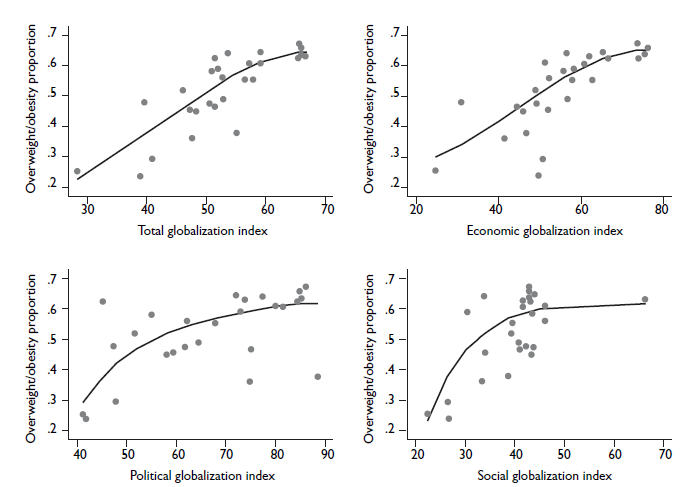
Figure 2 Fractional polynomial prediction between total, economic, political and social globalization and proportion of overweight/obesity in women 20-49 aged. Latin America and Caribbean countries, 1995-2013
To examine the association of interest, a logistic regression model that relates the KOF globalization index to the variable of interest was used. Subcomponents were then analyzed. The linear predictor of the logistic model was specified as:
where /
Results
Table I presents descriptive statistics. At the individual-level, it was observed that the population analyzed had a high prevalence of overweight and obesity (56%) and a low level of human capital. Only 9% of the total population had a higher education, and about 32% of subjects were unemployed. Indicators at the country level showed that, on average, Peru had the greatest value of total globalization (61) while Haiti had the lowest value (34). It was also observed that the Dominican Republic had the largest increase in total globalization (approximately 59%). At the disaggregated level, for the years and countries included in the analysis, the economic and political dimensions were above the world average (+0.02 and +0.50 standard deviations, respectively), while the social dimension was below the global average (-1.6 standard deviations).
Table I Individual- and country-level characteristics in Latin American and Caribbean countries. 1995-2013
| Variables | Values | |
| Individual-level* (n=848 405) | ||
| Overweight/obesity, % | 56.20 | |
| Age % | ||
| 20-29 | 21.14 | |
| 30-39 | 38.52 | |
| 40-49 | 40.34 | |
| Type of residence % | ||
| Urban | 50.37 | |
| Educational level % | ||
| No education | 15.22 | |
| Primary education | 50.02 | |
| Secondary education | 26.23 | |
| Higher education | 8.52 | |
| Marital status % | ||
| Married/living together | 84.74 | |
| Occupational status % | ||
| Employed | 57.79 | |
| Num. of children % | ||
| 0 | 3.55 | |
| 1-2 | 36.24 | |
| > 3 | 60.21 | |
| Country-level (k=27) | ||
| Globalization index ‡ | ||
| Total | 55.39±8.31 | |
| Economic | 58.19±11.49 | |
| Political | 71.50±12.88 | |
| Political | 71.50±12.88 | |
| Social | 40.93±6.77 | |
| GDP§ | 113 788.5±155 826.8 | |
| Human development index# | 0.65±0.07 | |
| Index of economic freedom& | 61.70±6.15 | |
*Data obtained from Demographic and Health Surveys22
‡Data obtained from KOF Swiss Economic Institute16
§Data obtained from World Development Indicators (World Bank)23
#Data obtained from World Development Indicators (World Bank). In millions at constant prices, 201023
&Data obtained from The Heritage Foundation24
Source: Prepared by the authors from the study data
Note: Estimates are percentages or mean ± standard deviation
figura 2 presents a fractional polynomial prediction between the proportion of the overweight and obese population for each country in each year and the indices of globalization in its different dimensions (total, economic, political and social). In all four cases, as the rates of globalization increased, the proportion of overweight and obesity increased. However, for political and social globalization, as the scores increased, this positive relationship weakened and took on a concave shape. In social globalization an outlier was identified and eliminated it to test if the curvature was maintained. It was observed that while the relationship weakens, it still maintains a concave shape. As for economic and total globalization, the slope appeared to be stronger and linear.
However, a visual examination cannot indicate whether this relationship alone can explain the association of globalization with overweight and obesity, or whether other confounding factors affected this association. In this sense, an interesting question refers to whether the association of the different dimensions of globalization remain when other mechanisms are considered. Column 2 of table II shows the logistic regressions between overweight and obese individuals and the total globalization index without adjusting for any covariates except for time fixed-effects. In this case, a positive association of total globalization with the odds of overweight and obesity was observed. To improve the accuracy of the estimation and control for relevant confounding factors, in column 3, the regressions are adjusted by characteristics at the individual-level, where a decrease in the magnitude of the association was observed. In column 4, it is controlled by relevant factors at the individual- and country-levels, and it was observed that the association was stable; in this case, a change of one standard deviation in the globalization index was associated with an increase of 38% in the odds of overweight and obesity. The control variables at the individual-level (table II, column 4) showed that all the coefficients at the education level indicated an increase in the odds of overweight and obesity with respect to their base category. However, there appeared to be a non-linear relationship in the form of an inverted U. Overweight and obese individuals were more likely to be living in urban areas, married and living together and employed. Conversely, there seemed to be a negative association between people with children and overweight and obesity. In relation to control variables at the country-level, the results suggest that an increase in GDP and economic freedom index were associated with reduced odds of obesity and being overweight, while an increase in the human development index could increase these odds.
Table II Association between the index of total globalization and overweight/obesity in women 20-49 aged. Latin America and Caribbean countries, 1995-2013
| Variables | Unadjusted* | Adjusted to individual-level‡ | Adjusted to individual- and country-level§ | |||||||||
| OR# [CI&] | P-value | OR [CI] | P-value | OR [CI] | P-value | |||||||
| z(total globalization) | 1.43 [1.40-1.46] | < 0.01 | 1.37 [1.34-1.39] | < 0.01 | 1.38 [1.34-1.43] | < 0.01 | ||||||
| Age | ||||||||||||
| 20-29 | Reference | Reference | Reference | |||||||||
| 30-39 | 1.87 [1.82 – 1.91] | < 0.01 | 1.85 [1.81 – 1.90] | < 0.01 | ||||||||
| 40-49 | 2.43 [2.37 – 2.50] | < 0.01 | 2.40 [2.34 – 2.47] | < 0.01 | ||||||||
| Educational level | ||||||||||||
| No education | Reference | Reference | Reference | |||||||||
| Primary education | 1.47 [1.42 – 1.52] | < 0.01 | 1.43 [1.38 – 1.49] | < 0.01 | ||||||||
| Secondary education | 1.62 [1.55 – 1.68] | < 0.01 | 1.57 [1.51 – 1.64] | < 0.01 | ||||||||
| Higher education | 1.33 [1.27 – 1.39] | < 0.01 | 1.28 [1.22 – 1.35] | < 0.01 | ||||||||
| Type of residence | ||||||||||||
| Rural | Reference | Reference | Reference | |||||||||
| Urban | 1.81 [1.76 – 1.86] | < 0.01 | 1.83 [1.78 – 1.88] | < 0.01 | ||||||||
| Marital status | ||||||||||||
| Single | Reference | Reference | Reference | |||||||||
| Married/living together | 1.33 [1.30 – 1.37] | < 0.01 | 1.35 [1.31 – 1.38] | < 0.01 | ||||||||
| Occupational status | ||||||||||||
| No employed | Reference | Reference | Reference | |||||||||
| Employed | 1.01 [0.99 – 1.03] | < 0.01 | 1.02 [1.00 - 1.04] | < 0.01 | ||||||||
| Num. of children | ||||||||||||
| 0 | Reference | Reference | Reference | |||||||||
| 1-2 | 0.83 [0.78 – 0.87] | < 0.01 | 0.83 [0.79 – 0.87] | < 0.01 | ||||||||
| > 3 | 0.79 [0.75 – 0.84] | < 0.01 | 0.80 [0.76 – 0.84] | < 0.01 | ||||||||
| z(GDP) | 0.84 [0.83 – 0.86] | < 0.01 | ||||||||||
| z(human development index) | 1.47 [1.40 – 1.54] | < 0.01 | ||||||||||
| z(index of economic freedom) | 0.73 [0.60 – 0.74] | < 0.01 | ||||||||||
*No controls except time-fixed-effects
‡Controls at individual-level, and time-fixed-effects
§Controls at individual- and country-level, and time-fixed-effects
#Odds ratio
&95% confidence interval
After analyzing the impact of total globalization, it is convenient to explore the heterogeneity of this index, disaggregating the association of the different dimensions. table III presents an analysis of the individual regressions between overweight and obesity and the indices of economic globalization, political globalization, and social globalization. Subsequently, a joint regression was made, including the three globalization indices. Finally, four levels were defined through quartiles and divided into four dummy variables, which represent the countries with the lowest globalization scores (level 1) to those with highest globalization scores (level 4). These levels were used to compute individual and joint regressions on the four globalization indices, thus allowing evaluation of nonlinearities in the estimates and a more intuitive interpretation of the coefficients than with the regressions of the globalization scores transformed into their standardized values. Consequently, if the level 2 coefficient was positive, people living in a country located within this level were at greater probability of being overweight and obese compared to level 1. In turn, for all estimates, column 2 contains unadjusted regressions, column 3 adjusts regressions for confounding factors at the individual-level and column 4 incorporates controls at the country-level.
Table III Association between total, economic, political and social globalization and overweight/obesity in women 20-49 aged. Latin America and Caribbean countries, 1995-2013
| Variables | Unadjusted* | Adjusted to individual-level‡ | Adjusted to individual- and country-level§ | |||||||||
| OR# [CI&] | P-value | OR [CI] | P-value | OR [CI] | P-value | |||||||
| Individual regressions | ||||||||||||
| z (economic globalization) | 1.33 [1.30 – 1.36] | < 0.01 | 1.30 [1.27 – 1.32] | < 0.01 | 1.14 [1.11 – 1.17] | < 0.01 | ||||||
| z (political globalization) | 1.35 [1.32 – 1.37] | < 0.01 | 1.28 [1.26 – 1.30] | < 0.01 | 1.40 [1.35 – 1.45] | < 0.01 | ||||||
| z (social globalization) | 1.58 [1.54 – 1.61] | < 0.01 | 1.49 [1.46 – 1.53] | < 0.01 | 1.40 [1.36 – 1.45] | < 0.01 | ||||||
| Joint regression | ||||||||||||
| z (economic globalization) | 1.19 [1.16 – 1.22] | < 0.01 | 1.24 [1.21 – 1.27] | < 0.01 | 1.09 [1.05 – 1.13] | < 0.01 | ||||||
| z (political globalization) | 0.96 [0.93 – 0.98] | < 0.01 | 0.90 [0.87 – 0.92] | < 0.01 | 1.18 [1.12 – 1.24] | < 0.01 | ||||||
| z (social globalization) | 1.52 [1.48 – 1.56] | < 0.01 | 1.49 [1.45 – 1.52] | < 0.01 | 1.36 [1.31 – 1.42] | < 0.01 | ||||||
| Individual regressions (levels≠) | ||||||||||||
| Total globalization | ||||||||||||
| Level 1 | Reference | Reference | Reference | |||||||||
| Level 2 | 1.90 [1.80 – 2.01] | < 0.01 | 1.58 [1.50 – 1.66] | < 0.01 | 1.51 [1.39 – 1.65] | < 0.01 | ||||||
| Level 3 | 2.24 [2.11 – 2.37] | < 0.01 | 2.30 [2.17 – 2.43] | < 0.01 | 2.17 [2.02 – 2.33] | < 0.01 | ||||||
| Level 4 | 2.41 [2.26 – 2.57] | < 0.01 | 2.24 [2.10 – 2.38] | < 0.01 | 1.74 [1.59 – 1.90] | < 0.01 | ||||||
| Economic globalization | ||||||||||||
| Level 1 | Reference | Reference | Reference | |||||||||
| Level 2 | 1.78 [1.69 – 1.88] | < 0.01 | 1.60 [1.53 – 1.68] | < 0.01 | 1.04 [0.97 – 1.11] | < 0.01 | ||||||
| Level 3 | 1.98 [1.86 – 2.11] | < 0.01 | 2.33 [2.19 – 2.47] | < 0.01 | 1.74 [1.58 – 1.92] | < 0.01 | ||||||
| Level 4 | 1.74 [1.64 – 1.84] | < 0.01 | 1.67 [1.59 – 1.76] | < 0.01 | 0.98 [0.92 – 1.04] | < 0.01 | ||||||
| Political globalization | ||||||||||||
| Level 1 | Reference | Reference | Reference | |||||||||
| Level 2 | 1.39 [1.33 – 1.47] | < 0.01 | 1.60 [1.52 – 1.68] | < 0.01 | 1.86 [1.78 – 1.95] | < 0.01 | ||||||
| Level 3 | 2.01 [1.89 – 2.14] | < 0.01 | 1.66 [1.56 – 1.76] | < 0.01 | 1.16 [1.08 – 1.25] | < 0.01 | ||||||
| Level 4 | 1.79 [1.70 – 1.89] | < 0.01 | 1.56 [1.48 – 1.64] | < 0.01 | 1.09 [1.01 – 1.17] | < 0.01 | ||||||
| Social globalization | ||||||||||||
| Level 1 | Reference | Reference | Reference | |||||||||
| Level 2 | 1.92 [1.81 – 2.04] | < 0.01 | 1.70 [1.61 – 1.80] | < 0.01 | 1.70 [1.61 –1.80] | < 0.01 | ||||||
| Level 3 | 3.05 [2.88 – 3.24] | < 0.01 | 2.69 [2.54 – 2.86] | < 0.01 | 2.69 [2.54 – 2.86] | < 0.01 | ||||||
| Level 4 | 2.96 [2.76 – 3.17] | < 0.01 | 2.54 [2.37 – 2.73] | < 0.01 | 2.54 [2.37 – 2.73] | < 0.01 | ||||||
| Joint regression (levels) | ||||||||||||
| Economic globalization | ||||||||||||
| Level 1 | Reference | Reference | Reference | |||||||||
| Level 2 | 1.42 [1.33 – 1.50] | < 0.01 | 1.33 [1.25 – 1.40] | < 0.01 | 1.33 [1.25 – 1.40] | < 0.01 | ||||||
| Level 3 | 2.25 [1.94 – 2.62] | < 0.01 | 2.32 [2.00 – 2.69] | < 0.01 | 2.32 [2.00 – 2.69] | < 0.01 | ||||||
| Level 4 | 2.54 [2.22 – 2.92] | < 0.01 | 2.88 [2.51 – 3.30] | < 0.01 | 2.88 [2.51 – 3.29] | < 0.01 | ||||||
| Political globalization | ||||||||||||
| Level 1 | Reference | Reference | Reference | |||||||||
| Level 2 | 0.68 [0.60 – 0.76] | < 0.01 | 0.81 [0.72 – 0.91] | < 0.01 | 0.81 [0.72 – 0.91] | < 0.01 | ||||||
| Level 3 | 1.51 [1.34 – 1.71] | < 0.01 | 1.48 [1.32 – 1.66] | < 0.01 | 1.48 [1.32 – 1.66] | < 0.01 | ||||||
| Level 4 | 0.72 [0.64 – 0.82] | < 0.01 | 0.63 [0.56 – 0.71] | < 0.01 | 0.62 [0.56 – 0.71] | < 0.01 | ||||||
| Social globalization | ||||||||||||
| Level 1 | Reference | Reference | Reference | |||||||||
| Level 2 | 1.31 [1.21 – 1.41] | < 0.01 | 1.15 [1.07 – 1.23] | < 0.01 | 1.15 [1.07 – 1.23] | < 0.01 | ||||||
| Level 3 | 2.35 [2.16 – 2.56] | < 0.01 | 2.02 [1.85 – 2.20] | < 0.01 | 2.02 [1.85 – 2.20] | < 0.01 | ||||||
| Level 4 | 2.59 [2.34 – 2.87] | < 0.01 | 2.16 [1.95 – 2.38] | < 0.01 | 2.16 [1.95 – 2.38] | < 0.01 | ||||||
*No controls except time-fixed-effects
‡Controls at individual-level and time-fixed-effects
§Controls at individual- and country-level, and time-fixed-effects
#Odds ratio
&95% confidence interval
≠Levels defined through quartil
In the case of individual regressions controlled by confounding factors at the individual- and country-levels (column 4), the coefficient of the three indices of globalization (economic, political and social) were significant (p<.01), correlating an increase in overweight and obesity to a higher globalization score. In the joint regression, the coefficients of economic and social globalization remained relatively stable and significant. Individual regressions using the levels for total globalization indicated a concave relationship since there was a decrease in the association of globalization with overweight and obesity in level 4 compared to level 3. In the regression on economic globalization, only level 2, which showed an increase in overweight and obesity in relation to its base category (level 1), was significant. In the estimation of social and political globalization, all levels were significant, presenting a positive and concave relationship (with decreasing changes). Finally, in the joint regressions all coefficients were significant. However, the relationship with political globalization did not show a consistent pattern, but in the relationship of overweight and obesity with economic and social globalization, higher odds were observed at levels 3 and 4.
Discussion
Over the past two decades, several factors have changed the food supply in both developing and developed countries. In the context of the nutrition transition, globalization has affected the food supply chain, generating changes in consumption patterns. In this sense, access to new, processed foods has been influenced by the different dimensions of globalization, the economic dimension through changes in agriculture, trade, investment and marketing; the political dimension through the design of policies to integrate the global food market; and the social dimension through changes to culture and socioeconomic context that have impacted consumer behaviour.
While overweight and obesity have become a topic of global concern in the last several years, the figures for LAC countries are higher than the international average. By 2014, 58% of the LAC population was overweight, and about 23% were obese,4 thus generating a significant economic burden for the public health system. Projections for some LAC countries indicate significant increases in public health costs over the next 45 years (e.g. 70% in Chile and Mexico, 150% in Ecuador).25 However, as overweight and obesity are modifiable and preventable risk factors that can be altered by changing behaviours and lifestyles, it is essential to investigate the factors associated with this problem. This paper has explored the association between the different aspects of globalization (economic, political and social) and the probability of overweight and obesity in 10 LAC countries.
The specifications adjusted for individual- and country-level factors indicate a positive relationship between overweight and obesity and total globalization (table II, Column 4). Meanwhile, the coefficients obtained in the control variables (except the educational level) are related to previous studies.13,14,15 The association of education with the odds of obesity and being overweight seems to be contrary expectations, in that people with higher levels of human capital have more information about the risks of obesity and being overweight on health. However, among those with some education level, those at the highest level (higher education) showed lower odds of overweight and obesity, so higher education could be a protective factor. Additionally, education level coefficients could capture the association of individual income with obesity because it is associated with higher levels of human capital. Therefore, people with higher income levels have a higher opportunity cost of time, which could affect certain unhealthy behaviors, such as lower levels of physical activity or the consumption of unhealthy fast food.When total globalization is disaggregated into its different components, the economic, political, and social dimensions show a robust and positive association with the odds of obesity and being overweight. Estimates of total globalization and its sub-components, transformed into levels, indicate potential nonlinearities in behavior because the countries included in the middle levels (2 and 3) have increased odds of obesity and being overweight compared to the reference level. Meanwhile, the odds fall back to the level of more globalized countries, indicating a concave relationship.
On the other hand, the association of economic globalization with overweight and obesity has a smaller impact than the other dimensions. These findings are consistent with estimates made by Goryakin and colleagues15 and Costa-Font,14which emphasize a greater association with the political and social dimensions compared to the economic component.
This study has several limitations. First, it restricts the sample to non-pregnant women aged 20 to 49. While the age range could have been extended by 15 years, as in previous studies,15as BMI values during childhood and adolescence vary according to sex and age, the cut-off points that determine the nutritional status of individuals in the 0-19 age range are a function of these variables and differ from those used for adults.26 However, as some countries have only released data for single years, it was impossible to control for country- and time-fixed-effects simultaneously. To avoid or at least mitigate this bias, the regressions were controlled due to confounding factors at the country-level (GDP, human development index and economic freedom index). Finally, as the DHSs do not contain information on level of individual income, it was impossible to control the regressions based on this factor. One strategy that could have been used was the creation of a wealth index through a principal component analysis using variables related to household assets (such as access to potable water, wall materials and floors). However, this was not possible because not all countries report the variables needed to estimate this index.
Although the results of this study show a robust and statistically significant association, they cannot be used or interpreted in a causal way. However, it is important to begin analyzing health policies that mitigate the impact of globalization on overweight and obesity. This does not mean that policies aimed at increasing the level of globalization should be discouraged, as the benefits of globalization have been corroborated in many respects, such as economic growth27 and poverty reduction.28
Notably, not all dimensions of globalization show the same association with overweight and obesity. As stated above, it seems that the political and social dimensions, aspects of globalization that, until a few years ago, were not explored, have a greater association than the economic dimension; consequently, more research is needed on the political and social elements. For example, it is possible to advertise unhealthy food on media such as the Internet, television and newspapers, or increase retail outlets for fast food chains such as McDonald’s, which are directly associated with high-calorie foods, thus increasing the probability of overweight and obesity. In such cases, the implementation of regulatory policies such as the restriction of unhealthy food advertising tends to be weaker in developing countries. Do effective mechanisms exist to reduce their impact on the probability of overweight and obesity? These questions should be addressed to determine the most efficient strategies for minimizing the impact of the different dimensions of globalization on public health.

