











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Children with disabilities are among the most vulnerable members of any society. A disability may occur due to a genetic condition, serious injury, nutritional deficiency, infection or exposure to environmental toxins.1 Child disabilities, or developmental disabilities, are limitations in mental, social, and/or physical function relative to age-specific norms.2
Challenges in producing reliable and comparable disability data are well documented, mostly due to a lack of consistent definitions and indicators along major differences in the study designs and methodologies.3,4 In general, disability data gathered through censuses and household national surveys has been found to under-enumerate disabled subjects.5 In addition, there is agreement among experts that measuring disability among children is particularly complicated given the developmental processes that occur at such young age that are inherent to normal child function limitations (e.g., independent washing, dressing).4 The lack of reliable and representative national and global estimates has contributed to a lack of visibility of the needs of the disabled population and to an absence of evidence for legislation and policy-making.2
According to the World Health Survey from WHO, around 785 million (15.6%) persons 15-years and older live with disability.6 The Global Burden of Disease estimates 975 million persons (19.4 %).7 The Global Burden of Disease measures children’s disabilities from 0 to 14 years, estimating that 95 million children (5.1%) live with disabilities, of whom 13 million (0.7%) live with severe disability.4 Results from the World Health Survey indicate higher disability prevalence in lower income countries as compared to higher income countries. People from the poorest wealth quintile have a higher prevalence of disability.3 Data from the Multiple Indicator Cluster Surveys (MICS) show that children from poorer households and those in ethnic minority groups are at higher risk of disability than other children.1
Despite growing interest about this subject, both at academic8 and policy level, data about disability among young children in Mexico is scarce. Previous official reports based on the last Population Census indicated that less than 1% of 0 to 4 year-old children had a disability.9 More recent estimates from the last Demographic Dynamic National Survey results (ENADID 2014), indicate that 1.9% of children under 18 years had a disability and 4.8% had a functioning difficulty.10
Generating population data on the magnitude of disability among Mexican children is crucial, as well as understanding its socio-demographic trends and association with other health and wellbeing outcomes such as nutritional status, immunization coverage, disease prevalence and violent discipline. The Mexican National Survey of Children and Women (ENIM 2015) represented the first effort to gather reliable, standardized comparable data on a wealth of indicators, which cover multiple domains of children and women health and wellbeing.11
This study aimed to (1) report the prevalence of severe child functioning difficulties and disability (CFD) among two to four year-old children in Mexico; (2) identify factors associated with severe CFD; and (3) document how discrete population profiles predict severe CFD.
Materials and methods
This analysis was performed based on the ENIM 2015, a survey implemented in 2015, as part of round 5 of the Multiple Indicator Cluster Surveys (MICS 5). The ENIM 2015 methodology can be found elsewhere.11 Briefly, the ENIM 2015 was a multistage, stratified and clustered national survey, designed to estimate indicators for children and women. The survey is representative of rural and urban areas as well as of five geographical regions: Northwest, Northeast, Central, Mexico City-State of Mexico and South. An oversampling of households with children under five years and homes in rural areas was obtained to generate a sufficient sample size of children under five years and indigenous population.
Four questionnaires were applied using tablets: 1) household questionnaire, 2) a questionnaire for women aged 15 to 49, 3) a questionnaire for children and adolescents aged 5-17 years answered by their mothers, and 4) a questionnaire for children under five years old, answered by their mothers. The questionnaire for children under five years-old included modules of: birth registration, Early Childhood Development, lactation and food intake, vaccination, disease care, functioning and disability in children (two to four years), anthropometry, and hemoglobin.
Variables
Severe child functioning difficulties and disability was measured using the UNICEF-Washington Group module on CFD,12 based on the World Health Organization International Classification of Functioning, Disability, and Health (ICF). The WG module was designed to identify those who are at greater risk than the general population for participation restrictions because of the presence of difficulties in core domains. The response categories introduce a scale to capture the level of difficulty experienced including no difficulty, some difficulty, a lot of difficulty (severe), or cannot do at all (very severe). The indicator used in our analysis identifies children presenting severe functioning difficulties in at least one of the following domains: seeing, hearing, walking, fine motor coordination, understanding, being understood, learning things, or playing, or, in the case of controlling behavior, very severe difficulties (i.e. having much more difficulties controlling their behavior than other children of the same age).
To define stunting, height was measured by trained nurses, using UNICEF portable child height measuring board made of wood, and standardized to a height-for-age ratio or z-score. Height-for-age z-scores were grouped based on standard deviations from the international reference population median. In this case stunting was define as those with height-for-age z-scores two or more standard deviations below the reference population median. 1
Body weight was measured by trained nurses using SECA-874U electronic scale for weighing. Underweight was evaluated by creating standardized weight-for-age ratios (z-scores). Underweight was defined as those at least two standard deviations below the median. 1
The wealth index is a composite indicator of wealth calculated using principal components analysis. To obtain this index, we use information on the ownership of consumer goods, dwelling characteristics, water and sanitation, and other characteristics related to the household’s wealth such as inhabitants per bedroom, having a bank account and home and land ownership, to generate factor scores for each of the items used. We first calculate initial factor scores for the total sample. Then, we calculated separate factor scores for households in urban and rural areas. Finally, we regress the urban and rural factor scores on the initial factor scores to obtain the combined final factor scores for the total sample. This is carried out to minimize the urban bias in the wealth index values. Each household in the total sample is then assigned a wealth score based on the assets owned by that household and on the final factor scores obtained as described above. The survey household population is then ranked according to the wealth score of the household they are living in, and is finally divided into 5 equal parts (quintiles) from the lowest (poorest) to highest (richest).
The head of household’s was classified as indigenous, if he or she speake an indigenous language. Children who experienced any physical punishment during the previous month of the survey were classified as having physical child discipline. Any psychological aggression to the child during the last month was considered as psychological child discipline.
Data analysis
We present prevalence and 95% confidence intervals, the magnitude of association between CFD and the main characteristics of the household, mothers and children. Using a multivariate logistic model, we estimated the odds of presenting CFD for the three socio-demographic predictors found to be significant in the previous analysis: sex, poor households and no maternal formal education. We then generated profiles based on combinations of the socio-demographic factors found to be significant in the logistic regression model best predicted CFD. For this, we used post-estimation exploration to interpret the logistic model by computing predicted probabilities of presenting CFD based on discrete combinations of socio-demographic profiles.13 Finally, we present the increase in probabilities according to the different profiles. For all the statistical analysis we took into account the complex sample design and used the survey sample weights. Data analysis was implemented in Stata 13.0 (College Station, TX).
The ENIM 2015 protocol was approved by the INSP’s research, ethics and biosafety committees. Informants were asked for informed consent.
Results
We analyzed data from 5 010 children two to four year-old participating in the ENIM 2015, of whom, 52.4% were girls, 92% lived in a non-indigenous household, 47% lived in a poor household, and 76% in urban communities (table I)
Table I Demographic and household characteristics of children two to four years old. México, ENIM 2015
* Includes: 3 dose of Hepatitis B, 3 dose of pentavalent (Poliovirus, Haemophilus influenzae type b, Diphtheria, tetanus, and acellular pertussis) one dose of BCG, two dose of Rotavirus, and two dose of Pneumococcal
ENIM: National Survey of Children and Women
Table II shows the prevalence of severe functioning difficulties or disabilities by domain. The most common difficulties or disabilities were: getting to be understood (0.9%), walking (0.3%), understanding (0.3%), and learning things (0.3%). All of the difficulties or disabilities were more prevalent among boys than girls, except for seeing which was higher in girls (0.2%) than in boys (0.1%). The percentage of children with severe functioning difficulties in at least one domain was 2% for all children, 2.5% in boys and 1.5% in girls.
Table II Children two to four years old with severe functioning difficulties or disabilities in any of the domains. México, ENIM 2015
ENIM: National Survey of Children and Women
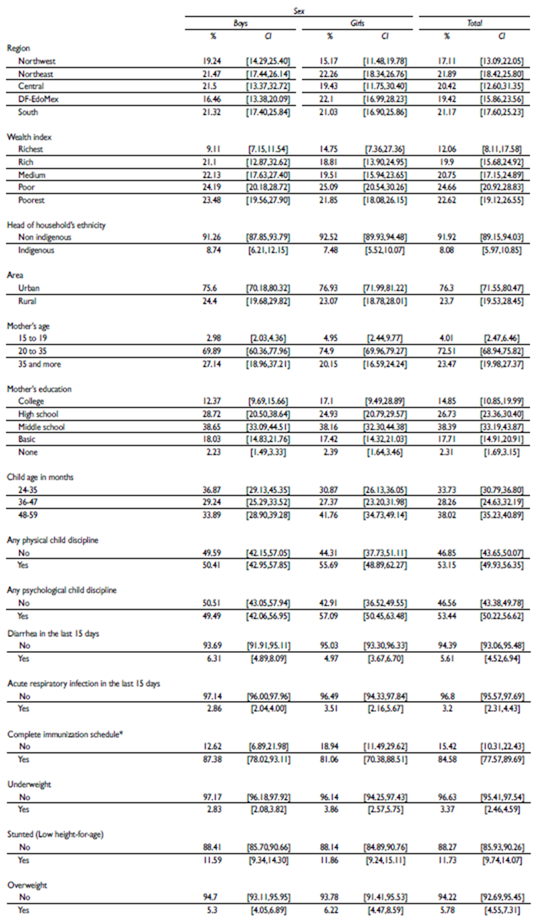
Table III shows the prevalence and the magnitude of associations between having at least one severe functioning difficulty or disability and the main demographic, household and characteristics of children two to four years old. Child disability is more prevalent among the poorest (3%) than the richest (0.7%), and among children of a mother with no education (8.3%) than of mothers with a college education (1%). The percentage of children with at least one severe functioning difficulty or disability is highest among children who are stunted (low height-for-age) (2.2%), underweight (6.2%), received physical punishment discipline (2.5%), and presented diarrhea in the previous 15 days (4.7%). Data from this survey does not allow to show differences within the categories of other variables.
Table III Prevalence and relation between having at least one severe functioning difficulty or disability and demographic, household and characteristics of children two to four years old. México, ENIM 2015
* Includes: three dose of Hepatitis B, three dose of pentavalent (Poliovirus, Haemophilus influenzae type b, Diphtheria, tetanus, and acellular pertussis) one dose of BCG, two dose of Rotavirus, and two dose of Pneumococcal
ENIM: National Survey of Children and Women
Results indicate that boys are 75% more likely than girls to present at least one severe functioning difficulties and disability. Children in the poorest households are five times more likely to present severe functioning difficulties or disability (OR=4.57 95%CI: 1.56-13.44). Children of women with no formal education are nine times more likely to present severe functioning difficulties or disability (OR=9.17 95%CI: 2.20-38.17). Underweight was also significantly associated with CFD (OR=1.01 95%CI: 1.01-1.02). Children living in households with reported use of violent child discipline were also more likely to present severe function difficulties and disability (OR=1.01 95%CI: 1.001-1.01) (table III).
Table IV presents the adjusted odds ratio of presenting at least one severe CFD for the three socio-demographic predictors. Boys are 72% more likely than girls of presenting severe CFD (OR:1.72 95%CI 1.07-2.74). Children living in households in wealth quintiles 1,2 or 3 and children whose mothers have primary education or lower, are nearly twice as likely of presenting severe CFD when compared with richer children, and children of women with higher education levels (OR:1.94; 95%CI 1.06-3.51 and OR:1.95; 95%CI 1.17-3.24, respectively).
Table IV Adjusted odds ratio for CFD. México, ENIM 2015
CFD: severe child functioning difficulties and disability
ENIM: National Survey of Children and Women
The conditional probability of presenting severe CFD according to the explored profiles ranged from 2.21 for children in wealth quintiles 1, 2 or 3, to 4.64% for boys in wealth quintiles 1, 2 or 3, whose mother has only primary level or less education (figure 1).
Discussion
Results from this nationally representative survey provide evidence that 2% of two to four year old children in Mexico present severe CFD. CFD is more frequent in boys, in children living in the poorest households, and those whose mother had low or no formal education. Severe functioning difficulty or disability in children was also significantly associated with underweight, and with violent discipline reported within the household.
Mexico was one of the first countries to include the UNICEF-WG module on CFD in a population survey. Thus, the collected data cannot be directly compared to other surveys using the same methodology. Previous evidence from rounds 3 and 4 of MICS survey, using the 10 Questions Questionnaire,14 a child disability screening tool that focuses on children at risk of disability, showed that family wealth or poverty is linked to higher risk of child disability. MICS3 surveys found percentages of children with risk of disability were higher among those in the poorer 60% of the households in 12 of 18 countries. In Bangladesh, Georgia, Mongolia, Serbia, Sierra Leone and Thailand, the odds of risk of disability were statistically significantly higher among those in the poorest 60% of households compared to the wealthiest 40%. Low household income may imply conditions that can lead to the development of child disability. Additionally, family wealth might determine access to health care facilities and therefore access to preventive or treatment services.1 MICS3 results also showed an association between risk of disability and malnutrition.1 In several countries participating in the MICS3, questions regarding discipline of children, including physical discipline, were included. Children with disability were significantly more likely to receive severe physical punishment in seven of the 15 countries (Albania, Belize, Cameroon, Central African Republic, Ghana, Mongolia, and Sierra Leone).1 Results for Mexican population of two to five year old children, using the same screening approach, showed higher prevalence of risk of disability risk among boys when compared to girls.15
Our study has some important strengths and limitations. Disability measurement at the population level is challenging due to the lack of consistent definitions and harmonized data collection methodologies,4 often resulting in bias by low sensitivity and underreporting.16 In recent years, there has been a call at the global and regional levels for the adoption of a standardized and comparable definition of disability that enables the estimation of population prevalence and disaggregation according to key characteristics.6,17 In order to improve the quality and international comparability of disability measures, the United Nations commissioned the Washington Group on Disability Statistics (WG) to develop an instrument suitable for censuses and national surveys. The WG developed a short questionnaire that includes six core functioning domains: seeing, hearing, walking, cognition, self-care and communication. Since 2009 the WG developed a specific instrument for measuring disability in children. In 2011 UNICEF and WG in conjunction reviewed and developed a disability module that would apply in MICS.12 The module is intended to provide an estimate of the number and proportion of children with functioning difficulties. These difficulties may place children at risk of experiencing limited participation in an unaccommodating environment. The survey module covers children between two and 17 years of age and assesses functioning difficulties in the domains of speech and language, hearing, vision, learning, mobility and motor skills, and emotions. The primary purpose is to identify the sub-population of children that are at greater risk than children of the same age of experiencing limited social participation due to functioning limitations.12
The increased recognition of functioning difficulties and disability as public health problems require the implementation of scalable and efficient population screening instruments aligned with the framework of the new Sustainable Development Goals. The identification of the population with functioning difficulties and of the sub-groups at increased risk provides useful information for policy formulation and implementation of targeted efforts. Our results show that the probability of presenting CFD increases dramatically in specific sub-groups of the population. In particular, males, children of women with low or no formal education, and those who live in the poorest households, present a two-fold higher probability of presenting severe functioning difficulties.

