











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Earthquakes are among the scariest natural disasters. We feel an earthquake as the shaking of the surface of the Earth, resulting from the sudden release of energy in the Earth’s lithosphere. This is the place called hypocentre-where every earthquake begins. This shaking is caused by seismic waves, which strength is biggest at the epicentre (directly above hypocentre)-the place at the surface where earthquake is most felt. The larger the distance from epicentre, the less impact is expected of an earthquake, but the real consequences will be determined taking into account other conditions. Earthquakes are also, in coastal regions, mostly followed by tsunamis.
Earthquakes can strike at any time and knowing that you can be sleeping or eating or having fun with your children and something could erase all that from your life in a split of a second is terrifying. Not knowing the exact moment when an earthquake can hit our daily routine (as we can do for tornados for example) makes it more difficult to deal with it. Today’s science and scientists are trying to foresee an earthquake, but the exact moment is still something hard to detect. However, we can say that we are much better prepared for an upcoming earthquake, than we were in the past.
During the history of mankind, some of the biggest and strongest earthquakes were recorded. The written facts tell a story of fear and consequences extremely sudden and hard to imagine. The first recorded earthquake occurred in 1831 BC in China (Mount Tai earthquake in Xia dynasty).1 From the earthquake in China to the invention of the seismograph, the intensity of the recorded earthquakes was estimated according to written documents. That is how we know about the earthquakes occurred in 464 BC in Sparta and 226 BC on Rhodes in Greece. The first detailed description of an earthquake in the new era is the one in Pompeii on February 5, 62.1 This earthquake destroyed the city; its recovery lasted until 79, when Pompeii disappeared due to volcanic eruptions. Since then, many earthquakes have hit the Earth, some of which have taken 50 000 or more human lives (table I).
Table I Earthquakes with 50 000 and more victims throughout hisory (based on data available on Internet - author’s search)
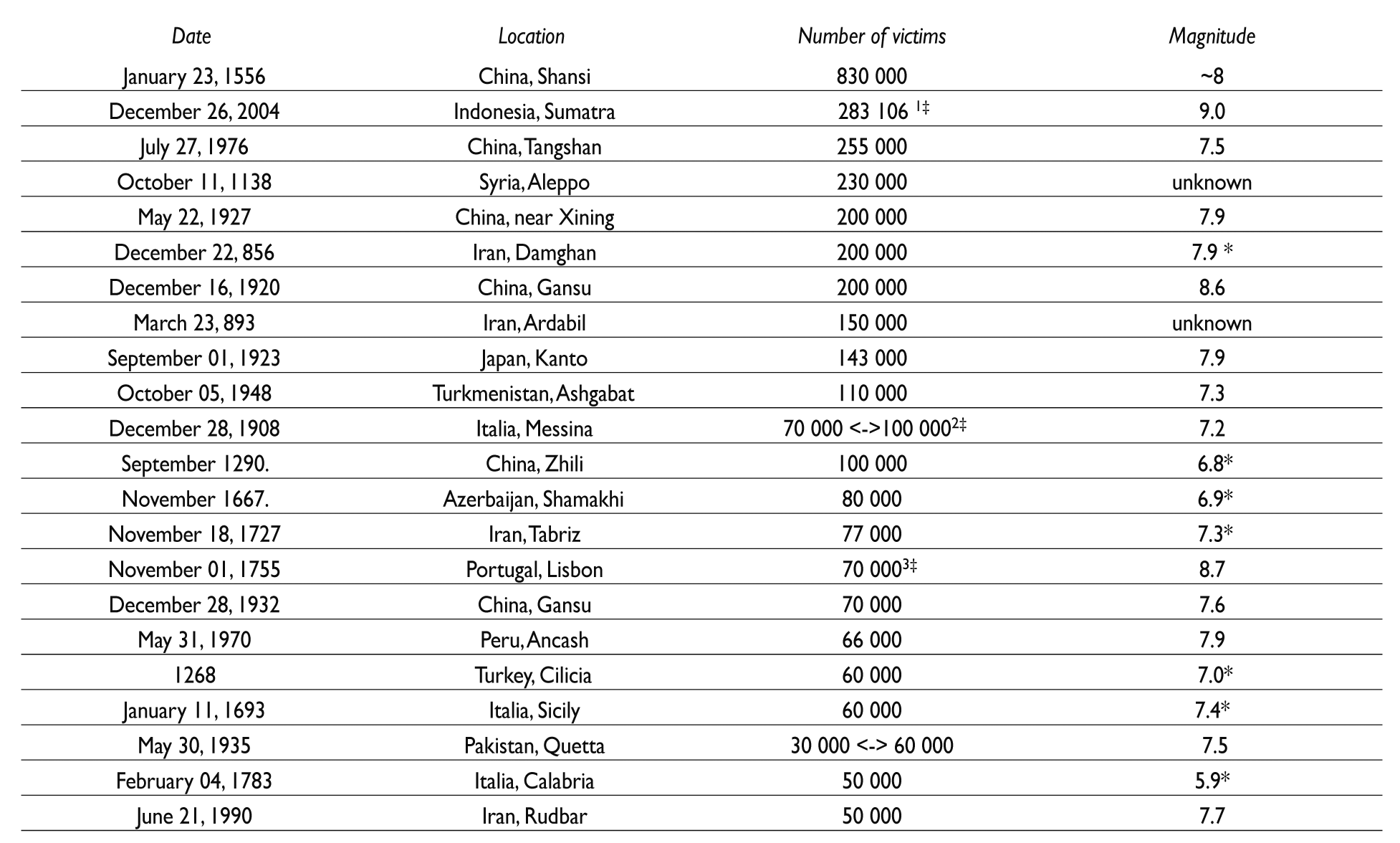
* Estimated value of magnitude based on historical documents
‡ Estimated total number of victims in earthquake and tsunami following the earthquake
Past earthquakes were described in historical documents and testimonies of survivors until the invention of the seismograph, when the measures of intensity and magnitude of earthquakes started to be systematically recorded. With the invention of the seismograph by Italian physicist Filippo Cecchi in 18752 begins the era of seismology: the study, measurement, monitoring and recording of the devastating earthquake effects. The seismograph registers the shift, velocity, or acceleration of the ground, by microseismic and macrosystemic methods. These methods describe the magnitude and intensity of each earthquake. Today’s shakes are monitored regularly, thus creating the presumption that earthquakes could be partly predicted. But there are still a lot of victims and damage caused by earthquakes and tsunamis following these earthquakes, even in the 20th and 21st centuries (table II).3,4
Table II The most intense earthquakes from 1900 till today with magnitude 8 and above (based on data available on internet - author’s search)

* Estimated total number of victims of earthquake and tsunami following the earthquake
There is really no such thing as earthquake prediction, rather forecasting. Probably it is better to say that today we are much more oriented to mitigation as a result of our own experience.5
The Richter magnitude scale was invented in 1935 by Charles F. Richter. It is determined from the logarithm of the amplitude of waves recorded by seismographs; values are expressed as decimal numbers in the 0 to 10 range (using Arabic numbers). Richter scale measures energy released from the hypocenter of the earthquake.6 But released energy is only half of the story. Another half is told by Mercalli-Cancani-Sieberg (MCS) scale (from 1917) which measures the intensity of an earthquake by quantifying its effects on humans, manmade objects/ structures, nature, earth surface. This scale was adapted and condensed and used as Modified Mercalli Intensity Scale (from 1931).7 MCS scale, in range from I to XII (using Latin numbers), was improved in 1964 (by Medvedev, Sponheuer and Karnik). They introduced a more detailed description taking into account quantity, classification of the damage and type of building structure, and their resistance to earthquakes. The new scale was named MSK-64, and also has XII grades. From 1978 on, this MSK-64 also considers impacts on environment (landscape changes).8
Today, using technology, new models for estimation of potential losses from earthquakes, floods and hurricanes, are developed; for example, Hazus. Hazus uses Geographic Information Systems (GIS) technology to estimate physical, economic and social impacts of disasters. It graphically illustrates the limits of identified high-risk locations due to earthquake, hurricane and floods.9
As we can see, it is not only the magnitude (or intensity) that defines the number of victims and damage. It is also the place, the environment in which an earthquake happens.
Environmental impacts
An example of how local soil conditions can greatly influence local intensity is given by catastrophic damage in Mexico City from the 1985, Mg 8.1 Mexico earthquake centered some 300 km away. Resonances of the soil-filled basin under parts of Mexico City amplified ground motions for periods of 2 seconds by a factor of 75 times. This shaking led to selective damage to buildings 15-25 stories high (same resonant period), resulting in losses to buildings of about $4.0 billion and at least 8 000 fatalities.6
There are two big areas prone for seismic activity: Circum-Pacific and Mediterranean/Trans-Asian belt. Circum-Pacific belt (also known as The ring of fire) is a horseshoe-shaped seismic belt. It goes from Chile, along the West coast of South America, through Central America and Mexico, to the West coast of North America till the South of Alaska. It goes over the Pacific Ocean and on the other side goes from Aleutian Islands to Japan, Filipinas, New Guinea, Southwest Pacific islands till the New Zealand. This belt covers almost 81% of all earthquakes’ released energy.10,11 The Mediterranean/ Trans-Asian belt goes from Canary Islands through Gibraltar, Mediterranean Sea, Apennine and Balkan Peninsula, through Turkey to part of Asia where it goes on through Caucasus and Armenian mountains over the Iranian plateau and Himalaya till Thailand, Sumatra and Java, where it is connected to the Circum-Pacific belt.11
We can say the earthquake danger goes all over the world. Thus, knowing the possible consequences of such disaster makes us stronger in preparing our disaster relief organizations, state agencies, and people. Unfortunately, history teaches us that nature is almost always one step ahead, but impacts of such disasters now can be much sooner detected and solved. Earthquakes can change environment in drastic ways with consequences that can be lethal for the affected population and remain in their environment for a very long time. The biggest problems arise when earthquakes hit densely populated areas, where changes in environment can make continuation of life difficult. Environmental impacts of earthquakes can basically be divided on direct and indirect ones.
Direct impacts will be felt immediately and will cause damage on structures, buildings and land, including ground failure, landslides, and seiches. The damage is influenced by the particularities of the affected area: coastal areas could expect tsunami followed by enormous floods; earthquakes caused or followed by volcano eruption can bring tons of ashes and fires. Direct impacts include big changes in land morphology as well (disappearance of existing lakes or formation of new ones, for example).
Indirect impacts are those that are mostly unforeseen but can cause long time problems in the environment. They include environmental pollution caused by harmful factors released from damaged factories, pollution of drinking water, broken water pipes that can flood land; ruptured gas, electrical and fuel lines lead to fire, especially in urban areas.12,13 Released heavy metals can pollute agriculture land for many years.13 Waste management could be hard to maintain, thus causing a lot of new harmful factors in environment. Thousands of buildings suddenly become debris and this overwhelms the capacity of waste management, says UNEP’s Muralee Thummarukudy, who is directing efforts to collect the waste for use in reconstruction projects.14 Hazardous material spills introduce sewage, medical, radioactive and poisonous material into the air, water and earth. Land without trees can be subjected to huge soil erosion problems.12,13,14
In the Japan earthquake (March 11, 2011; Fukushima) the subsequent tsunami destroyed a part of a nuclear plant and population was exposed to radiation. This consequence has both a direct and an indirect impact on population: radionuclides will persist in this environment for a very long time, causing health issues. There are some evidences from newly published papers stating that perinatal mortality in six severely contaminated prefectures jumped up from January 2012 onward.15
Lost vegetation or/and animal species will define (undermine) the progress of affected population once they are back. Environmental impacts are, thus, very important to be assessed while their strength and type will define expected medical and public health consequences in populated areas.
Medical impacts
Medical impacts will be mostly defined by the environment in which the earthquake happened: dense population, a lot of structures, non-seismic resistance buildings, affected elderly and/or children. In these situations, medical assistance will be much more challenging. Local health departments will be at the forefront of a disaster response, dealing with immediate trauma and also, together with public health professionals, with the long-term health consequences.16 The first medical principle: Primum non nocere should remain a priority even in disasters.
Medical treatment starts at the disaster place and will include triage, first aid, and transport of injured people. Triage in situ will include classification of injuries and prioritization in medical assistance and transportation, according to standardized international procedures and protocols.17,18,19
The first 24/48 hours is the period in which each affected country hardly could count on international help. In this period it is crucial to have professionals that could provide quick help: advanced procedures in injuries rehabilitation, surgical resuscitation procedures, anesthesia and analgesia in situ, and intensive care. Professionals must be well trained and follow existing medical protocols/procedures. Disaster protocol that is implemented in the very beginning of the event will assure surveillance and data on number and type of medical impacts. Selection of appropriate care standard, when there is overload of medical forces, is crucial.20,21
Medical impacts characteristic of earthquakes are: direct impact of trauma (fractures, musculoskeletal injuries, hemotorax, bleeding), burns, poisoning and related respiratory problems, neurological and cardiovascular symptoms, drowning (if tsunami follows earthquake).19,22
Typical injuries in earthquakes include crush syndrome and related conditions: kidney insufficiency (pressure of building material cause tissue necrosis and revascularization after excavation cause, by uric acid and myoglobin, intratubular obstruction); pressure on limbs (can lead to the amputation); hemothorax (traumatic injury to the chest). Kidney insufficiency must be prevented with early fluid resuscitation.23,24,25 Orthopedic injuries and their medical treatment are specially related to the lower limbs while they are most frequently injured. Amputation on disaster site is strongly related to higher mortality rate, thus logistic drawbacks must be avoided and adequate help to both patient and physicians, that are overwhelmed with situation and decisions, should be provided. Spine fractures are an important issue: a neurosurgeon team on a disaster site is an important asset during the response. When it is possible, conservative treatment for fractures should be encouraged at disaster site.26,27,28 Neurosurgical injuries demand correct triage procedures and prompt intervention with appropriate and qualified equipment. This will play a key role in reducing morbidity and mortality.29,30 An acute massive hemothorax demands immediate check and permanent control of the hemorrhage from the lung: by radical surgery or by artificial pneumothorax (which is the procedure of choice).25
In cardiovascular, neurological and psychiatric patients, first principle is to find out if they are chronic patients and then continue with their therapy in order to prevent exacerbation of the primary disease. Other cardiovascular, neurological and psychiatric symptoms include acute episodes caused by stress or trauma, in which situation follow-up and adequate therapy is needed.22
Last but not least are conditions that need blood transfusion. In disasters, when a lot of blood is needed, is it quantity over quality principle the right one? If the blood stock is devastated and supply depends on donors, screening of donated blood and the quarantine of it and its components represent critical processes that should be followed to ensure that units are safe. In a situation where this cannot be achieved, international blood supply should be considered.31
Public health impacts
After the earthquake, the resulting sanitation problems will bring up cases of dysentery, malaria and drug-resistant tuberculosis among poverty-stricken population. Trash-filled beaches, smelly waterways, swarms of dead fish and tons of floating debris will bring water pollution problems-now exacerbated by the earthquake.14 Environmental health includes air quality, water quality, weather/climate change, food safety, healthy housing, waste/sanitation, infectious disease/vector control, radiation, injury prevention, emergency preparedness, and toxicology. All of these aspects will be present in public health impacts of earthquakes, followed by specific interventions.32
During and after an earthquake public health professionals will deal with specific problems: water, food and drug supply (especially for those with chronic disease-thus pharmaceutics protocols should be involved in general protocols); disinfection and sanitation; communicable diseases and epidemics, and psychology problems caused by panic and stress.18,33,34,35,36 Public health professionals will be also involved in organized help for disabled people; special surveillance for vulnerable groups (children, pregnant women, elderly, chronic patients), toxicology surveillance in environment; work in shelters; care on corpse disposal.34,35,36 When tsunami, after earthquake, is expected, things will be doubly demanding.
Communicable diseases cause most common problems. Water-borne or respiratory transmitted will be more frequent when a lot of people will spend time in crowded places (shelters). Proper disinfection, timely distributed pharmaceuticals and continuous follow-up will reduce occurrence of communicable diseases.34,35,36
Not only the place and rescue team’s access, but the total psychophysiological condition of the affected person will contribute to a smaller or greater survival capability. An average grown up person can survive up to three weeks without food, but only three to seven days without water. Vulnerable groups are specific because of their sensitivity: they are not equally resistant as the average population thus could present earlier or stronger consequences on declined environmental conditions. Timely supply of water and food will prevent malnutrition and related consequences, but this supply should be in accordance with the person’s psychophysiological condition (more caloric food for pregnant women for example).33
Earthquakes will cause, in the majority of survivors, symptoms of acute stress, often accompanied by fear, lack of sleep, and later by depression. Early implementation of mental care with specific therapeutic interventions will reduce subsequent posttraumatic stress disorders in survivors.37
Public health professionals will collect the necessary (epidemiological) data about morbidity and mortality (types and incidence); needs for shelters, water, food, drugs; and will be the most precious educators, at the disaster scene, related to health and survival. Based on collected data, organization of help will be much more concrete, thorough and faster; and, with the agreement of medical professionals, will offer uniform information to the affected population: where to go, how to act, who and when should seek immediate help, how to protect yourself and the closest ones. Accurate and timely informing is the best prevention of panic, as well as fast introduction of teams that will secure affected population and the area.35 Thus, good communication between teams and different groups involved in search, rescue, and medical and public health actions is crucial.
Conclusion
Those who forget history are doomed to repeat it. Popular proverb.
Earthquakes cause fear, panic, diseases, deaths and changed environment, leaving people in discomfort with their own vulnerability. Living in an earthquake prone area doesn’t make us more vulnerable. It is our ignorance of how to react that makes us vulnerable and lost. Thus, each country needs good disaster management with protocols specific for each expected type of disaster. These protocols must incorporate environmental, medical and public health aspects and must be very well implemented. These include educated inhabitants; trained teams involved in rescue, (eventual) migration/evacuation, medical treatments and public health actions; and educated and trained leaders. Responders also need help to better cope with their demanding job and ethical decisions, which must be given at individual and/or organizational level as well. The most important thing is to bring people back to their homes once the disaster threat is over, to rehabilitate areas as soon as possible. As with all disasters, earthquakes function circularly, thus it is very important to learn from previous events and improve existing protocols based on experience. There is no worse mistake as the one that is repetitive.

