











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Cancer patients are especially susceptible to invasive infectious diseases including blood stream infections. Immunosuppression induced by cancer itself or as a consequence of radiation or chemotherapy, such as neutropenia, or breakdown to mucosal barriers, the kind that occurs following long-term vascular catheter placement, synergize to make cancer patients particularly susceptible to Gram positive infections and among them, particularly those caused by Streptococcus pneumoniae.1
In Mexico, the Program of Specific Action of Cancer in Infants and Adolescents estimates 5 000 new cancer cases in persons <18 years of age with an accumulated incidence for years 2008-2013 of 9.4/100 000 affiliated to the Seguro Popular being the main mortality cause in children from 1-14 years of age.2 For adults >20-80 years of age, morbidity rates for 2013 ranged from 94 to 769.4/100 000 with a mortality rate of 13.6% of the total population. Immunization with the heptavalent pneumococcal conjugate vaccine (PCV7), which protected against serotypes 4, 6B, 9V, 14, 18C, 19F and 23F, began in early 2006 when this vaccine was applied gradually only in the municipalities with the lowest human development indices. In 2008, the application of this vaccine was universalized among the population under the age of one year. During the period from 2008 to 2010, PCV10 (PCV7 serotypes + 1, 5 and 7F) was introduced with a three-dose schedule to the pediatric population insured by the Instituto Mexicano del Seguro Social (IMSS), which attends half of the population. Since 2011, PCV13 (PCV7 serotypes + 1, 3, 5, 6A, 7F and 19A) has been used in a 2-, 4- and 12-month schedule as part of the universal immunization.3 PCV7 is no commercially available anymore. Pneumococcal polysaccharide 23-valent vaccine (PPV23) is included for all adult population >65 years of age or >60 years with any risk factor as a single dose, although coverage is limited.
Scare information regarding distribution of pneumococcal serotypes in cancer patients as well as concern regarding the increase of serotypes not included in the PCV prompted us to analyze this information in Mexico. Considering the availability of pneumococcal conjugate vaccines and changes in serotype distribution as well as the need for empiric antimicrobial treatment for cancer patients, we describe the serotype distribution of pneumococcal isolates before and after introduction of PCV in Mexico and the antimicrobial susceptibility pattern of the isolates.
Materials and methods
Surveillance of S. pneumoniae and clinical samples
In 1993, Mexico along with six other Latin American countries formed the Sistema Regional de Vacunas (Sireva) project coordinated by the Pan American Health Organization,4 and since that time, pneumococcal isolates from patients, children and adults with invasive and non-invasive diseases from 16 hospitals in 12 states, have been sent with demographic data to the Instituto Nacional de Salud Pública (INSP) in Cuernavaca, Morelos, México. As part of this passive laboratory surveillance, a retrospective observational study of consecutive pneumococcal isolates was conducted from patients with diagnosis of cancer. Two periods were considered: 1994-2007, before the introduction of PCV7 (pre-PCV7); and 2008-2016 (post-PCV7), after the introduction of PCV7. S. pneumoniae isolates from children, adolescents and adults were separated in two sub-groups: patients with diagnosis of hematological malignancies: acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), lymphomas and myelomas; and patients with solid tumors. Invasive pneumococcal disease (IPD) was defined by the isolation of S. pneumoniae from blood and/or cerebrospinal fluid (CSF). Community acquired pneumonia and complicated pneumonia were defined for those patients with clinical diagnosis of pneumonia and positive culture for S. pneumoniae as a single culture from pleural fluid and/or bronchoaleveolar lavage. Other sites of isolation included middle ear, peritonitis, arthritic fluid and eye discharge.
Microbiological studies
Once in the laboratory, pneumococcal isolates were re-identified by standard procedures that included tests for bile solubility and optochin sensitivity. Pneumococcal isolates were serotyped by the Quellung reaction with type- and factor-specific antisera (Statens Serum Institut, Copenhagen, Denmark). Antimicrobial susceptibility tests for penicillin, cefotaxime, vancomycin, erythromycin, chloramphenicol and trimethoprim/sulfamethoxazole (TMP/SMX) all from Sigma-Aldrich, (St Louis MO,US) were performed by the broth microdilution method to determine the minimum inhibitory concentration (MIC) and clinical interpretation according to the procedures of the Clinical and Laboratory Standards Institute (CLSI) using cation-adjusted Mueller-Hinton broth (CAMHB) supplemented with 3% lysed horse blood. Interpretative criteria were differentiated for meningitis and non-meningitis isolates to penicillin and cefotaxime according to CLSI. S. pneumoniae ATCC 49619 was used as the control strain.5
Statistical analysis
An analysis was carried out comparing age and type of tumor. A second analysis was performed comparing pneumococcal serotypes included in the PCV with type of tumor, age and pre- and post- vaccine periods, both with chi-square test. All the analyses were performed using SPSS version 20. p-values ≤0.05 were interpreted as statistically significant.
Ethical statement
The study was submitted for ethical approval and it was exempt by the Research Ethics Committee at the INSP considering it was performed with S. pneumoniae isolates that resulted from standard microbiological diagnostic procedures as requested by the treating physician. No additional biological specimens were taken for the purpose of this study. Specimens were anonymized and only data on year and month of birth, sex, type of specimen and hospital/ laboratory were registered.
Results
During the period 1994-2016, a total of 3 249 pneumococcal isolates clinical isolates were recovered from 16 participant hospitals from the passive laboratory pneumococcal surveillance SIREVA-Mexico. From them, 175 (5.4%) were recovered from patients with diagnosis of cancer. All patients were receiving active chemotherapy at the time of infection and were hospitalized. There were 78 (45%) female and 97 (55%) male patients. Eighty six (49.7%) patients were ≤17 years old and 89 (50.8%) ≥18 years of age. The median age and interquartile range (IQR) of pediatric patients were 5 years (IQR: 3 to 8.3 years of age) and 54 years for adults (IQR: 36.7 to 66.8 years of age). Overall, there were 105 (60%) cases of hematological malignancies and 70 (40%) cases of solid tumors. Hematological malignancies were present in 66 (63%) patients ≤17 years of age compared to 39 (37%) in patients ≥18 years of age (p= 0.000), while solid tumors were present in 21 (30%) and 49 (70%) in each age group respectively as shown in figure 1. Bacteremia was the most frequent clinical presentation found in 108 (61.7%) patients followed by pneumonia 47 (26.9%), meningitis 10 (5.7%) and other diagnosis in 10 (5.7%) patients. Bacteremia was more frequently associated with hematological malignancies 75 (71.3%) (p= 0.001) and solid tumors were more frequently associated with pneumonia 43 (61.7%) but this association was not significant. Serotypes 19F, 19A, and 35B, were the most common serotypes in patients with hematological cancer. In patients with solid tumors, serotypes 3 and 19A were the most common isolates with serotype 3 as the most important isolate in adult patients as shown in figure 2. Serotypes included in PCV10, PCV13 and PP23V for hematological and solid malignancies were 34 (32.3%) and 20 (28.5%); 59 (56.2%) and 46 (65.7%); and 67 (63.8%) and 53 (75.7%), respectively. Theoretical serotype coverage for PP23V for patients older than 18 years of age was 69.2% in the pre-PCV7 and 68.3% in the post-PCV7 era (p=0.54). Pneumococcal serotype distribution according to period of isolation and age of patients is shown in table I. Serotype 19A was significantly more frequently isolated after introduction of PCV7 (p= 0.0052). Considering the capsular types causing infections in the population investigated, PCV10 and PCV13 would have an estimated overall coverage of 31.5 and 60.5% respectively.
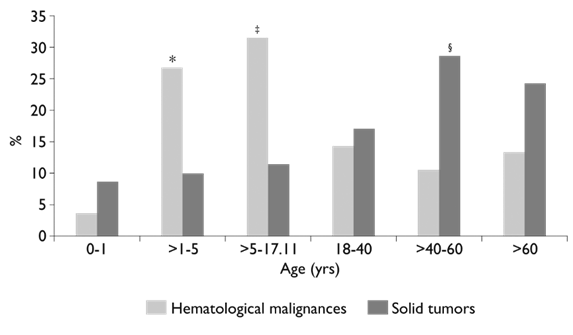
* p= 0.007
‡ p= 0.002
§ p= 0.0041
Figure 1 Distribution of age and type of cancer in patients with pneumococcal diseases in Mexico (1994-2016). N = 175 cases
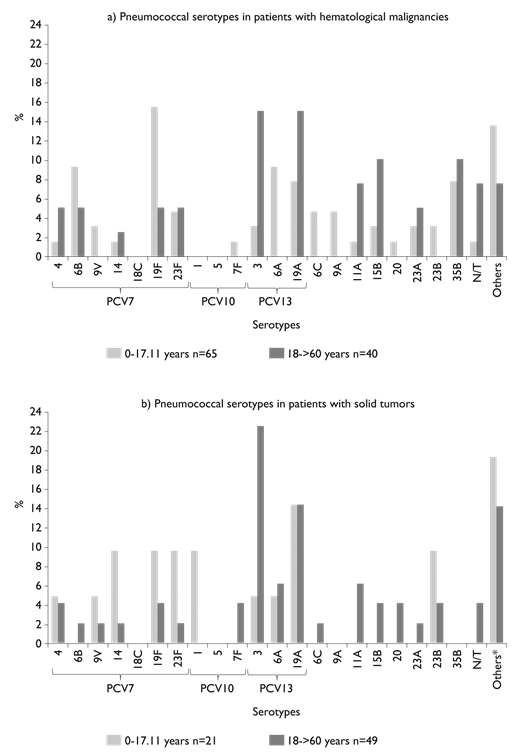
*Other serotypes include one strain each with the following serotypes: 2, 7C, 8, 9N, 10A, 13, 15A, 16F, 17F, 18A, 18C, 19B, 20, 31, 35A, and 35C
N/T Non-typable serotypes
Figure 2 Pneumococcal serotype distribution according to cancer type and age in Mexico
Table I Distribution of S. pneumoniae serotypes causing invasive and non-invasive diseases in patients with cancer before and after introduction of PCV7 in Mexico, 1994-2016
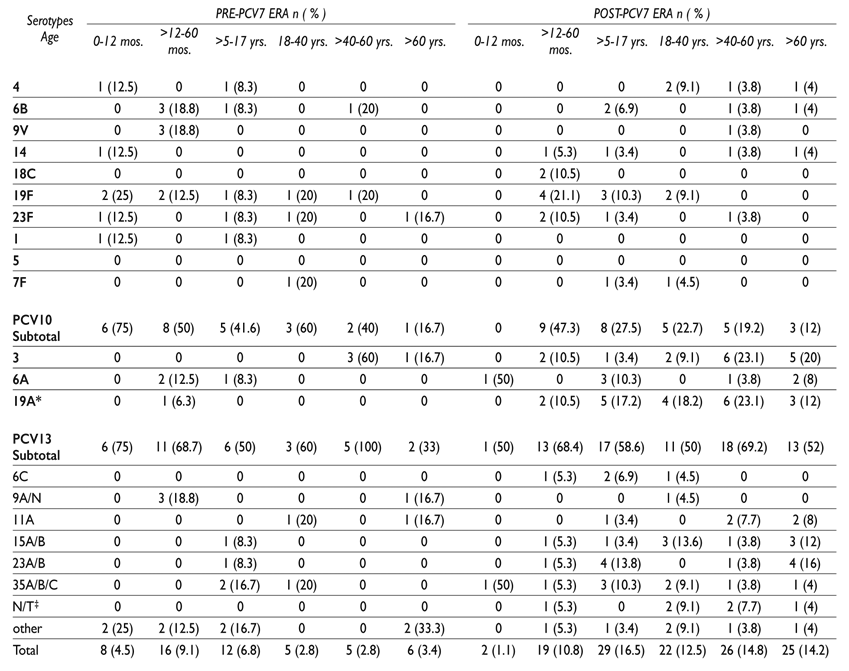
* P= 0.0052
‡ N/T = Non-typable serotypes
mos. = months; yrs. = years
Serotypes included in PCV are in bold
Antimicrobial susceptibility in the pre and post-PCV7 era is shown in figure 3. Fifty two pneumococcal strains were recovered in the pre-PCV7 period and 123 in the post-PCV7 era. An increase in penicillin and TMP/SMX resistance was observed in the post-PCV7 period mainly because of resistance of serotype 19A (data not shown). No significant differences were found in antimicrobial susceptibilities in both periods.

Discussion
S. pneumoniae is a pathogen that affects healthy and immunocompromised population and among the last, cancer patients are especially susceptible to severe pneumococcal infections like bacteremia and pneumonia as has been recently shown in Spain6,7,8 and in the United States1,9 among others. In this study we observed a significantly increase in hematological malignances in pediatric patients with a concomitant increased in bacteremia caused by S. pneumoniae, compared to solid tumors in adults. Phillips R.S and colleagues10 performed a risk-prediction model for outcomes of episodes of neutropenic sepsis based on clinical and laboratory data at presentation in patients aged 0-24 years old. Univariable analyses showed association with microbiologically defined infection in many items, including higher temperature, lower white cell counts and acute myeloid leukemia, or relapsed acute leukemia, but not age. Patients with osteosarcoma/Ewing sarcoma and those with more severe mucositis were associated with a decrease risk of infection. These results are in accordance to what we found regarding an increased risk of infection with hematological malignancies compared to solid tumors but the limited number of cases and lack of more relevant clinical data did not allow making further associations.
The serotype distribution reported in this study reflects better serotype coverage with PCV13 mainly derived by the elevated frequency of serotype 19A, in the post-PCV7 period, which is not present in PCV10 and it does not differ from pneumococcal serotypes causing infections in non-cancer patients reported previously.11 In this study, serotypes 3, 19A and 35B were the most frequent pneumococcal serotypes in adult patients. The presence of serotypes 15B, 23A, 23B and 35B, not included in any PCV is important. This has to be considered when following vaccine guidelines and reinforce the use of PPV23 after the last dose of PCV13. The proportion of serotypes causing pneumococcal diseases covered with the PP23V was the same for adult patients in the pre and post-PCV7 period with almost 70% of serotype coverage. Thus, we do not observe a herd effect as a consequence of the introduction of PCV7 in children ≤2 years of age for this particular population making vaccination with PP23V very important for cancer patients. In Brazil, Cardoso NT and colleagues12 reported the prevalent pneumococcal serotypes in cancer patients for year 2013-2014 in 50 isolates as 23F (12%), 6A (8%), 3, 4, 20 and 23A (6% each) reflecting most non-vaccine serotypes as they use PCV10 with universal access for all children less than 2 years of age.
Similarly to studies conducted by Garcia-Vidal and colleagues6 a large diversity of capsular types was found to be associated with diseases among the population investigated, although types differed in prevalence. This fact may be related to the immunocompromising conditions of the disease itself or to therapies that such patients usually undergo that significantly decrease the immunological system functions and allowing less common capsular types to cause infections.
Recently, guidelines for vaccination of the immunocompromised host were published by Rubin and colleagues on behalf of the Infectious Diseases Society of America (IDSA)13 and for vaccination in pediatric hematology and oncology patients by Cesaro and colleagues.14 Both groups coincide on the importance of vaccinations during and after treatment for pediatric and adult cancer patients, despite the fact that chemotherapy suppresses the immune response and recovers up to 6 to 12 months after the end of treatment. Particularly for S. pneumoniae, it has been shown that in children treated for ALL, lymphocyte subpopulation levels decrease during treatment but recover functionally by 6 months after completion of chemotherapy.15 However, both in children treated for ALL and AML, pneumococcal serotype-specific IgG antibody levels are non-protective thus the risk of pneumococcal disease is increase in this group of patients.16 Thus, ideally, vaccines should be administered prior to planned immunosuppression as long as it is feasible.13 According to IDSA recommendations, PCV13 should be administered to newly diagnosed adults with hematological or solid malignancies and children with malignancies according to the following indications: Patients with primary complement deficiencies and who are (a) aged 2-5 years should receive 1 dose of PCV13 if they have received 3 doses of any PCV before age 24 months and 2 doses of PCV13 (8 weeks apart) if they have received an incomplete schedule of ≤2 doses of PCV7 (PCV7, PCV10 or PCV13) before age 24 months; (b) aged 6-18 years with a classic pathway (C1, C2, C3, C4), alternate pathway, or severe mannan-binding lectin (MBL) deficiency who have not received PCV13 should receive a single dose of PCV13 and (c) aged ≥19 years with a classic pathway (C1, C2, C3. C4). Alternate pathway, or severe MBL deficiency that are PCV13 naïve, should receive a single dose of PCV13. For those who received PPV23, PCV13 should be administered ≥1 year after the last PPV23 dose.13
Limitations of the study include a small number of patients and lack of information on baseline characteristics like neutropenia, clinical features and case-fatality rate, particularly important is the lack of information regarding the vaccine status at the time of infection.
It has been found that the administration of inappropriate initial empirical antibiotic therapy is a risk factor associated with mortality in patients with solid tumors, suggesting a prompt identification and knowledge of antimicrobial susceptibility patterns can influence patient outcome. In this study, antimicrobial susceptibility to penicillin and cefotaxime decreased in the post-PCV7 period, erythromycin resistance was above 30% in both periods. Empirical treatment with third generation cephalosporin may decrease the risk of treatment failures due to beta-lactam resistance, but local susceptibility patterns must be available to improve empirical treatments. Efforts should be made to reinforce surveillance and increase vaccination coverage in adults, particularly in oncology patients.

