











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The issue of drug use and its consequences in the US-Mexico border region has attracted much interest for several reasons.1,2 In Mexico, cities closer to the US are relatively more affluent compared to other parts of the country,3,4 and in some of these cities norms and law enforcement for substance use tend to be more liberal in order to attract foreign customers.5,6 Additionally, large border cities like Tijuana include in their population Mexicans seeking to migrate to the US; return immigrants, and deported Mexican nationals, a population mix conducive to a higher prevalence of drug use than in other parts of the country.7,8,9,10 In the US, cities closer to the Mexican border are relatively poorer than the rest of the country,4,11 making the proximity to cheaper drug markets appealing.12 Drug trafficking and associated violence in the border area has been a serious concern for law enforcement and public health officials in South Texas13 and leads to the image of border cities as places with high levels of risk for alcohol, drug use and drug use problems,14,15 even if the epidemiological evidence so far does not confirm this image, at least on the US side.16,17,18,19
The physical environment in which individuals live is one of the social determinants of health and the relationship between the socioeconomic inequalities of the neighborhoods and the consumption of illicit sub stances by the individuals who inhabit them has been studied for several years. Components of the environ ment are: the population structure that surrounds it (i.e., demographic composition), physical environment (including housing quality, population density and infrastructure), social environment (including social networks, social support and social capital), as well as formal and informal health and social services.20 Besides these general elements, the border area is distinctive from interior regions of the United States and Mexico in terms of exposure to stressors and other contribu tors to drug use and related problems. On the US side, border counties have higher rates of unemployment and poverty than the rest of the country. In Mexico, border municipalities conversely show below average poverty rates when compared to the national average. Further, recently the entire border region has suffered added stresses derived from the United States increasing border security efforts and a costly drug war in Mexico that has produced thousands of victims.
Surprisingly, only a handful of epidemiological, population-based studies have focused on the prevalence of illicit drug use along the US-Mexico border, either in US border cities16,18,19,21 or Mexican border cities.8,22,23,24 In particular, to date no binational research on the topic has been conducted comparing the so called “twin” or “sister cities” in the region. These are legally separate cities, in both countries, that nevertheless share strong binational cultural ties, often with family members living on both sides of the border. Health-related issues for these sister cities have been a matter of relevance, with alcohol and drug use starting to gain attention,25 but research is al most non-existent for drug use in sister cities. While some prior research has compared different cities along both sides of the border (especially, Harrison and Kennedy, and Wallisch and Spence17,19) these comparisons suffer from the lack of a common target population, common measures and methodology, similar time frame and common covariates. Updated information on drug use in this region would be important for implementing new programs for prevention and treatment for drug use and disorders in the area.
In the present study, we use data from the recently completed US-Mexico Study on Alcohol and Related Conditions (UMSARC), a cross-sectional survey of 4 796 randomly selected Mexican and Mexican-origin individuals interviewed between 2011 and 2013 in six metropolitan areas on both sides of the US-Mexico border.26,27,28 In these reports, border versus non-border comparisons suggest a complex mixture of effects. For instance, the co-occurrence of alcohol use disorder (AUD) and drug use disorder (DUD) symptoms was more common at the US border than off-border, as well as at the Mexican border, compared to off-border. Nevertheless, among current drinkers, prevalence of AUD was marginally greater at the US border com pared to the non-border, but the opposite was true in Mexico. Cities within countries may also be different, as exemplified by the finding of very high rates of past- 12-month AUD among Laredan men, which suggest the possibility of significant heterogeneity even within demographically similar border areas. No report from the UMSARC has solely focused on drug use and symptoms of DUD. Our main goals are to compare drug use (illicit and non-medical use of prescription drugs) for border and non-border cities in each country and to compare pairs of cities (“sister cities”) across countries. Our hypothesis is that, for both sides of the border, the prevalence of drug use will be higher in border than in non-border cities. A secondary goal is to put these prevalence estimates into the context of national prevalence estimates for both Mexico and the US so that we can shed some light on the prevailing image of border communities as places with rampant rates of substance use.
Materials and methods
The UMSARC is a cross-sectional survey that interviewed randomly selected respondents from 2011 to 2013 in metropolitan areas on both sides of the USMexico border. Household face-to-face interviews of about 45 minutes in length were conducted in the United States by the Public Policy Research Institute at Texas A&M University and in Mexico by the National Institute of Psychiatry (INP) in Mexico City. Sampling was carried out simultaneously on each side using a multistage
area probability sampling design with stratification by city. On the US side, primary sampling units (PSUs) were defined as census block groups with at least 70% Hispanic population, with blocks serving as the secondary sampling unit (SSU). In Mexico, PSUs were defined using the catalog of the census basic geo-statistical áreas (“áreas geoestadísticas básicas [AGEB]”), similar to block groups in the United States, with blocks within the AGEB serving as SSUs. On both sides, three households per SSU were randomly selected, with eligible residents defined as those aged 18 to 65 (both sides) and who were of Mexican origin (US side only). Eligible respondents were then enumerated, selecting the resident with the most recent birthday as the respondent. Each household was visited at least three times on different days of the week and hours of the day. If the randomly selected respondent was not immediately available for interview, up to three additional attempts were made to locate and interview this person. All interviewing was conducted by trained interviewers using a face-to- face, computerassisted interview. Interviews were conducted in either Spanish or English in the United States and in Spanish in Mexico.
Response rate
On the US side, the border sample consisted of respondents from the three Texas border metropolitan áreas of Laredo (Webb County; n=751) and McAllen and Brownsville (Hidalgo and Cameron counties; n=814); the non-border sample consisted of n=771 respondents from the metropolitan area of San Antonio (Bexar county). Together, the US samples reflected a combined cooperation rate of 84% (53.1% response rate) (as per the standard definitions of the American Association for Public Opinion Research29). We carried out parallel sampling in Mexico on respondents living in the respective border sister metropolitan areas (sister cities) of Nuevo Laredo (n=828) and Reynosa and Matamoros (state of Tamaulipas; n=821) and in the non-border metropolitan area counterpart of Monterrey (state of Nuevo Leon; n=811), reflecting a combined cooperation rate of 71.4% (63.3% response rate). By design, the cities of McAllen and Brownsville were sampled as a single stratum (as were Reynosa and Matamoros), so each was considered a single site.
Weights, instruments and variables
In both the United States and Mexico, we first weighted data to reflect the multistage clustered sampling design. Then we used a raking algorithm30 approach to iteratively adjust the sampling weights to match Census marginal distributions of education and the combined gender-by-age distribution, separately within each site.
Drug use in the past 12 months was assessed with items adapted from the Mexican National Addiction Survey 2008.31 It included illicit drugs and the nonmedical use of prescription drugs (i.e. that were not prescribed for the respondent or that were not taken as prescribed).
Illicit drugs included marijuana, cocaine or crack, heroin or opium, methamphetamines, hallucinogens and other recreational drugs. Prescription drugs included pain relievers, sedatives, stimulants and other prescription medicines. An indicator of ‘any drug use’ was created for the use of either illicit or prescription drugs. ‘Polydrug use’ was defined as using two or more of any of the drugs listed as illicit or prescription. Limited interview time precluded a comprehensive assessment of drug use disorders (DUD) so, as an alternative, we selected two items from the DSM-IV with a high prevalence of endorsement across different drugs:32,33 Recurrent use in physically dangerous situations, such as while driving or operating machinery, or injury while drinking (=hazardous use); and persistent desire, or unsuccessful efforts, to reduce consumption (=quit or control). The report of these two symptoms of DUD can be interpreted here as a marker of heavier drug involvement or possible problem drug use, but not as a diagnosis of drug use disorder per se.
We included other demographic and mobility variables known or believed to influence the prevalence of drug use and problem use as statistical controls in our main models. These were sex, age, education, employment, religion, marital status, whether the respondent was a native of the surveyed city and whether the respondent had visited the neighbor country in the past 12 months.
Data analyses
After estimating the prevalence of the demographic and mobility variables and the prevalence of drug use and DUD symptoms for each study site in the UMSARC, we estimated odds ratios (OR) for drug outcomes in logistic regression models,34 with statistical adjustment for sociodemographic and mobility variables. We used weights developed for the UMSARC as described previously. We estimated all model parameters, standard errors and 95% confidence intervals (CI) of coefficients using the Taylor series method implemented in Stata version 13.1 survey commands to adjust for the design effects, stratification, clustering and unequal weighting of the observations.*
Comparisons were made among cities within each country, with significance tests of cross-tabulations using the design-based Pearson Χ2 test. Model-based comparisons for each pair of cities within each country and for each pair of sister cities across the border, were estimated by logistic regression using Stata’s pwcompare command.‡
Results
Table I shows the distribution across the sample sites of the demographic and mobility variables, which were used as covariates to examine drug use outcomes, focusing on comparisons between border and off-border cities within each country. In the United States, while the three locations had similar age and sex distributions, some differences were apparent: San Antonio had lower proportions of college graduates, higher proportions in “other” occupations (which includes unemployment) and a higher proportion of individuals who were separated, divorced or widowed. San Antonians were also less likely to have crossed the border in the past year; Laredo had a higher proportion of individuals identifying as Catholic; and respondents in Brownsville/McAllen were less likely to be natives of their city. On the Mexican side, the three locations also had similar age and sex distributions. However, Monterrey had a higher proportion of college graduates, fewer people working full time and more Catholics and single people and Monterrey residents were less likely to have crossed the border during the past year. Additionally, there was a higher proportion of non-natives in both Nuevo Laredo and Reynosa/Matamoros.
Table I Distribution of sociodemographic variables across cities, by country. US-Mexico Study on Alcohol and Related Conditions (UMSARC), 2011-2013
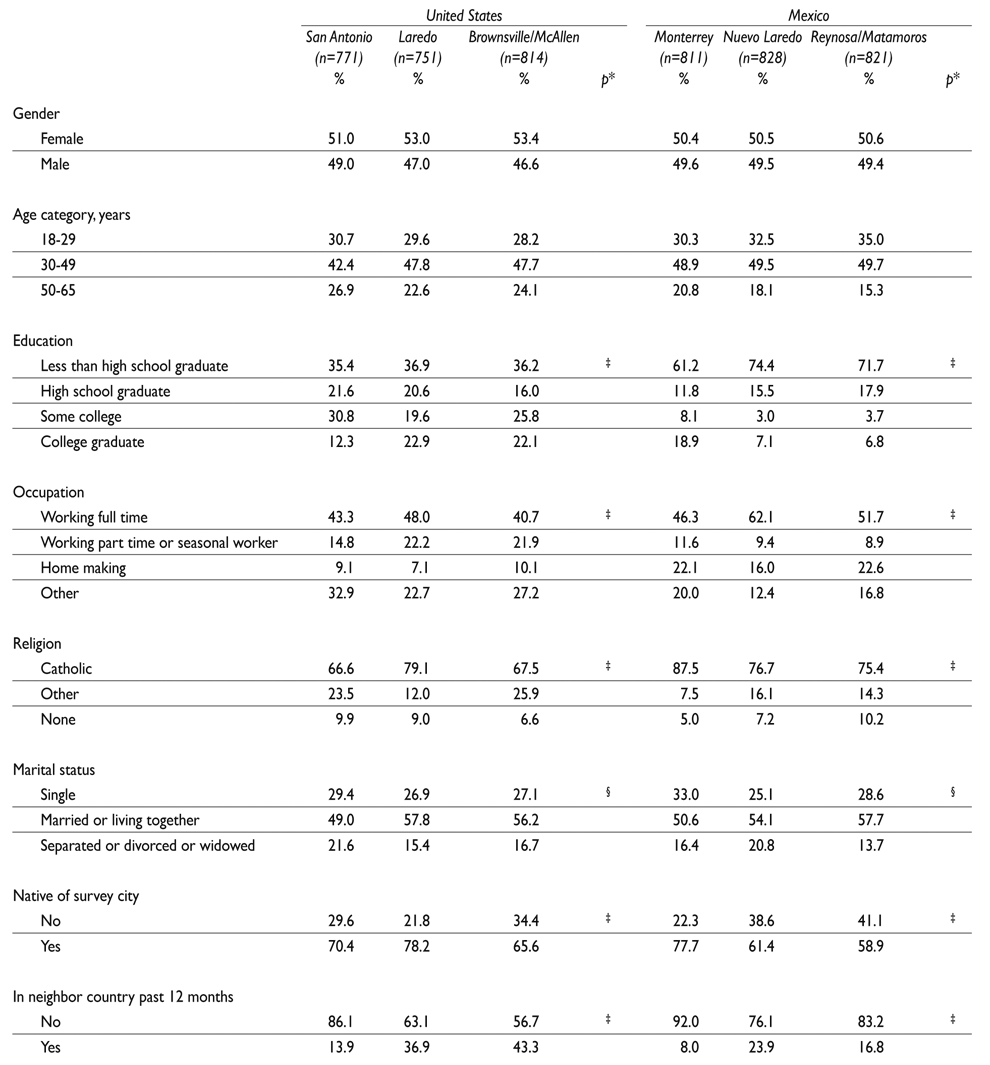
*Indicated p values are derived from chi-squared tests, adjusted for the survey design (within countries)
‡ p<.001
§ p<.01
Weighted column percentages. Missing values: United States: education (n=2), marital status (n=1), in neighbor country (n=1); Mexico: education (n=24), marital status (n=5), native of survey city (n=1), in neighbor country (n=7)
Table II shows the prevalence of past-year drug use and problems by study site. In the United States, the prevalence of any illicit drug use was similar across all sites, but prescription drug use, any drug use, poly drug use and symptoms of DUD were all higher in Laredo. While the marijuana prevalence rate was similar across sites, Laredo had higher rates of cocaine/crack and methamphetamines, while Brownsville/McAllen showed lower rates of heroin or opium use. In Mexico, site differences were found for any illicit drug use, any drug use and symptoms of DUD, which were all higher in Nuevo Laredo. The only individual illicit drug with a difference in rates across sites was marijuana, with higher rates also in Nuevo Laredo.
Table II Prevalence of past-year drug use and DUD symptoms, by country and city. US-Mexico Study on Alcohol and Related Conditions (UMSARC). 2011-2013
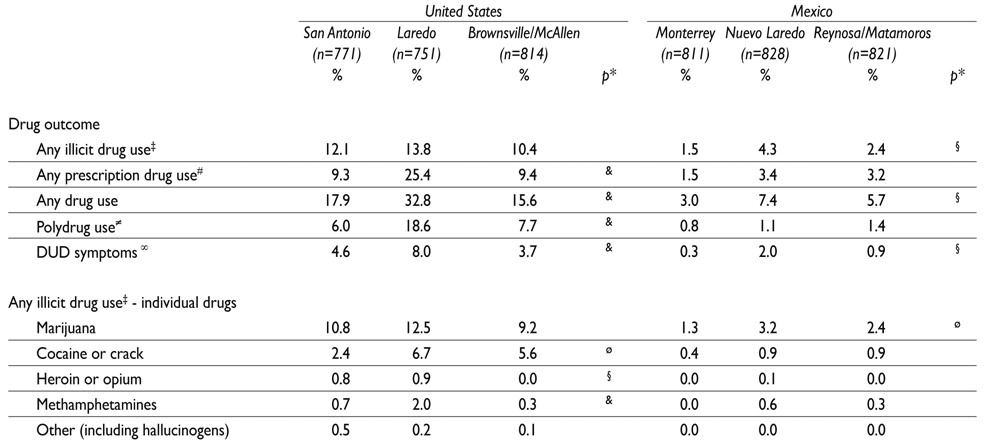
* Indicated p values are derived from chi-squared tests, adjusted for the survey design (two df; i.e., within countries)
‡ Illicit drugs are 1) marijuana, 2) cocaine/crack, 3) heroin/opium, 4) methamphetamines, 5) hallucinogens and 6) other recreational drugs
§ p<.01
# Use of prescription drugs that were not prescribed for the respondent or that was not taken as prescribed. Prescription drugs are 1) pain relievers, 2) sedatives, 3) stimulants and 4) other prescription drugs
& p<.001
≠ Polydrug use is defined as using two or more of any of the drugs listed as illicit or prescription
∞ DUD symptoms assessed were hazardous use and quit/control
ø p<.05
DUD = drug use disorder. Weighted percentages. Number of missing values ranging from n=2 (prescription drugs) to n=43 (DUD symptoms)
Table III presents border/non-border comparisons within country, adjusted by the demographic and mobil ity variables. Compared to the non-border site of San Antonio, all rates of past-year drug use and symptoms of DUD, with the exception of ‘any illicit drug use’, were higher in Laredo, but no differences were found in ‘any illicit drug use’ and symptoms of DUD for the comparison between Brownsville/McAllen and San An tonio. Among the border sites, Laredo, when compared to Brownsville/McAllen, had higher rates of drug use and symptoms of DUD (with the exception again of any illicit drug use). In Mexico, Nuevo Laredo had higher rates of drug use and symptoms of DUD (except for polydrug use) when compared to non-border Monte rrey, and Reynosa/Matamoros had higher rates of any prescription drug use and any drug use when compared to Monterrey. The two Mexican border sites differed only in Nuevo Laredo having higher rates of any illicit drug use when compared to Reynosa/Matamoros. Figure 1 presents graphically the adjusted estimates from table III. This figure shows that in Mexico, most point esti mate comparisons of drug use in border/non-border areas are above the null, while in the US this is true only for the Laredo/San Antonio comparison. While we searched for possible differences in effects by sex and age groups (18-29 and 30-65) by study site, we couldn’t find enough statistical support to report age or sex ef fects for all outcome variables. Especially for cities in Mexico, prevalence data became too sparse by sex and age groups for meaningful interpretations.
Table III Adjusted pairwise contrasts of past-year drug use and DUD symptoms by city, within countries. US-Mexico Study on Alcohol and Related Conditions (UMSARC). 2011-2013
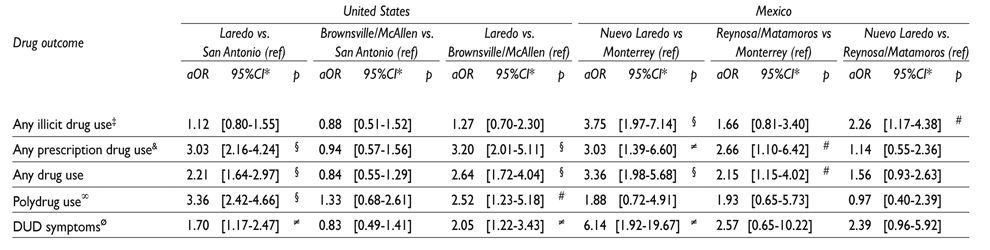
ref = Reference; aOR = adjusted odds ratio; CI = confidence interval; DUD = drug use disorder. Each row is a logistic model (for each country) with drug use or problem as dependent variable and city as independent, adjusted by sex, age (continuous), education (4 categories), employment (4 cat), religion (3 cat), marital status (3 cat), native of survey city and being in neighbor country in the past year
* Adjusted for the survey design
‡ Illicit drugs are 1) marijuana, 2) cocaine/crack, 3) heroin/opium, 4) methamphetamines, 5) hallucinogens and 6) other recreational drugs
§ p<.001
# p<.05
& Use of prescription drugs that were not prescribed for the respondent or that was not taken as prescribed. Prescription drugs are 1) pain relievers, 2) sedatives, 3) stimulants and 4) other prescription drugs
≠ p<.01
∞ Polydrug use is defined as using two or more of any of the drugs listed as illicit or prescription
ø DUD symptoms assessed were hazardous use and quit/control
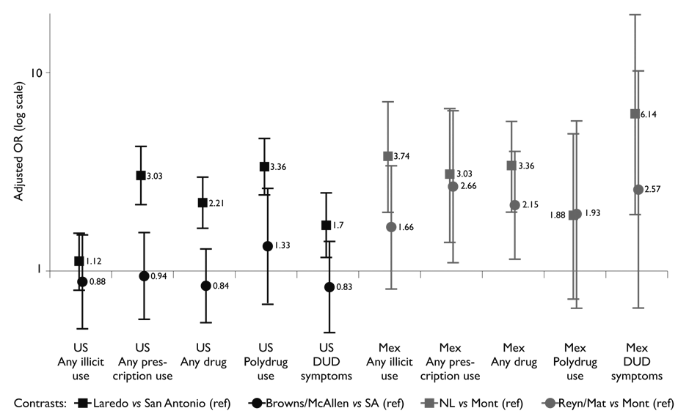
Figure 1 Pairwise contrasts of past-year drug use and DUD symptoms with city, adjusted by sociodemographic variables, by country
Table IV compares the rates of past-year use of any illicit drug, marijuana and cocaine/crack (the only substances whose sample size was large enough to compute reliable estimates) across “sister cities”, using multivariate models to adjust for key risk factors across these cities. Substantially higher rates were found in the US cities when compared to their Mexican coun terparts across the border, ranging from a low OR=3.75 (95% CI [2.53, 5.56], p< .001) for the comparison of any illicit drug use between Laredo and Nuevo Laredo to a high OR=11.01 (95% CI [5.93, 20.46], p< .001) for the comparison between San Antonio and Monterrey in rates of marijuana use. Interestingly, with only one exception (OR=9.52, 95% CI [3.27, 27.76] , p< .001), for cocaine/crack in the comparison Brownsville/McAllen vs. Reynosa/Matamoros), OR’s were lower for border sister cities than for the comparison of the two non-border cities.
Table IV Adjusted pairwise contrasts of past-year drug use by city, between countries. US-Mexico Study on Alcohol and Related Conditions (UMSARC). 2011-2013

aOR= adjusted odds ratio. Each row is a logistic model with drug use or problem as dependent variable and city as independent, adjusted by sex, age (continuous), education (4 categories), employment (4 cat), religion (3 cat), marital status (3 cat), native of survey city and being in neighbor country in the past year
* Adjusted for the survey design
‡ Illicit drugs are 1) marijuana, 2) cocaine/crack, 3) heroin/opium, 4) methamphetamines, 5) hallucinogens and 6) other recreational drugs
§ p<.001
The simple prevalence estimates of drug use shown in table II can be used to make raw comparisons with national estimates of drug use in both countries using published data from other surveys (data not shown). In Mexico, using the National Addiction Survey of 2008, we computed national averages of past-year prevalence rates of 1.8% for any drug use, 1.6% for illicit drug use, 0.4% for prescription drug use and 1.1% for marijuana use.31 All those rates are lower than the ones reported in table II for Monterrey (except for illicit drug use) and much lower than the ones reported for our Mexican border cities.
In the US, using the 2014 National Survey on Drug Use and Health,35 the national past-year prevalence of any drug use among Hispanics aged 18 or older (table 1.23B of the detailed tables of the survey) was 15.0%, 5.6% for prescription drug misuse (idem, table 1.53B) and 10.9% for marijuana (idem, table 1.28B).36 While the national Hispanic prevalence of any drug use and of marijuana use is not too different compared to the three US sites of the UMSARC as per table II (with the exception of Laredo), data from the UMSARC suggest a higher prevalence of prescription drug use in all three sites (and especially Laredo) than nationally.
Discussion
To summarize our results: 1) In the US, higher rates of any past-year drug use and symptoms of DUD were found only in the border city of Laredo, when compared to the non-border city of San Antonio; in Mexico, both Nuevo Laredo and Reynosa/Matamoros showed higher rates of drug use than the non-border city of Monterrey; 2) much higher rates (OR’s in the range of 4-11) were found in the US border and non-border cities when compared to their Mexican border and non-border counterparts; and 3) Compared to US national estimates, a higher prevalence of prescription drug use was found in all US UMSARC sites; in Mexico, the national com parison suggested that the three UMSARC sites had higher rates of use for all classes of drugs.
A main finding from this study is that the cities that we surveyed along the US-Mexico border are not homogeneous regarding drug use and this heterogeneity has also been documented previously in the UMSARC for alcohol use and disorders.27 The reason for this het erogeneity is yet unexplained and may be due to differ ences in preferences and availability of specific drugs, patterns of drug trafficking, violence and levels of stress in this dynamic region, all of which should be explored in more complex models than were possible here. Our hypotheses for factors affecting drug use were based on our prior studies of US border alcohol use and a future challenge would be to investigate the validity of these models on the Mexican side as well. The identification of Laredo as a high risk area, as shown both in this study and others,27 has potential important policy implications for the border area. Yet, the fact that some border cities in the US have drug use rates that are comparable to, or even lower than, those of non-border cities suggests the danger of portraying the entire border with a broad brush stroke.12,14,22
While a few previous comparisons of drug use37,38,39 have suggested that drug use and disorders are much more common in the US than in Mexico, to the best of our knowledge, this is the first time that representa tive epidemiological data from sister cities have been compared. Yet, this comparison is particularly relevant, as paired cities such as Laredo and Nuevo Laredo or Brownsville/McAllen and Reynosa/Matamoros are literally separated by only a bridge traversed by thousands every day. It was found that the sister cities of Laredo/Nuevo Laredo were both highest on drug use and DUD symptoms in each country and both localities are known for activities of drug cartels and drug related violence. We have been able to contribute to knowledge of comparative drug use prevalence in these cities with a study sample, design and covariates that ensured good population homogeneity across the sites and controlled for a complex set of probable risk factors. The even larger differences noted (OR’s of 9-11) between the non-border cities (San Antonio and Monterrey), as compared to the border sister cities, suggest that perhaps variations in social determinants are key to understanding differences in this otherwise demographically homogeneous population. More in-depth analyses of these differences in drug outcomes are needed to determine which factors drive them, but this study has made a start in ruling out some obvious ones. While nativity and immigration patterns have been shown in previous studies to be important in understanding drug use in this population,40 it is likely that inclusion of additional factors would enhance our understanding (e.g. Zemore and colleagues27).
It would be especially important to further explore factors associated with the high prevalence of prescription drug misuse, particularly in Laredo (25%), which cannot be solely attributable to access to Mexican border pharmacies,6 since it persists even after border crossings are taken into account. Rates of prescription drug misuse were also somewhat higher in both Brownsville/McAllen and San Antonio (9% each) as compared with rates for the US as a whole (5.6%, as per the 2014 National Household Survey cited above). It is possible that Mexican-origin border residents are accustomed to sharing prescription medications among household members both for expediency and cost and this kind of misuse may not represent an imminent danger of addiction per se. Yet, given the recent rise in prescription drug abuse and the severity of its consequences (fatal overdoses or progression to illicit drugs) observed nationally in the US, the high rates on the border are worrisome and worthy of further investigation.
Our findings that the border cities that we surveyed in Mexico were at high risk for drug use and symptoms of DUD as compared to elsewhere in the country are in line with those of other studies.8,9 Reasons for these higher rates are not immediately apparent, since the non-border city of Monterrey also showed some higher rates, so the finding seems applicable to the northern region of Mexico rather tan only the border cities. It is possible that greater levels of inequality in the relatively more affluent north may contribute to stress and risks for substance use.41 Our study is a first step towards greater understanding of the prevalence and patterns of drug use and problems in the binational border area, but many questions remain that deserve further research.
Public health actions on drug use and drug use disorders, that closely follows public health models that emphasizes drug use and health consequences of drug use beyond the mere prohibition and criminalization, is needed for the region.42 These measures should be broad in the actions and the type of organizations that are needed to implement such policies, ranging from clinical attention of affected individuals, to public health preventive measures and efforts to make treatment services readily available, improvements in schooling and, when necessary, effective measures to reduce the availability of substances for the population.43 While treatment for those in need is a central public health measure, but by no means should be an exclusive action, scarcity of resources in the US-Mexico border is especially worrisome. Previous work from our group has shown that in both countries, border substance users were about half as likely as non-border substance users to have wanted or obtained any kind of help, independent of predisposing, need and enabling factors, including migration status. Among those desiring help, however, about half had obtained it, both on and off the border in both countries.44 Actions to improve this complex situation are sorely needed.
Limitations
Some limitations to our study should be borne in mind. First, our three sister cities in the Texas-Tamaulipas border area were selected to ensure homogeneity of comparisons and are not necessarily representative of other sister cities on the border, such as El Paso and Juarez or San Diego and Tijuana, or of non-Mexican/Mexican-American populations there. Similarly, the non-border cities were selected for comparison because they were the closest large cities within 150 miles of their respective borders, but they cannot be considered representative of the entire interior of each country. Additionally, even though this study was conducted at the same time with the same methodology and questionnaire in both countries, the political, economic and security situation in Mexico was in particular turmoil during data collection and conditions affecting drug use there may not be stable. Nevertheless, our comparisons between sister cities are relatively robust, since we used the same study design, instrument and covariates and the data collection took place at roughly the same time. The somewhat low response rates are a concern, but we have shown elsewhere that this did not affect the validity of our estimates of alcohol or drug use.26,28 A further limitation is that our screening measure of DUD symptoms, which included only two of the 11 criteria of the new DSM-5 diagnostic, may underestimate the true prevalence of DUD, so our estimate of problem drug use should be considered a conservative one. Finally, our comparisons with national estimates are based on raw data (for Hispanics and not Mexican-Americans on the US side) and are not adjusted for key variables, so they should be regarded as suggestive only.
Conclusion
Despite these limitations, this study is the first to exam ine the prevalence of drug use and symptoms of DUD in a truly binational context. In the US, Laredo appears especially at risk for drug use, while in Mexico, Nuevo Laredo and Reynosa/Matamoros both show increased risk for drug use, yet lower risk than their US counter parts. On the US side, high rates of prescription drug misuse, especially in Laredo but also to some degree in the other study sites, are a concern and should be investigated further. These findings highlight the urgent need for reducing public health actions for substance use and substance use disorders in the US-Mexico border area, where, unfortunately, limitations for the treatment of substance use disorders abound.

