











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroducción
In 2012, 21% of the global population aged 15 and above smoked tobacco. Men smoked at five times the rate of women; the average rates were 36 and 7%, respectively. Although Caribbean countries are generally below this global average, the region is dominated by small island developing states with limited absolute resources to counter tobacco advertising, promotion and sponsorship. These economic vulnerabilities increase the importance of implementing the World Health Organization Framework Convention on Tobacco Control (WHO-FCTC), and monitoring the effects of these implementation efforts becomes a regional imperative.
Tobacco is a major driver of chronic disease, and is therefore a key target for interventions to limit smoking prevalence and cigarette consumption. Globally, commonly adopted interventions include cigarette taxation, and bans on tobacco advertising, sales to minors, and smoking in public places. In response to the global extent of tobacco use, WHO-FCTC came into force in 2005.1 The WHO-FCTC is a legally binding treaty in which nation states commit to the development and implementation of a series of evidence-based tobacco control measures. As of 2013, the WHO-FCTC had been ratified by 177 countries globally, including 14 countries in the Caribbean. 2 To assist countries to fulfil their WHO-FCTC obligations, in 2008 the WHO introduced a package of six tobacco control measures to reduce tobacco use (the MPOWER initiative). A key measure in this initiative is to establish monitoring on the magnitude, determinants and consequences of tobacco consumption, for national, regional, and global surveillance.3 These coordinated efforts are timely, with tobacco leading to an estimated 5.7 million deaths in 2010 and with one published scenario suggesting a rise to between 7.4 and 9.7 million deaths by 2030.4,5 The burden of tobacco use is also shifting towards developing economies, with tobacco-related deaths in developed economies projected to decline gently by 2030, but estimated to double in low and middle income countries.5
For much smoking-related chronic disease, the risk of onset increases with smoking duration and cumulative cigarette consumption.6 Therefore, developing a smoking dependency early in the life-course can adversely influence subsequent morbidity and mortality. Tobacco consumption often begins in adolescence. In the US, almost 90% of adults in the US who smoke on a daily basis tried their first cigarette during adolescence and before 18 years of age.6 In 1999, in response to a paucity of information on adolescent tobacco use, the WHO’s Tobacco Free Initiative (TFI), and the Centers for Disease Control and Prevention (CDC), and Office on Smoking and Health (OSH) developed the Global Youth Tobacco Survey (GYTS). In addition to prevalence, the GYTS survey instrument collects information of relevance to monitoring the success of a country’s tobacco control programme. The GYTS uses a standardized methodology allowing cross country and regional comparisons.7,8
In this report we provide baseline information on tobacco use among adolescents in the Caribbean for the period before country-level implementation of WHO-FCTC control efforts. Our analysis comprises three parts. First, we report baseline prevalence of tobacco use among adolescents, second, we report prevalence change over a short time period before implementation of MPOWER initiatives in the Caribbean, and third we report regional disparities in these baseline prevalence rates.
Materials and méthods
Survey methods
The GYTS uses a standardized survey methodology to facilitate cross-country comparisons. Each GYTS sample is selected using a two-stage cluster design (classes within schools), with schools selected using probability proportional to pupil enrolment numbers. Each survey collects tobacco related information from adolescents aged 13 to 15 years of age grouped into several information domains, including prevalence of tobacco use, perceptions and attitudes to tobacco use, access and availability of tobacco, tobacco in the school curriculum, media and advertising, and cessation. Each domain is seen as an important contributor to a comprehensive tobacco control program. Full details of survey methodology is available elsewhere.7
Defining the Caribbean
As acknowledged by Girvan,9 a definition for the Caribbean depends not only on geography, but also on historical and socio-political factors.9 The United Nations definition of the Caribbean includes 30 island territories in the Caribbean basin: 13 independent nations, two unincorporated US territories, five British overseas territories, four overseas French administrative divisions, and six countries or municipalities within the Kingdom of the Netherlands. Four additional territories have been added to this UN definition because of their strong historical and socio-political links to many of the Caribbean island states: Belize in Central America, and the Guianas in north-eastern South America consisting of Guyana, Suriname, and French Guiana, an overseas territory of France.10
Caribbean GYTS
Because we wanted to provide baseline information on adolescent smoking prior to country-level control efforts, we identified all Caribbean countries with GYTS surveys between 2000 and 2008. To report baseline prevalence and prevalence change over time we restricted countries to those with two GYTS surveys during this time frame. From 30 Caribbean territories, 10 have not conducted a GYTS survey, four have performed one GYTS survey, one has performed two GYTS surveys with only one between 2000 and 2008, and one has performed two GYTS surveys between 2000 and 2008 but has no publically available data. This leaves information on 14 countries with GYTS surveys included in this report. Details of included and excluded countries, along with GYTS survey years, number of participants and response rates are presented in table I We used two survey questions to describe tobacco use: “Have you ever tried or experimented with cigarette smoking: even one or two puffs?” (ever smoked) and “During the past 30 days (one month), one how many days did you smoke cigarettes?” (identified as a current smoker if participant smoked on one or more days in previous month).
Table I Countries and territories included in a definition of the Caribbean with at least two Global Youth Tobacco Surveys (GYTS) between 2000 and 2008, year of survey,grouped into rounds one or two, and response rate for each round
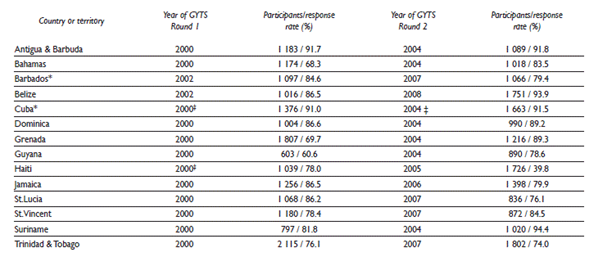
The following countries and territories have not performed a GYTS survey: Anguilla, Aruba, Caribbean Netherlands (refers to Bonaire, Saba, and Sint Eustatius), Cayman Islands, Curaçao, French Guiana, Guadeloupe (includes Saint-Barthélemy and Saint-Martin), Martinique, Sint Maarten, Turks and Caicos Islands
The following countries and territories have performed one GYTS survey: Dominican Republic (2004), Montserrat (2000), British Virgin Islands (2001), Puerto Rico
The following countries have performed two GYTS surveys, with one between 2000 and 2008: St Kitts & Nevis (2002, 2010)
The following countries and territories have performed two GYTS surveys between 2000 and 2008 but have no publically available data: United States Virgin Islands
* Also had survey in 1999
‡ Haiti GYTS 2000 sampled schools in Port-au-Prince only. Cuba GYTS 2000 and 2004 sampled schools in Havana only
n/a Data or results not yet publically available
Measuring disparities
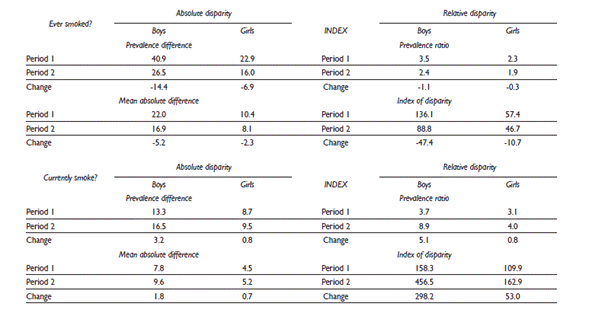
There are many potential disparity measures, and the properties of some of these measures have been summarized in recent reviews.11,12,13 This analysis follows current pragmatic advice, presented for cancer disparity research but broadly applicable, to present a suite of disparity measures encompassing both absolute and relative measures.11 Details of the health disparity measures used in this analysis are provided in Hambleton and colleages.14 Briefly, four disparity measures are presented: two absolute and two relative measures of disparity, with two measures considered ‘simple’ (comparing the two countries with the best and worst prevalence rates) and two considered ‘complex’ (comparing prevalence rates in all countries against a chosen comparator) according to an informal WHO classification.13 The prevalence difference (PD) is a simple absolute disparity measure. It is the arithmetic difference between the two Caribbean countries with the highest and lowest smoking prevalence rate; in other words, it reports the absolute disparity range. The prevalence ratio (PR) is a simple relative disparity measure. It divides the Caribbean country with the best (lowest) prevalence rate by that with the worst (highest) prevalence in each time period; in other words it reports the relative disparity range. Both measures are easy to interpret but ignore the experience of the “non-extreme” Caribbean countries. The absolute mean difference (MD) is an absolute disparity measure. For each Caribbean country it calculates the difference of its prevalence rate from the regional average, adds these differences together and divides by the number of countries. So MD considers all countries in the assessment group. The index of disparity (ID)15 is a relative disparity measure. It is the absolute mean difference, expressed as a percentage of the reference country. For PD, MD, and ID zero means perfect equity (all countries with the same prevalence rate) and for PR one means equity. For all measures, larger positive values indicate increasing smoking rate disparity. Although not guaranteed, consensus across the suite of disparity measures would offer consistent evidence for a particular disparity trend. All measures are appropriate when there is no implicit ordering in the groups being compared, as is the case when comparing countries or world regions.
Statistical methods
In table II, we present prevalence rates for our two survey questions (ever smoke, currently smoke) stratified by country, by survey round and by gender, adjusting for survey design at all times. The number of years between surveys varied from four years to seven years, and we standardized the prevalence change between rounds to be the 5-year change since round one. We then visualized these prevalence rates for boys (figure 1) and girls (figure 2). For this visualization, we present ordered plots of lowest to highest tobacco-use prevalence in survey period one for each country (with 95% confidence intervals) for ever smoked tobacco (figures 1A and 2A) and for currently smoke (figures 1B and 2B). We plotted the joint change in ever smoke and currently smoke prevalence rates between survey round one and survey round two as a scatterplot in figures 1C and 2C. This scatterplot has been divided into four quadrants for interpretation. Countries in the lower-left quadrant have seen a 5-year drop in the prevalence of adolescents reporting that they have “ever-smoked” and “currently smoke” cigarettes (green points). Countries in the upperright quadrant have seen a rise in both prevalence rates (red points), with the remaining two quadrants seeing either a rise in the prevalence of “ever-smoked” or “currently smoke”, but not both. We report the statistical significance associated with the 5-year prevalence change of “ever-smoked” and “currently smoke” by country and gender using a univariate test of proportions. With two types of prevalence rate among 14 countries for boys and girls, this creates 60 separate univariate tests of significance, and we control for the possibility of false positive statistical significance using the Šidák inequality. 16 Using this adjustment for multiple testing, we must achieve a p-value of 0.00085 or smaller to achieve statistical significance at the 5% level. Last, our four health disparity metrics were calculated: two absolute measures (PD, MD) and two relative measures (PR, ID) and reported separately for boys and girls. All analyses were performed using Stata statistical software.(a)
Table II Prevalence of students aged 13-15 years who used tobacc o during two rounds of the Global Youth Tobacc o Survey in the Caribbean, 2000-2008
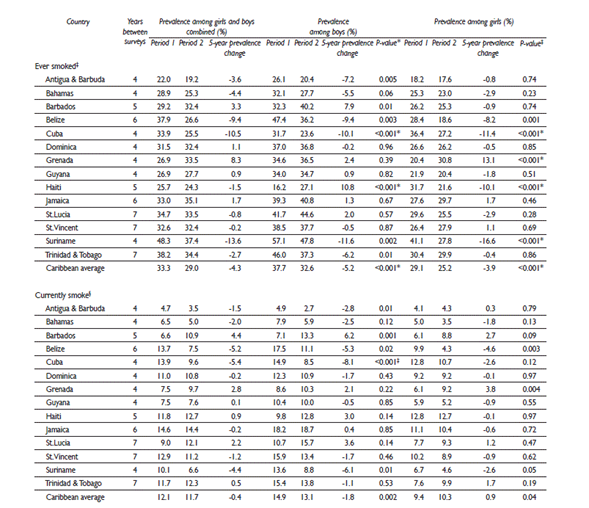
* P Values. After adjustment for multiple testing, a p-value of 0.00085 or smaller must be achieved for statistical significance at the 5% level
‡ Ever-Smoked. Survey question: “Have you ever tried or experimented with cigarette smoking: even one or two puffs?”
§ Currently smoke. Survey question: “During the past 30 days (one month), one how many days did you smoke cigarettes?” (identified as a current smoker if participant smoked on 1 or more days in previous month)
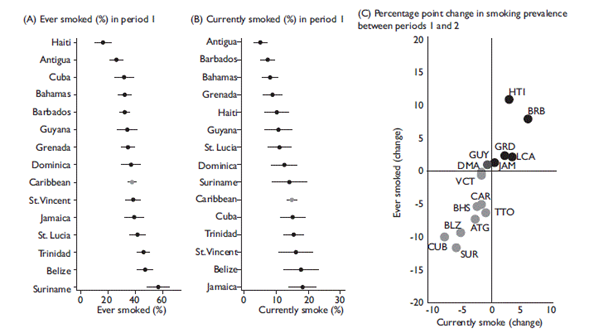
Note: UN 3 digit country codes are used to highlight country prevalence change between periods 1 and 2. ATG= Antigua & Barbuda, BHS= Bahamas, BRB= Barbados, BLZ= Belize, CUB= Cuba, DMA= Dominica, GRD= Grenada, GUY= Guyana, HTI= Haiti, JAM= Jamaica, LCA= St. Lucia, VCT= St. Vincent & the Grenadines, SUR= Suriname, TTO= Trinidad & Tobago, CAR= Caribbean region
Figure 1 Smoking prevalence during survey round 1 among boys aged 13-15 years, measured using two indicators (ever smoked, even one or two puffs, and currently smoke) and the joint change in smoking prevalence between survey rounds 1 and 2, among 14 Caribbean nations during two succ essive Global Youth Tobacc o Surveys (2000-2008)

Note: UN 3 digit country codes are used to highlight country prevalence change between periods 1 and 2. ATG= Antigua & Barbuda, BHS= Bahamas, BRB= Barbados, BLZ= Belize, CUB= Cuba, DMA= Dominica, GRD= Grenada, GUY= Guyana, HTI= Haiti, JAM= Jamaica, LCA= St. Lucia, VCT= St. Vincent & the Grenadines, SUR= Suriname, TTO= Trinidad & Tobago, CAR= Caribbean region
Figure 2 Smoking prevalence during survey round 1 among girls aged 13-15 years, measured using two indicators (ever smoked, even one or two puffs, and currently smoke) and the joint change in smoking prevalence between survey rounds 1 and 2, among 14 Caribbean nations during two succ essive Global Youth Tobacc o Surveys.
Results
Survey details
We included 28 surveys from 14 countries. The total number of participants was 16 715 in survey round one and 17 337 in survey round two. Country response rates varied between 60.6% and 91.7% in round one (with a median response rate of 83.2%) and between 39.8 and 94.4% in round two (with a median response rate of 84.0%). The number of participants and country response rates are presented in table I.
Prevalence: ever smoked cigarettes
The Caribbean prevalence of ever-smoked cigarettes fell from 33.3% in survey round one to 29.0% in survey round two (37.7 to 32.6% in boys, 29.1 to 25.2% in girls) (table II). Among boys in survey round one, Haiti reported the lowest prevalence of 16.2% (95%CI 11.2 to 23.0%) and Suriname reported the highest prevalence of 57.2% (95%CI 48.4 to 65.4%) (figure 1A). The Caribbean 5-year prevalence change in boys was a 5.2 percentage point decrease, and ranged from an 11.6 percentage point decrease (Suriname) to a 10.8 percentage point increase (Haiti), with 8 of 14 countries reporting a 5-year decrease. After adjustment for multiple testing, two countries (Cuba and Suriname) have seen a statistically significant decrease in the proportion of boys reporting that they have ever-smoked cigarettes (p<0.001 in each case). Among girls in survey round one, Antigua reported the lowest prevalence of 18.2% (95% CI 14.7 to 22.3%) and Suriname reported the highest prevalence of 41.1% (95% CI 35.5 to 46.9%) (figure 2A). The Caribbean countries have seen a statistically significant decrease (Cuba, Suriname and Haiti) and one has seen a statistically significant increase (Grenada) in the proportion of girls reporting that they have ever-smoked cigarettes (p<0.001 in each case).
Prevalence: current cigarette smoking
The Caribbean prevalence of currently-smoke cigarettes fell from 12.1% in survey round one to 11.7% in survey round two (falling from 14.9 to 13.1% in boys, rising from 9.4 to 10.3% in girls) (table II). Among boys in survey round one, Antigua reported the lowest prevalence of 4.9% (95%CI 3.2 to 7.5%) and Jamaica reported the highest prevalence of 18.2% (95%CI 14.3 to 22.9%) (figure 1B). The Caribbean 5-year prevalence change in boys was a 1.8 percentage point decrease, and ranged from an 8.1 percentage point decrease (Cuba) to a 6.2 percentage point increase (Barbados), with 9 of 14 countries reporting a 5-year decrease. After adjustment for multiple testing, one country (Cuba) has seen 5-year prevalence change in girls was a 3.9 percentage point decrease, and ranged from a 16.6 percentage point decrease (Suriname) to a 13.1 percentage point increase (Grenada), with 9 of 14 countries reporting a 5-year decrease. After adjustment for multiple testing, three statistically significant decrease in the proportion of boys reporting that they currently smoke (p<0.001). Among girls in survey round one, Antigua reported the lowest prevalence of 4.1% (95% CI 2.5 to 6.5%) and Cuba and Haiti reported the joint highest prevalence of 12.8% (Cuba 95%CI 9.7 to 16.8%, Haiti 95%CI 7.9 to 20.1%) (figure 2B). The Caribbean 5-year prevalence change in girls was a 0.9 percentage point increase, and ranged from a 4.6 percentage point decrease (Belize) to a 3.8 percentage point increase (Grenada), with 9 of 14 countries reporting a 5-year decrease. After adjustment for multiple testing, no countries report a statistically significant change in the proportion of girls reporting that they currently smoke.
Prevalence: joint 5-year change in ever smoked and currently smoke
The joint 5-year change in the prevalence of ever-smoked and currently smoke is graphed in figure 1C for boys and in figure 2C for girls. Among boys, eight countries reported a joint 5-year decrease in ever-smoke and currently-smoke, and five countries reported a joint increase in these prevalence rates (figure 1C). This figure highlights those countries with larger joint prevalence decreases (Cuba, Suriname, Belize) and those with larger joint prevalence increases (Haiti, Barbados). Among girls, seven countries reported a joint 5-year decrease in eversmoke and currently-smoke, and one country reported a joint increase in these prevalence rates (figure 2C). This figure highlights those countries with larger joint prevalence decreases (Cuba, Suriname, Belize) and one country with a large joint prevalence increase (Grenada).
Prevalence: between-country disparities
Considering boys and girls separately, between-country disparities among adolescents that have ever smoked have decreased while disparities among current smokers saw little change (table III). In boys ever-smoked absolute disparity metrics dropped by 14.4 percentage points (PD) and 5.2 percentage points (MD), and currently smoke absolute disparity metrics increased by 3.2 percentage points (PD) and 1.8 percentage points (MD). In girls ever-smoked absolute disparity metrics dropped by 6.9 percentage points (PD) and 2.3 percentage points (MD), and currently smoke absolute disparity metrics increased by 0.8 percentage points (PD) and 0.7 percentage points (MD).
Discussion
Adolescent smoking: prevalence in the Caribbean
In Caribbean adolescents, there were modest reductions in the prevalence of ever-smoked cigarettes and of current smokers over a 5-year period. Overall, the prevalence of ever-smoked cigarettes fell from 33.3 to 29.0%, and the prevalence of current smokers fell slightly from 12.1 to 11.7%. Considering the countries and territories individually, statistically significant decreases in “ever-smoked” were seen for both boys and girls in Cuba and Suriname, and for girls in Haiti. Only one country (Cuba) saw a statistically significant decrease in current smoking in boys. This minimal progress in tobacco smoking reduction is not surprising, as the period considered was relatively short, and preceded the ratification of the WHO-FCTC and implementation of MPOWER initiatives in the Caribbean. Therefore, these rates should be interpreted as a baseline for subsequent Caribbean monitoring of adolescent tobacco use.
Adolescent smoking: Caribbean prevalence in context
Presenting median Caribbean smoking rates for boys and girls together allows a direct comparison with published global rates.7 For survey round one (years 2000-2002) and two (years 2004-2007) regional rates were 32.1 and 32.4% for “ever smoked” and 10.6 and 10.3% for “currently smoke”. Global rates between 1999 and 2001 were 33.0% for “ever smoked” and 13.9% for currently smoke. The proportion of Caribbean adolescents who had ever tried tobacco matched the global average, while the proportion of current smokers was slightly below the global average. Recognising within-region variation, nine out of 14 Caribbean countries were at or lower than the global average (ever smoked) while 13 out of 14 were at or lower than the global average for current smokers.
Adolescent smoking: between-country disparities in the Caribbean
Between-country disparities in “ever-smoked” reduced over the 5-year assessment interval. In boys absolute disparity metrics decreased by 14.4 percentage points (PD) and by 5.2 percentage points (MD), and in girls absolute disparity metrics decreased by 6.9 percentage points (PD) and by 2.3 percentage points (MD). These decreases were primarily due to large 5-year prevalence rate decreases among three countries with initially high rates for either boys, or girls or both (Suriname, Cuba, Belize). There was little change in between-country disparities among current smokers. The Declaration of Port-of-Spain, issued in 2007, calls for unity amongst Caribbean Community member states in the response to non-communicable diseases (NCDs). The persistent adolescent smoking differences between Caribbean countries complicates the regional commitment to a coordinated public-health response, reminding us that public health interventions should be tailored to individual countries to be most effective.17,18 These baseline disparities were examined over a short time period and were relatively small in many countries, and should be viewed as initial values for the purpose of future monitoring.
WHO-FCTC in the Caribbean
The WHO-FCTC was introduced in 2005 and the associated MPOWER toolkit for implementation was launched three years later. In the Caribbean, two rounds of GYTS were conducted prior to launch of the MPOWER initiative. Of the fourteen countries who had two surveys in this pre-MPOWER period (2008 or earlier), ten had signed and ratified the WHO-FCTC between the two survey rounds, two countries ratified post-2008 (Bahamas, Saint Vincent & the Grenadines), and two countries had signed but not ratified the WHO-FCTC (Haiti, Cuba). It is now a decade since the launch of the WHO-FCTC and more than half of the world’s countries have implemented at least one MPOWER measure at the highest level of achievement.19 By region, South and Central America have the highest proportion of countries with at least one MPOWER implantation (17 out of 19 countries, 89%), followed by Europe (39 out of 53 countries, 74%), Western Pacific (20 out of 27.74%), Eastern Mediterranean (13 out of 23.57%), South-East Asia (6 out of 11.55%), Africa (14 out of 47.30%), and the Caribbean (4 out of 16.25%). In the Caribbean, Barbados, Jamaica, Trinidad & Tobago, and Suriname have implemented smoke-free public places. Additionally, Jamaica has implemented warnings on cigarette packaging, and Suriname has implemented a ban on tobacco advertising. Further GYTS monitoring is planned for the Caribbean, and Caribbean MPOWER initiatives are critical to accompany the substantial regional monitoring efforts.
Data limitations
The GYTS survey provides a standardized regimen for data collection and processing. Nevertheless, variations between country data collection effort inevitably exist and this is partly reflected in survey response rates, which vary from 60.6 to 91.7% in survey round one (median 83.2%) and from between 39.8 to 94.4% in round two (median 84.0%). Moreover, in population surveys such as the GYTS, self-reported data are typically used to monitor population trends in cigarette smoking, and are subject to reporting biases.20,21 Objective assessment of smoking status for current smokers exists, with urinary cotinine suggesting generally higher prevalence than self-report,22 but with the extent of the difference varying by country.23 Nevertheless, for much of the world, with limited absolute resources to monitor a range of disease risk factors and outcomes, tobacco use self-report -even if conservatively underestimating- represents a pragmatic data collection option for monitoring through time.
Conclusions
The GYTS remains the single source of adolescent smoking, continues to be conducted regularly throughout the Caribbean, and is the key data source for regional monitoring of adolescent tobacco use. This national and regional summary of GYTS tobacco use provides baseline estimates of adolescent smoking, and crosscountry disparities in smoking for the period before country-level implementation of MPOWER. Information generated from subsequent GYTS survey rounds can be can be used to stimulate the development of tobacco control programs and to subsequently monitor program success.

