











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
According to projections of the World Health Organization (WHO), by the year 2050 it is estimated that the number of older adults (OA) aged 60 years + will represent 22% of the world population1 and 28% of the Mexican one.2 This demographical change will bring an increase in non-communicable chronic diseases (NCDs) as well as geriatric syndromes in OA.3
In addition, OA population frequently have malnourishment problems due to the physiological changes that take place during the aging process4 (edentulism, gastric achlorhydria, malabsorption, etc.), as well as psychological (cognitive decline and depression) and social aspects (poverty and loneliness),5 resulting in an inadequate intake of essential micronutrients (folates, vitamin B12, retinol, iron), which in turn affect their physical and mental performance.4 In Mexico, there is scarce literature that documents the dietary intake of OA. The internal evaluation of the 70 y más program documented a median energy intake of 1 259.14 kcal in OA residing in rural areas, based on food staples (corn, bread) with little variety of other foods, such as fruits and vegetables and animal products.6 The monotony of the diet, combined with physiological changes, partly explains the high prevalence of low weight (6.9%) and the high proportion of OA with a decreased muscle mass (40%) in later ages,7 which puts them in a higher risk for sarcopenia.8These conditions place OA in a state of greater vulnerability and detrimental health, affecting their quality of life.
Given the fundamental role of nutrition in these stages, it is of interest to know the dietary intake of this population. The objective of this study is to describe the intake, adequacy and inadequacy of energy, macro- and micronutrients of the diet in Mexican Older Adults aged 60 and older, participating in the 2006 and 2012 Ensanut (National Health and Nutrition Survey).
Materials and methods
Design and study population
Adults aged 60 years and older, participants from two Mexican National Health and Nutrition Surveys (Ensanut) were studied. The sample of OA 2006 (n=3 470) and 2012 (n=526), represented 9 506 100 OA in 2006 and 12 293 100 OA in 2012. Both surveys were conducted at a national level with a probabilistic design and representing urban and rural areas, as well as every state in the country. The sample design of both surveys has already been published.9,10
Description of variables
The semiquantitative food frequency questionnaire. Dietary data concerning the seven days prior to the interview were collected by qualified and standardized personnel through the semiquantitative food frequency questionnaire (SFFQ), which consists of a closed list of foods for which a standard serving size was previously established. The data cleaning methodology for the 2006 Ensanut has already been published.11 The SFFQ used in 2012 is similar to the one used in 2006, but it has 39 extra foods; thus, information was obtained for 140 foods and drinks, classified in 14 food groups.
Intake. In order to process the dietary information, the amount of each food and drink was obtained by multiplying the number of days, times per day, serving size (g, ml) and number of portions consumed in each meal. The total g and ml were divided by seven days to obtain the daily intake. The consumption of foods that were above three standard deviations (>3 SD) was eliminated.12 The nutritional contribution of the food was obtained using the nutritional composition table.
Intake adequacy percentages. The estimated energy requirement was calculated using the equations of the United States’ Institute of Medicine (IOM) for maintaining body mass considering a sedentary level of physical activity.13 For the adequacy of carbohydrates, 55% of the estimated average energy requirement was used as a reference; 30% for lipids, saturated fats (8%), trans fatty acids (TFA) (<2%) and sugar (<10%). Adequate intake was used for fiber.13 The WHO’s average requirement estimates were used for protein, calcium, vitamin A, vitamin C, vitamin D, vitamin B12, folate and zinc.14 For the adequacy of iron, the Mexican intake recommendations were used.15
Risk of intake inadequacy. The prevalence of the population under 100% of the adequate intake or requirement for each specified nutrient was estimated, except for sugar, cholesterol, saturated fats and TFA, whose values were classified as an excess. Given the low intake of TFA, no OA with inadequate intakes were observed (consumption >2%).
More details about the diet cleaning methodology, intake adequacy percentages values used as reference and implausible reporters in this group of population are published elsewhere.12
Nutritional status. The weight and height were obtained by standardized and trained personnel16 in adults who had no limitations for having their height and weight measured while standing. The weight was obtained using digital scales with 100g precision; the height was measured using a stadiometer with 1mm precision. The body mass index was generated (BMI=kg/m2) and classified according to the cutoff points proposed by the WHO.17 In those OA for whom we did not have anthropometric information, the weight and height were imputed through a regression model; in 205 cases (5.45%) for the 2006 Ensanut and in 63 (12%) for the 2012 Ensanut, to avoid a greater loss of information.
Area. A locality was classified as rural when the number of inhabitants was <2500 and as urban otherwise.
Geographical region. The country was divided into three geographical regions:9 Northern, Central and Southern. Mexico City was included in the Central region.
Indigenous population. The members of a household were classified as speakers of an indigenous language when this was stated by the head of the household and/or they considered themselves as being indigenous.
Household wealth index (HWI). This index was based on housing conditions, possession of goods, and the number of electrical appliances (the first component that accumulated 40.5% of the variability was chosen as an index).18 This index was considered as a proxy of the socioeconomic status, and it was classified in tertiles: low, middle and high.
Beneficiaries of social programs. Older adults were considered beneficiaries if they stated having received benefits from the Prospera program, the Program for the Social Distribution of Liconsa Milk (Programa de Abasto Social de Leche Liconsa, in Spanish) or the 70 y más program (for adults 70 and older).
Abdominal obesity. If the waist circumference was >80 cm in women and >90 cm in men.19
Education. The last grade of completed studies was considered, classifying them as: illiterate (non-education), elementary school, high school, and college/university.
Statistical analysis
The information is described as adjusted proportions and 95%CI for categorical data, and as adjusted medians, 25 and 75 percentile for the continuous variables, due to the biased distribution of intake and the adequacy of the reported nutrients.
A quantile regression model was used to estimate the adjusted data of intake and adequacy of energy and nutrients. Logistic regression models were used to estimate the risk of inadequacy for each nutrient. All models were adjusted by sex, age, BMI, geographical region and HWI for each survey. The statistical significance was set at α=0.05 and a confidence of 95%. The sensitivity of the model was tested where the prevalence of inadequacy of some nutrient was greater than 95% or less than 5%.
All estimations and analyses were adjusted by the sampling design of each survey, using the SVY module of STATA v13 (College Station, TX, USA).
Results
Descriptive characteristics
The characteristics of the OA participating in the 2006 and 2012 Ensanut surveys are described in table I.

Ensanut 2012
The median energy intake in the OA population was 1 500 kcals, with a median energy adequacy of 88%; 67% of OA had an inadequate energy intake. The median energy intake was higher in men when compared to women. No differences were observed in the percentage of energy inadequacy between men and women. For most of the nutrients, the median intake was lower in women, compared to men; no differences were observed in the median intake adequacy of such nutrients, with the exception of fiber and trans fatty acids, whose adequacy median was higher in women (and vitamin B12 was lower), when compared to men.
63.3% of the OA population exceeded the recommendation for saturated fat and 87.5% exceeded the recommendation for sugar. More than 80% did not cover the intake recommendations for polyunsaturated fatty acids, vitamin A, vitamin B12, vitamin D and calcium (table II). The proportion of OA that did not cover these requirements remained constant by sex, area and region, and it was more noticeable in OA from the lowest tertile of the HWI.
Table II Adjusted* nutrient intake, adequacy and percent of inadequacy intake (<100%) at the national level, by sex and by area. Mexico, Ensanut 2012
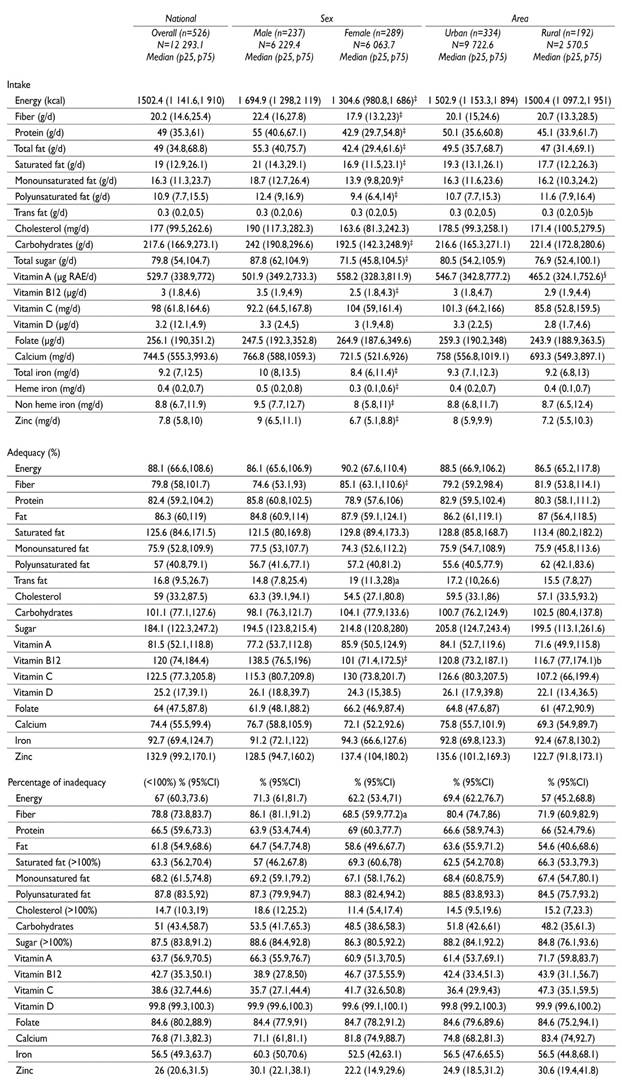
* Data are adjusted by sex, area, region, HWI and survey design using a quantil regression model
‡ Statistically different by sex (p<0.05)
§ Statistically different by area (p<0.05)
No statistical differences were observed in the median intake, energy adequacy and inadequacy, and macro- and most micronutrients in OA from the urban area vs rural; except for the intake of retinol and adequacy of vitamin B12. The proportion of OA with an inadequate intake of energy, macro- and micronutrients was not different by area (table II).
By geographical region, no differences were observed in intake, adequacy and inadequacy of energy. The intake and adequacy of cholesterol and the intake of heme iron were greater in the north, when compared to the center and south. The intake and adequacy of sugar was higher and the intake of vitamin A was lower in the center, compared to the south. The northern region had the lowest prevalence of sugar inadequacy, compared to the center. No differences were observed between regions, regarding the intake, adequacy and inadequate consumption of other macro- and micronutrients (table III)
Table III Adjusted* nutrient intake, adequacy and percent of inadequacy intake (<100%) at the national level, by geographical region and by tertile of household wealth index. Mexico, Ensanut 2012
* Data are adjusted by sex, area, region, HWI and survey design using a quantil regression model
‡, §, # Statistically different between regions (p<0.05). ‡= Northern, §= Central, #= Southern
&, ≠, ∞ Statistically different between tertiles of Household Wealth Index. (p<0.05). &= Low, ≠= Medium, ∞= High tertile of HWI
By HWI tertile, no significant differences were observed in the intake, adequacy and inadequate consumption of energy. The intake and adequacy of proteins and fats (total and fatty acids), vitamin B12, vitamin D, folate, vitamin C and heme iron, were lower, and the adequacy of carbohydrates was higher, in the OA of the lower tertile, compared to the middle and high tertiles. As a result, the highest inadequacies in the intake of energy, and of most macro- and micronutrients, were observed in OA from the low tertile, compared to the middle and high HWI tertiles; the exception was the inadequate intake of saturated fat, sugar and cholesterol, where the proportion of OA with intakes exceeding the recommendation was higher in OA from the middle and high tertiles, compared to the low HWI tertile (table III).
Ensanut 2006
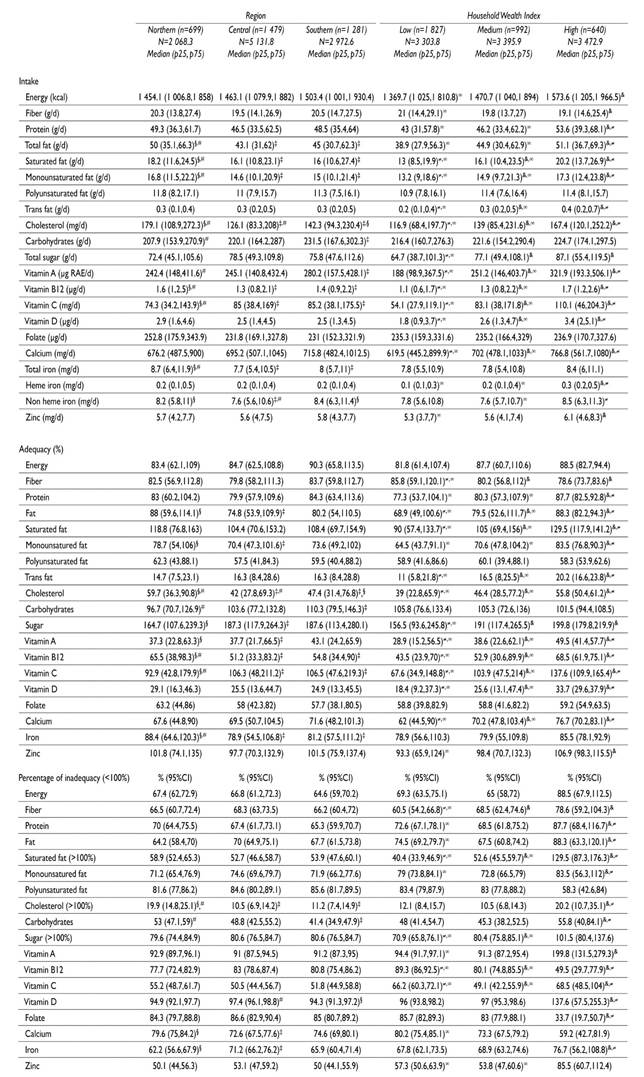
The median energy intake for OA in 2006 was 1 473 kcals, with an adequacy of 86%, where 66% of OA were below the energy requirement. By sex, women had lower intakes of energy, macro- and micronutrients, and higher adequacies of most nutrients, compared to men, except for folate, vitamin D, B12 and calcium, where the adequacy was higher in men than in women. A great proportion of OA (>80%) had inadequate intakes of polyunsaturated fats, vitamin A, vitamin B12, vitamin D, folate and sugars; and 50% of OA had an inadequate intake of saturated fatty acids. With regard to sex differences, a higher proportion of women with an inadequate intake of vitamin B12, folate and sugar was observed, compared to men (table IV).
Table IV Adjusted* nutrient intake, adequacy and percent of inadequacy intake (<100%) at the national level, by sex and by area. Mexico, Ensanut 2006

* Data are adjusted by sex, area, region, HWI and survey design using a quantil regression model
‡ Statistically different by sex (p<0.05)
§ Statistically different by area (p<0.05)
The energy intake and adequacy among the inhabitants of the rural and urban areas were not different. The intake and adequacy of unsaturated fats, vitamin D and non-heme iron was higher; and the intake and adequacy of sugar, vitamin A, B12 and heme iron was lower in OA from the rural area, compared to those from the urban area (table IV).
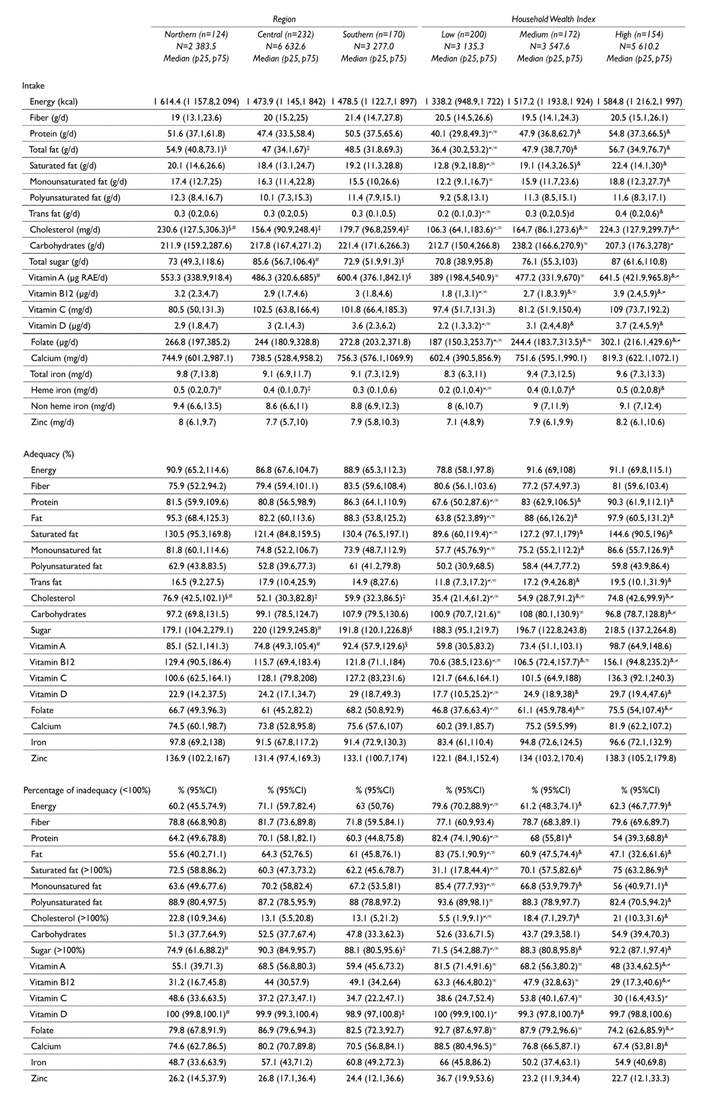
No differences were observed by geographical region in the median intake of energy. A higher energy adequacy was observed, however, in OA from the southern region, compared to those from the central and northern regions. OA from the northern region had a higher intake of saturated fat, intake and adequacy of total and unsaturated fats, cholesterol, vitamin B12, total iron and a lower intake and adequacy of carbohydrates and vitamin C, compared to the inhabitants of the central and southern regions. When comparing OA from the southern region, a higher intake and adequacy of vitamin A, vitamin C, and carbohydrates were observed compared to the northern and central regions (table V).
Table V Adjusted* nutrient intake, adequacy and percent of inadequacy intake (<100%) at the national level, by geographical region and by tertile of household wealth index. Mexico, Ensanut 2006
* Data are adjusted by sex, area, region, HWI and survey design using a quantil regression model
‡, §, # Statistically different between regions (p<0.05). ‡= Northern , §=Central, #= Southern
&, ≠, ∞ Statistically different between tertiles of Household Wealth Index. (p<0.05). &= Low, ≠= Medium, ∞= High tertile of HWI
By socioeconomic status, a tendency was observed of a lower intake and adequacy of nutrients in the low HWI tertile, compared to the high tertile. The intake of protein, total fats, saturated, unsaturated fats, cholesterol, trans fats, vitamin A, B12, C, D, calcium, heme iron and zinc was greater in OA from the high tertile compared to the middle and low HWI tertiles, except for the intake and adequacy of fiber and carbohydrates.
When comparing the middle vs the low HWI tertiles, differences were observed in a greater intake and adequacy of total fats; saturated, unsaturated and trans fats; cholesterol; carbohydrates; sugars; vitamins A, B12, C, D; calcium, and heme iron in OA from tertile 2 vs tertile 1. These tendencies were also reflected in the prevalence of OA who did not meet their requirements of energy, macro- and micronutrients; this prevalence was higher in OA from tertile 1 compared to those in tertile 3 (table V).
When comparing the median of energy intake between the two surveys, adjusting by sex, age, and BMI, no significant changes were observed in a greater intake and adequacy of energy, between the 2012 and the 2006 Ensanut surveys (p=0.68, data not shown).
Discussion
The results of this study document, for the first time, the intake and adequacy of energy and nutrients in Mexican OA showing high risks of dietary deficiencies of several micronutrients which are important for maintaining good health and a healthy aging process. During the period between 2006 and 2012, the energy and nutrient intakes have not been modified in a significant way, indicating that the quality of the diet of OA in Mexico has remained unchanged. The estimates of nutrient intake in OA allow us to monitor changes in their nutritional status, and to identify the subgroups of population with higher dietary inadequacies and health risk.
The median energy intake reported in this study is higher than that found for Chilean OA (>65 y), which is 1 300 kcals,20and very similar to what was observed in the OA population aged >60 in the US NHANES 1999-2000 (1 658 kcals).21 In Latin America, documentation of the dietary intake of OA that could allow us to compare our data has been scarce. Our data shows that 67% of OA do not meet their daily energy recommendations. This results could due to the dietary assessment method used, since the 7d SFFQ does not capture the “usual or habitual” diet of the OA (that explains the maintaining of their body mass) which, considering the underreporting of energy.12 These data regarding the energy intake contraste with the high prevalence of overweight, obesity and abdominal obesity. In addition, 66.5% of OA did not meet their estimated protein requirement (1g/kg/d), although it was not possible to differentiate between the sources of protein (animal vs. vegetable). A higher protein intake (1.2 to 1.5 g/kg/day) is recommended to prevent muscle loss.22 Changes in body composition due to the aging process predispose the OA to a higher risk of sarcopenia and loss of functionality.23 Adequate intake of protein could prevent this accelerated replacement.24,25
In agreement with what was reported for Chilean OA,20 the higher prevalences of inadequate intakes were observed in the those of essential nutrients, possibly showing that OA have a small variety of foods, scarce fresh vegetables and food sources of animal products, whose diets are mostly based on simple carbohydrates.
The low intake of vitamin B12 and folates observed in this study may predispose the OA to a higher risk of nutritional deficiencies, since both nutrients are critical in the prevention of cognitive impairment, anemia and neuromuscular disorders.26 Likewise, it is important to point out that in this population, there is a double burden of malnutrition, either by dietary deficiencies, or obesity problems. Abdominal obesity was observed in over 80% of the OA in both surveys, which, along with excessive intakes of sugar (20.9% of the total energy) and saturated fat (11.6% of the total energy, data not shown) predisposes them to a higher risk of NCDs.27
Few differences were observed in the consumption of energy and of some nutrients between the inhabitants of urban vs. rural areas in both surveys; in contrast to what was observed in younger Mexican adults,28 this lack of differences may be determined by factors that are common to the aging process, and which determine their total energy intake, but not the source of that energy.6 For 2012, the only observed difference was the intake of vitamin A, which was higher in the urban area vs. the rural one; but for 2006, the observed differences were for some essential nutrients and others with a higher risk (sugar) being consumed less in the rural compared to the urban area. This helps to explain why even though OA in both areas consume the same amount of energy, the source of this energy is different, with OA from the urban area consuming denser nutrients/kcal compared to the ones in the rural area. At this respect, it is necessary to document the food consumption pattern in order to describe the main foods sources of energy and micronutrients of this population.
A very low vitamin D intake and adequacy was also observed in both surveys. Practically all of the OA population does not meet the vitamin D recommendation, as stated by the WHO.14 This result is of concern, if we consider that a high inadequacy was also observed in calcium intake and that the lack of both of these nutrients predisposes this population to a greater risk of osteoporosis, frailty,29falls,30fractures,31,32functional dependency33 and loss of muscle function.34 In a random sample of 158 Mexican OA of the 2006 Ensanut, 33% had suboptimal concentrations of vitamin D.35 This problem has been recently documented in Latin America.36In Mexico, fortifying/adding vitamin D to milk is compulsory, at 200 IU/L.37 With this level of fortification, a very large milk intake would be required in order to satisfy the recommendations, which is not feasible in the case of OA. Thus, intervention strategies are needed to improve and ensure a greater intake of this vitamin to favor an adequate functioning and quality of life in the OA.
Socioeconomic status (SES) is one of the main social determinants that have an influence on dietary intake. The OA of the lowest HWI tertile had the lowest intakes and energy adequacies and the greatest micronutrient inadequacies, compared to the other two HWI tertiles, as was observed in OA from the southern region. Since the design of this study limits our ability to explain the temporary nature of the relationship between dietary intake and HWI, we suppose that SES determines their dietary intake, from an early advanced age, and the restricted dietary intake due to conditions of poverty and food insecurity38 puts them at a greater risk of adverse health events. Consequences of malnutrition such as frailty, sarcopenia, osteoporosis and chronic morbidity will be experienced by the older adult at an earlier age, only because of his/her socioeconomic condition.39
It has been reported that the SFFQ instrument underestimates energy intake. OA are more vulnerable to memory bias and underreport energy.40,41Although this could be a limitation, in the 2012 survey 7% of OA had a cognitive impairment, so that the 7d-SFFQ was answered by a person in charge of feeding them, or by their caretaker. For the 2006 Ensanut, we do not have information regarding cognitive impairment, but we estimate that the prevalence could have been the same or less than in the 2012 Ensanut.42 Due to the greater size of the population sample in 2006, and to the smaller proportion of OA >80 years old, the underestimation error in the intake of energy and nutrients in this population could be less. The proportion of underreports in 2006 was no different with respect to 2012.12 Also, non-parametric models were used for the adjusted intake estimation, which were not influenced by the extremes of the nutrient distribution.
This study describes the nutrient intake transversally, without the objective of statistically comparing the intake changes for macro- and micronutrients between the 2012 and the 2006 Ensanut surveys, mainly for methodological reasons: 1) The dietary methodology for the 2006 Ensanut11 varies with respect to 2012 Ensanut,12 2) The range of references of adequacies varies between both surveys, and 3) The SFFQ of 2012 considers 39 items more compared to the 2006 SFFQ; although we point out that both surveys used the same base for food nutritional composition, any interpretation of these changes must be done cautiously.
The SFFQ instrument used in this study differs from traditional FFQs used in other epidemiologic surveys in two main aspects:43,441) Its semiquantitative nature allows a more accurate estimation of portion sizes and intakes, and 2) A shorter recall period -7 days- prior to the interview could minimize recall bias normally associated with the use of FFQs for longer recall periods. This could favor its use for estimating actual intakes, instead of usual intakes, assuming that the week-by-week variability could be lower than the day-to-day variation. Additionally, the SFFQ used in this study has been previously validated in Mexican adults,45 showing usefulness to estimate the dietary intake in that population.
Information from diet consumption and nutrient distribution representative of Mexican OA is scarce, and validated instruments of food recollection are necessary to improve accuracy and precision in the estimation of recent and habitual diet in this population.
In conclusion, diet in older Mexican adults has not changed over the past six years, is low in various micronutrients that are important for maintaining an adequate nutritional status and optimal health, as well as high in sugar and saturated fat. Paying attention to diet in this age group by means of social programs and targeted interventions is necessary to promote a healthy aging

