











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Anemia persists as the main nutritional problem in the world, affecting 42.6% (95%CI 37-47) of preschool children (273 million).1 According to the Global Burden of Disease Study 2013, the burden of anemia in developing countries accounts for 89% of all anemia-related disability.2 Prevalence of anemia is trending downward, however, as a result of improved health systems, lower mortality, and broader access to health services, among other causes.2 Nonetheless, despite the decline registered by Mexican surveys, prevalence remains high among the poorest and most vulnerable populations.3,4
In children under 5 y,2 anemia can have irreversible negative consequences for the higher intellectual functions of the brain if timely action is not taken.5 As for female adolescents, menstrual blood loss and increased iron requirements for growth at that age call for adequate iron-rich nutrition. Overall, anemia has been associated with increased morbidity and mortality among the most vulnerable populations.6
Data collected by surveys on anemia have proved insufficient to adequately analyze its principal causes and, hence, to prevent or correct its effects.3 For instance, the National Health and Nutrition Surveys (in Spanish, Encuesta Nacional de Salud y Nutrición, Ensanut) have clearly highlighted the role of iron deficiency (ID) as an important nutritional cause of anemia in Mexican children; however, the specific contribution of this deficiency to anemia cannot be pinpointed: among the few related biomarkers available for analysis, those that reflect ID can be underestimated due to the presence of inflammatory processes among other factors.7
The Mexican diet contains numerous dietary antagonists of iron absorption, such as phytates and polyphenols, owing to the high intake of corn tortillas among the population. Reports have suggested that iron intake among Mexican children and adolescents is insufficient to cover their daily requirements.8 Diet can thus be considered a risk factor for ID and anemia. It is noteworthy, then, that no studies have explored sources of iron by specific food groups, making it difficult to draw firm or reliable inferences for dietary policy and practice.
The aim of our study was twofold: to update existing information and provide new knowledge regarding prevalence of anemia among the Mexican children and adolescents who participated in the Halfway National Health and Nutrition Survey, 2016 (in Spanish, Encuesta Nacional de Salud y Nutrición de Medio Camino, Ensanut MC 2016), and to link our findings to the consumption of iron-rich food groups associated with anemia with a view to identifying opportunities for intervention.
Materials and methods
Study population. Our sample was drawn from the Ensanut MC 2016, a probabilistic, nationally representative survey with data disaggregated by regions and urban/rural strata. Analysis considered hemoglobin (Hb) data from 1 639 children aged 1 to 4.9 y; 3 181 aged 5 to 11.9 y; and 2 554 adolescents aged 12 to 19 y. Demographic and socioeconomic information was collected using ad hoc questionnaires. A detailed description of design and sampling procedures has been published elsewhere.9
Definition of variables
Anemia. Capillary Hb was measured using a portable HemoCue Hb photometer (HemoCue, Angelholm, Sweden). Anemia was determined when Hb concentration adjusted by altitude was <110 g/L for toddlers aged 1 to 4 y, <115g/L for children 5 to 11y, Hb<12 g/L for females aged ≥12 y and male children aged 12 to 14 y; and Hb<12g/L for males aged ≥ 15 y.10
Indigenous ethnicity was defined by whether an indigenous language was spoken at home. Localities with less than 2 500 inhabitants were considered rural, and otherwise classified as urban. A Household Wealth Index (HWI) was constructed based on household characteristics and family assets estimated through principal components analysis; the Index was divided into terciles being one as the lowest HWI score. Mexico was divided into four geographic regions: Northern, Southern, Central, and Mexico City, as in previous surveys.9 Anthropometric data (weight and height) were collected using validated and standardized methods.11 Body mass index (BMI) and nutritional status (underweight, wasting and stunting) were computed for preschoolers according to WHO standards.12,13
Children and adolescents participating in social programs were classified as Prospera and Liconsa beneficiaries.
Dietary information
Trained and standardized personnel administered a 7-day semi-quantitative food-frequency questionnaire (SFFQ) to participants, and entered the dietary data using computers in the field.14 Mothers reported the foods consumed by children in the seven days prior to the survey; adolescents responded to the questionnaire themselves in the presence of their mothers. Food consumption was calculated in grams (g) and milliliters per day. Total iron (heme and non-heme), fiber, calcium and energy were estimated using the food composition tables compiled by the National Institute of Public Health (INSP by its Spanish initials).*,4 For the purpose of analysis, the principal iron-rich food groups were beef, pork and chicken; viscera; Liconsa milk; and beans. Corn tortillas were also taken as a relevant food group because their consumption can interfere with iron bioavailability. Respondents who reported consuming one or more food items above the 99th percentile (in grams) were excluded from analysis.
Statistical analysis
Sample characteristics and prevalence of anemia, estimated by frequency and 95% confidence intervals, were stratified by age group. Logistic regression models were constructed to test the variables associated with anemia: sex, age, BMI, HWI, nutritional status, ethnicity, rurality, geographical region, Prospera/Liconsa program affiliation, and consumption of iron-rich food groups.
All analyses were adjusted for the survey sampling design using the STATA SE v14 SVY module for complex samples (College Station, USA). Statistical significance was set at α=0.05.
The INSP Research, Ethics, and Biosecurity Committees approved the survey protocol. Prior informed consent was obtained individually from the parents of all participants.
Results
Table I illustrates the descriptive characteristics of the sample by age group.
Table I Descriptive characteristics of Mexican children and adolescents. México, Ensanut MC 2016
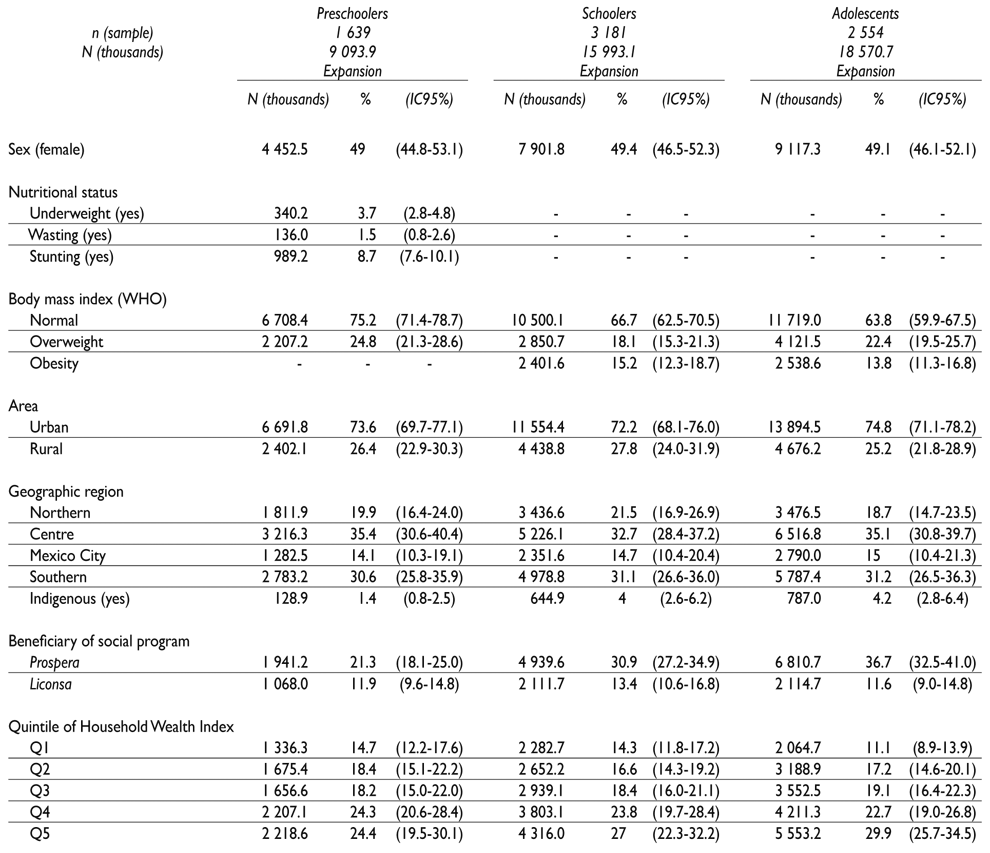
Ensanut MC: Encuesta Nacional de Salud y Nutrición de Medio Camino (in English, Halfway National Health and Nutrition Survey)
Preschoolers
In preschoolers, the national prevalence of anemia amounted to 26.9% (95%CI 23.3, 30.9), representing an expanded population of 2.44 million anemic children. The 12 to 23-month age group yielded higher prevalence (37.9%; 95%CI 29.9, 46.7) than the 48 to 59-month age group (16%; 95%CI 11.7, 21.4), and females were affected more frequently than males (p=0.07). Prevalence of anemia was lower in children with overweight (OW) than in those with a normal BMI: 19.8 and 28.4%, respectively. No differences emerged between children benefiting from the Prospera/Liconsa programs and their counterparts, nor by HWI quintile, geographic area and ethnicity (table II). Prevalence of anemia in children under five years was not statistically different from that reported by the Ensanut 2012 (p=0.08) (figure 1).
Table II Prevalence of anemia in Mexican children and adolescents by sociodemographic characteristics. México, Ensanut MC 2016
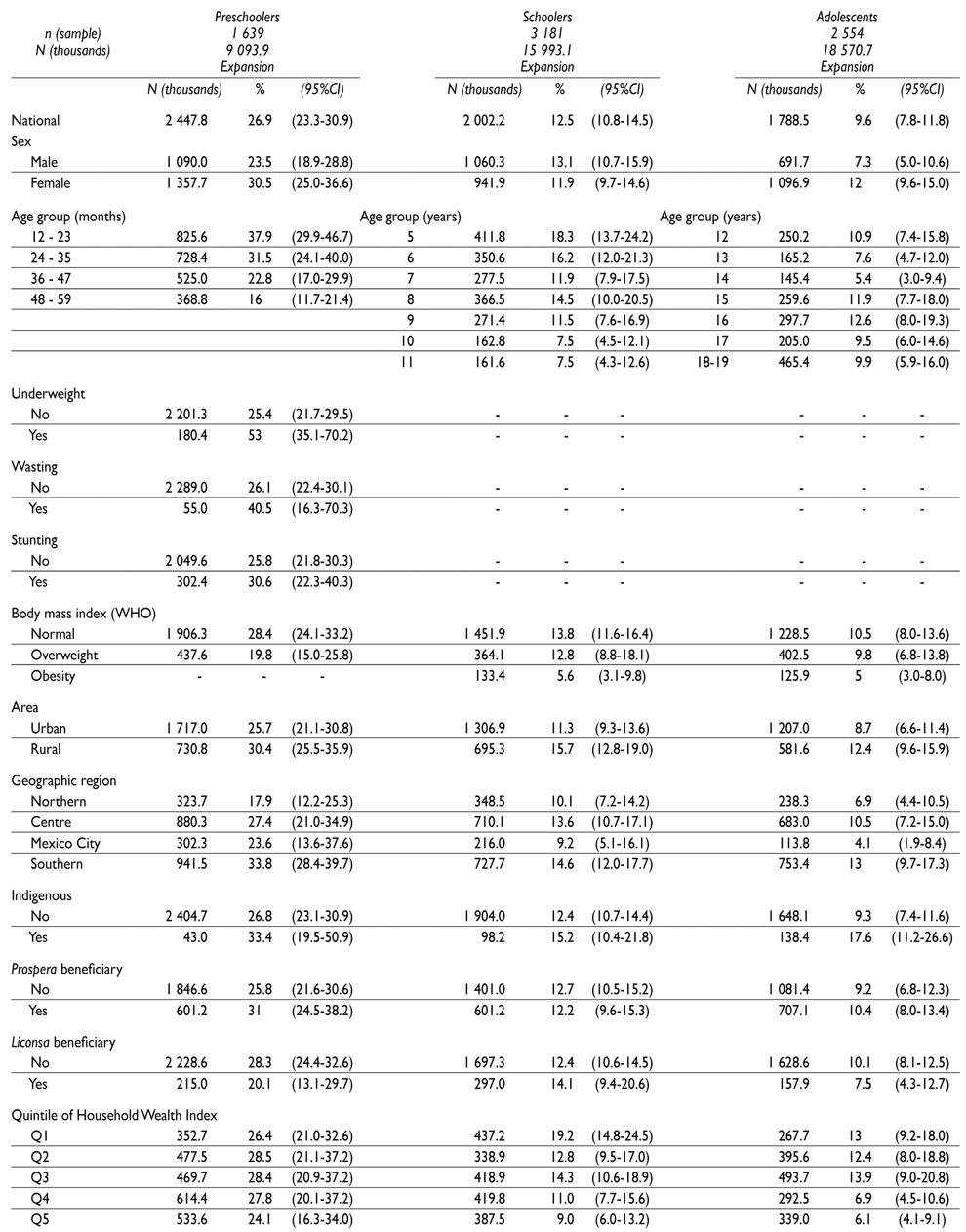
Ensanut MC: Encuesta Nacional de Salud y Nutrición de Medio Camino (in English, Halfway National Health and Nutrition Survey)
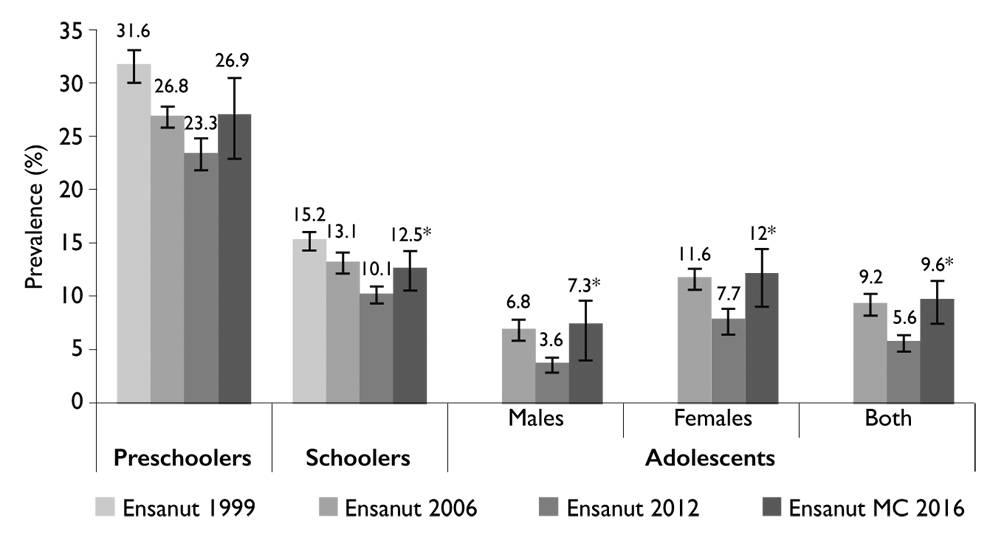
* Statistically different from Ensanut 2012, p<0.05
Ensanut: Encuesta Nacional de Salud y Nutrición (in English, National Health and Nutrition Survey)
Ensanut MC: Encuesta Nacional de Salud y Nutrición de Medio Camino (in English, Halfway National Health and Nutrition Survey)
Figure 1 Prevalence rates of anemia in Mexican children and adolescents from 1999 to 2016. México, Ensanut MC 2016
Consumption of iron-rich food groups
The proportion of preschool children who consumed beef and beans was higher in the non-anemic (38.2 and 82.5%, respectively) than in the anemic (26.9 and 73.2%, respectively, p<0.05) group (table III).
Table III Frequency of consumers by iron-rich food groups, among non-anemic and anemic population. México, Ensanut MC 2016
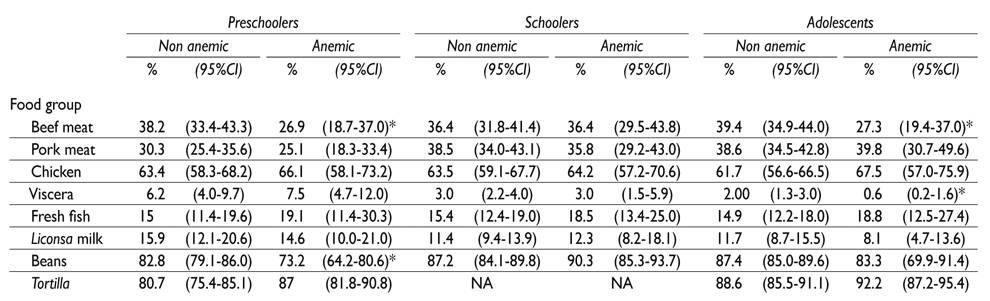
* Statistically different from non-anemic population, p<0.05
Ensanut MC: Encuesta Nacional de Salud y Nutrición de Medio Camino (in English, Halfway National Health and Nutrition Survey)
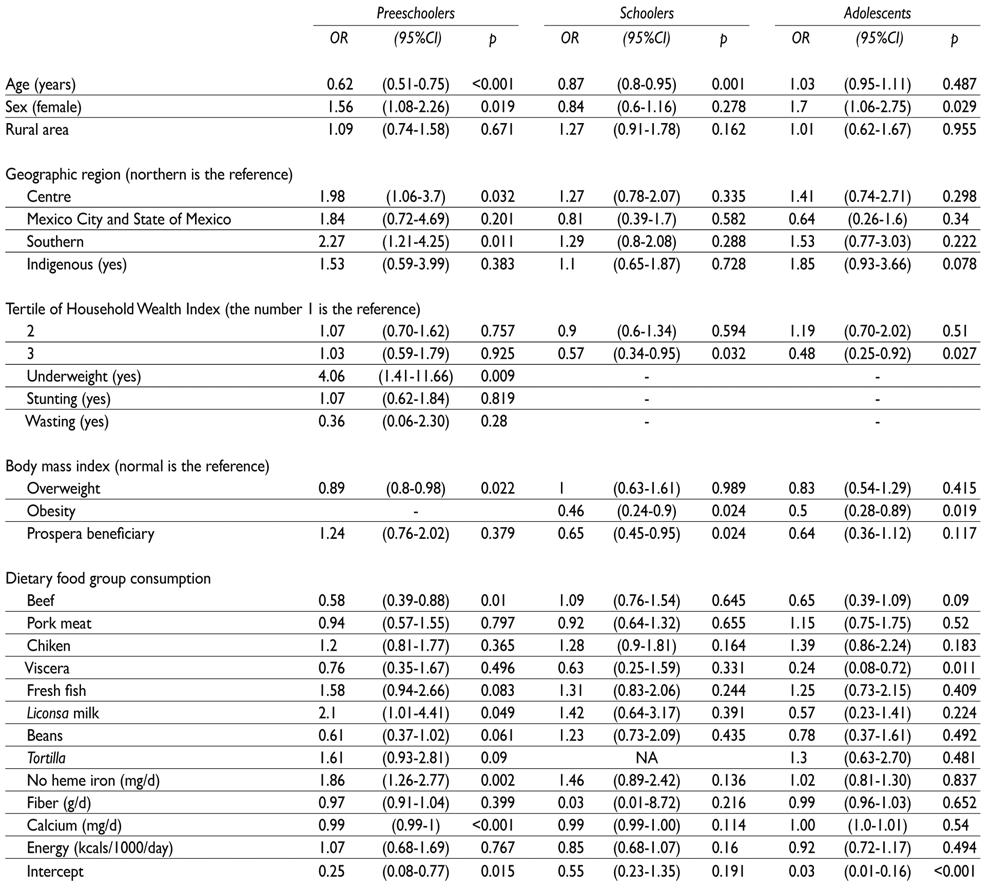
In the adjusted model, females (OR=1.5) living in the Central (OR=1.9) and Southern (OR=2.3) regions of Mexico, as well as underweight children (OR=4.0) were associated with higher odds of anemia (p<0.05). In contrast, older (OR=0.6) and OW (OR=0.9) children presented lower odds (p<0.05) for anemia (table IV). Children consuming beef (OR=0.6) and higher levels of calcium (OR=0.99) were associated with lower risk for anemia (p<0.05). However, those consuming non-heme iron (OR=1.8) and Liconsa milk (OR=2.1) were associated with higher risk (p<0.05) por anemia (table IV). Beans, tortillas and fresh fish were scarcely associated with anemia.
School-aged children
National prevalence of anemia in school-aged children was 12.5% (95%CI 10.8, 14.5), representing an expanded population of two million anemic children. Higher prevalence of anemia occurred in the five year old group (18%) compared with the 11 y group (7.5%, p<0.001). Children living in rural areas (15.7%) and in the South region (14.6%) yielded higher rates than their urban (11.3%) and Northern (14.6%) counterparts (p<0.05). Children with obesity (OB) (5%) suffered less frequently from anemia than those with a normal BMI (13.8%, p<0.01). Prevalence trended downward from the highest HWI quintil (p trend=0.007). No differences were observed by sex, ethnicity, or Prospera/Liconsa affiliation (table II). Prevalence in school-aged children found in our study was higher than that reported by the Ensanut 2012 (p=0.016) (figure 1).
Consumption of iron-rich food groups
Regarding the proportion of children who consumed iron-rich food groups, no significant differences emerged between the anemic and non-anemic groups (table III).
In the adjusted model, children who were older (OR=0.87), obese (OR=0.5), Prospera beneficiaries (OR=0.6), and in the third HWI tercile (OR=0.6) indicated lower risk for anemia (p<0.05) (table I). No food-group intake was associated with anemia (table IV).
Adolescents
National prevalence of anemia in adolescents was 9.6% (95%CI 7.8, 11.8), representing an expanded population of 1.78 million anemic adolescents. Higher rates were observed among indigenous (17.6%) and female (12%) vs. non-indigenous (9.3%) and male (7.3%) adolescents (p=0.016). Those residing in rural (12.4%) and Southern (13.0%) localities were affected more frequently than their urban (8.7%, p=0.06) and Northern (6.9%, p<0.05) counterparts. And those with obesity (5%) registered lower prevalence than those with a normal BMI (10.5%, p=0.006). Prevalence trended downward in the two highest as opposed to the three lowest HWI quintiles (p trend<0.001). No differences were observed by age or Prospera/Liconsa affiliation (table II). Compared with previous surveys, current prevalence of anemia in adolescents, by sex, did not differ from Ensanut 2006 results (p=0.8), but exceeded those of the Ensanut 2012 (p<0.001) (figure 1).
Consumption of iron-rich food groups
The proportion of adolescents consuming beef and viscera was higher in the non-anemic (39.4% and 2%, respectively) than in the anemic group (27.3 and 0.6%, respectively, p<0.05) (table III).
In the adjusted model, female adolescents (OR= 1.7, p=0.029) ranked a higher risk for anemia. Those who were obese (OR=0.5) and fell within the third HWI tercile (OR=0.5) were associated with a lower risk (p<0.05). Intake of viscera (OR=0.2, p=0.011) was also linked to a lower risk. The association of anemia with ethnicity and beef consumption was scarcely significant (table IV).
Discussion
In Mexico, anemia affects one out of every four preschool children, one out of every seven school-aged children and one out of every 10 adolescents. Across all age groups, the prevalence trends estimated in our study matched those of the Ensanut 2006 but exceeded those of the Ensanut 2012.3
Anemia continues to afflict to the most vulnerable sectors, that is, the indigenous, poorest and youngest populations, as well as children suffering from wasting. Despite federal initiatives including Prospera15 and Liconsa16 programs-which distribute iron supplements and iron-fortified foods, respectively, to the poorest populations-anemia remains the most severe nutritional problem across all population sectors in Mexico.4
According to the Global Burden of Disease Study 2013, the burden of anemia showed regional differences in prevalence owing to specific and widely varying causes. Factors as diverse as hemoglobinopathies, infectious diseases and iron-deficient diets have been found to cause anemia. In children under 5 years old, anemia is mostly due to iron-deficiency anemia (IDA).2 Data from the National Health and Nutrition Examination Survey 2010 (NHANES-2010) indicated a 3.9% prevalence of anemia among children 1 to 5 years (95%CI 2.5, 5.3), ID in 7.1% (5.5, 8.7) and 1.1% (0.6, 1.7) in IDA.17 In Mexican children, previous surveys have highlighted nutritional deficiencies as one of its major causes.18 Our study was limited by the lack of biomarker measurements for identifying total body iron, Vitamin-B12, folate, CRP and hepcidin. Such data would have allowed us to pinpoint the proportion of deficiencies in iron, vitamins and other minerals, as well as the presence of inflammation, as causes of anemia. In turn, this would have served to determine their contributions to the high prevalence rates reported by the Ensanut MC 2016.
Contrary to expectations, our findings indicated lower risk for anemia in preschoolers with OW, as well as in children and adolescents with obesity (OB). It has been documented that OW-OB are emerging risk factors for ID given their pro-inflammatory role in promoting increased hepcidin synthesis and restricted iron export activity in cells.7,19,20 While ID resulting from an inflammatory process (commonly promoted by OB) can lead to anemia of inflammation, cross-sectional studies of Mexican children have consistently demonstrated that a high BMI is inversely associated with anemia.3,21 García and colleagues found no association between low-iron status and OW/OB in a sample of Mexican children.22 In contrast, Cepeda-López and colleagues documented that OB was a predictor for low-iron status among Mexican children.20 Divergent results can be explained by the use of different biomarkers in defining ID. In Mexico, it is noteworthy that no studies have analyzed the association between BMI and anemia. Because cross-sectional designs allow for limited understanding as to how BMI trajectories influence Hb concentration over time, it is recommended that future studies explore such an association using a cohort design. Given the double burden of nutrition and the epidemiological transition Mexico has been facing, the dietary patterns of subjects with OW may be marked by greater vitamin and mineral density coupled with higher energy intake. In turn, this could be leading to higher Hb concentrations and lower prevalence of anemia in comparison with normal BMI subjects. Additional factors including a higher socioeconomic status (SES) in subjects with OW may also explain such an association. We did not explore SES data by statistical interaction; further analysis should be undertaken, stratifying by BMI, in order to better understand the ways in which SES, dietary iron absorption, adiposity and inflammation influence anemia among Mexican children and adolescents.
While dietary analysis under the Ensanut 2012 showed that iron inadequacy was highly prevalent among Mexican children and adolescents,8 it did not clarify whether this condition was associated with anemia. Given the dearth of studies using food groups to investigate such an association in Mexico, we decided to analyze the food groups richest in iron in an effort to elucidate the relationship between iron inadequacy and anemia. Our results indicated that beef and viscera, well-known sources of bioavailable heme iron, were associated with lower risk for anemia. Preschoolers exhibited the lowest risk, followed by adolescents. The highest association, found in adolescent consumers of viscera, indicated 77% lower odds of anemia compared to non-consumers. Intake of these foods has been widely recognized to improve Hb concentrations; however, only a small proportion of Mexican children and adolescents consume beef. This suggests that certain population groups (from non-indigenous, urban and higher SES sectors - data not shown) enjoy access to animal foods while others (from indigenous and poverty-ridden contexts) do not, with the latter living in conditions of high food insecurity.23 Chicken was the most frequently consumed meat across all age groups. Although proven to be an abundant source of iron,24 it was not associated with anemia. More comprehensive studies are required in order to gain a better understanding of results obtained thus far. Analysis should consider the amounts, types and frequency of meat consumed, use a 24-hour recall method, and establish a clear contrast between anemic and non-anemic populations. Our study aimed at identifying the association of iron-rich food groups with anemia.
According to our findings, food groups rich in non-heme iron such as beans and legumes were consumed extensively throughout the population, with intake declining, however, among anemic preschoolers: Prevalence of anemia among preschool consumers of beans was eight percentage points higher (33%) than among non-consumers in the same age group (25%, p=0.027) (data not shown). Intake was not different in other age groups; however, school-aged children yielded the highest proportion of bean consumers. This suggests that beans combined with other foods that facilitate iron absorption may be an effective dietary source of iron for preventing anemia.
Although other non-heme iron food groups were not evaluated in our study, we were able to identify that total dietary non-heme iron was associated with higher risk for anemia among preschoolers.
The iron-rich food groups associated with anemia in this study are also sources of other micronutrients that contribute to Hb synthesis such as Vitamin A, Vitamin B12, and zinc. The food-synergy approach may therefore be useful for understanding the interaction of diet with risk for anemia.25,26
The present study is subject to several limitations. First, a cross-sectional design rendered reverse causality an alternative explanation as regards the association of food groups with anemia, despite adjustment for confounders. Second, misclassification of food groups, under- and over-reporting of food consumption (specifically by subjects with OB and low body weight), and use of a food frequency questionnaire may have undermined accuracy in estimating the association between food group consumption and anemia. Third, changes in population-level determinants of anemia, particularly dietary intake, can influence trends. The upswing in prevalence over the past three years was unexpected. Although the three Ensanut consulted used the same method for measuring Hb and classifying anemia, and population characteristics remained unchanged during the period analyzed, we were unable to identify the underlying factors of increased prevalence. Methodological issues concerning Ensanut MC 2016 include seasonality for data collection.
The major strength of our study resides in its nationally representative samples of children and adolescents. Additionally, in a random subsample of this population, capillary Hb and venous Hb measured by means of a hematology analyzer yielded results that were consistently reliable, ruling out potential measurement bias. Our results provide updated evidence of the prevalence of anemia for policy makers, thus improving opportunities for interventions.
All of these findings pinpoint anemia as a serious challenge for public health nutrition, despite a number of efforts by the government to prevent it, especially in the vulnerable populations. The current nutrition policy relying on social programs such as Prospera and Liconsa should reinforce micronutrient supplementation and education for mothers of childbearing age. Studies that address the main causes of anemia more comprehensively in Mexican children are required as a basis for more targeted public health policies.
In conclusion, anemia is highly prevalent among Mexican children and adolescents, affecting mainly indigenous peoples as well as the youngest and poorest populations. Dietary sources of bioavailable iron remain as the main dietary factor associated with lower risk for anemia. Further analyses taking the whole diet as well as other demographic characteristics into account are necessary for improving dietary recommendations designed specifically for the vulnerable populations.

