











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
HIV transmission in Mexico is performed mainly through sexual practice and the HIV epidemic is concentrated among men who have sex with men (MSM), intravenous drug users, and sex workers.1 According to the National Surveillance System of HIV/AIDS in Mexico, by 2012 the prevalence of HIV at population level among individuals between 14 to 49 years old was of 0.24.2 In contrast, high HIV frequencies have been reported among MSM ranging from 9.8% through 20.4%.3,4 A control trial study performed among male sex workers found, at baseline, a HIV prevalence of 38%.5 Most current studies of HIV frequencies among female sex workers in Northern Mexico have fluctuated between 4.8 and 10.9% and intravenous drug use was significantly associated to that HIV prevalences.6,7,8,9 Nevertheless, no HIV prevalence study have been done among people who requested Voluntary Counseling and Testing in the HIV/AIDS preventive programs in Mexico.
In Mexico City, there is an HIV-specialized clinic called Condesa Clinic (CC) whose main objectives are to provide diagnosis, ambulatory care and referral of People Living with HIV. The clinic is also the venue of the HIV/AIDS Program of Mexico City, which offers HIV testing and supports programs to reach key populations.10 We started a fast and comprehensive HIV diagnosis at CC using a rapid HIV-antibody test, followed by Ag/Ab Combo HIV, HBsAg, anti-HVC and anti-TP CLIA testing applied in parallel to all participants. Since the fall of 2011, CD4 count and HIV-1 viral load tests were added to all HIV positive individuals in their first laboratory studies visit. During the first quarter of 2012 we added a rapid CD4 count to those reactive to HIV rapid test to better support a quick medical referral the first day. Herein, we describe the laboratory approach utilized for HIV and sexually transmitted diseases (HIV/STI) detection in the first visit and timely HIV diagnosis among people who have recently requested HIV Testing and Counseling (HTC).
Materials and methods
Study design and study population: This is a cross-sectional study performed from November 2011 to September 2012. There were 3 390 women and 7 095 men selected who requested HTC at CC.
Ethics: The research protocol of this study was evaluated by the Ethics Committee of El Colegio de la Frontera Norte.
Samples: After pre-test counseling and signing of an informed consent, a four ml-tube of blood was taken from each participant for rapid HIV and CLIA testing. Those individuals with a reactive rapid test provided two more blood samples for CD4 cell count and HIV-1 viral load measurement. Pre and post counseling and informed consent followed the statements of the Official Mexican Norm for the prevention and control of HIV infection.11 Complete laboratory results were delivered in five days. HIV-positive patients discussed the results with a peer counselor who led them to medical consultation the first day. Non-assisting patients, those with non-reactive rapid HIV test but suspected of acute HIV infection (CLIA HIV Ag/Ab positive) and those who turned out positive for other tests were invited by telephone to contact the clinic. Acute HIV infection was defined as a non-reactive HIV rapid test, a positive CLIA Ag/Ab result, a negative or indeterminate HIV-antibody profile test and a HIV viral load of more than 500 000 copies, excluding those with CD4 cell counts of less than 200 cells.12
Laboratory assays: Whole venous blood samples from all participants were assayed with an HIV-antibody rapid test, Uni-Gold HIV, Trinity Biotech. We established an algorithm of confirmation of all HIV rapid test positive samples with Abbott Architect HIV Ag/Ab Combo, Abbott HIV-1 RNA RT-PCR and Orgenics Immunocomb II HIV 1&2 Combfirm. Furthermore, each serum in the positive samples were assayed with Abbott Architect HBsAg, anti-HCV and syphilis TP followed by Venereal Disease Research Laboratory (VDRL) of Syphilis TP positive. With the samples that were non-reactive to the HIV rapid test, we prepared pools of four sera before testing with the Architect HIV Ag/Ab, HBsAg, Hepatitis C Virus (anti-HCV) and syphilis tests. Positive pools were developed and the individual sera were assayed to identify the positive ones. This approach allowed the identification of acute HIV infections as we reported before.13
Data analysis: A descriptive analyses was performed to estimate the global prevalence of HIV, Syphilis, Hepatitis B (HBsAg) and Hepatitis C (anti-HCV) serological markers; stratifying them by sex and including the prevalences of HIV coinfection with serological markers of the above mentioned STIs. Bivariate and multivariate analyses, separating women and men, were carried out to estimate the prevalence odds ratio of being HIV-infected in relation to age as well as to Syphilis, Hepatitis B and Hepatitis C status. The distribution of CD4 cell counts among HIV positive individuals was classified into three groups: a) a cell count of >350 was considered timely diagnoses, b) cell counts between 200 and 350 were considered as untimely diagnoses, and c) cell counts of <200 were considered as late diagnoses. Bivariate analyses of the CD4-count categories were performed stratifying their distribution by sex and age. Finally, a multinomial logistic regression was used to compare the three CD4-cell count categories in relation to sex and age, (category [a] was taken as reference). Descriptive and bivariate analyses were performed using SPSS version 18, and multivariate analysis was carried out with STATA, version 10.1.
Results
The global seroprevalence of HIV, syphilis, HBsAg, and anti-HCV markers were 20.1, 6.0, 1.0 and 1.0, respectively. Men displayed 5.7, 9.3, 14 and 1.6, times higher seroprevalence of HIV, syphilis, HBsAg, and anti-HCV infection markers, respectively, than women (table I). Men had a higher prevalence of co-infection of HIV and all STI serological markers (syphilis, HVC and HBsAg) than women. There were eight cases of acute HIV infection (all among men) and were more frequent among young people: three in the 18-27 year old age group, three in the 28-37 year old age group. Characteristics such as age and syphilis, HVB (HBsAg), and anti-HCV sero-status behaved differently among women than among men. Taking the youngest age group as the reference among women, the 28 to 37 year old age group and the oldest of over 58 years of age had 1.8 (95%CI, 1.5-2.6) and 3.4 (95%CI, 1.6-7.6) times higher risks of being HIV infected, respectively, than the reference group (table II). The risk of syphilis infection among HIV-infected women was 5.4 (95%CI, 2.2-13.1) times higher than among HIV-negative women. There was no relationship between the HIV infection and the HVB (HBsAg), or anti-HCV sero-status among women. Among men, the 28 to 37 and 38 to 47 year old age groups had 1.5 (95%CI, 1.3-1.6) and 1.8 (95%CI, 1.5-2.1) times higher risks of being HIV-infected than the reference group. Furthermore, the risk of HCV, HBV and syphilis infection among HIV-seropositive individuals was 3.5 (95%CI, 2.2-5.6), 8 (95% CI, 4.9-13.2) and 5.4 (95% CI, 2.2-13.1) times higher, respectively, than among HIV-seronegative individuals (table II).
Table I Global prevalence and prevalence stratified by sex and co-infection percentage of HIV,* syphilis, ‡ HBsAg, and anti-HCV among Voluntary Counseling and Testing (VCT ) patients studied at Condesa Clinic in Mexico City from November 1st, 2011 to September 28th, 2012
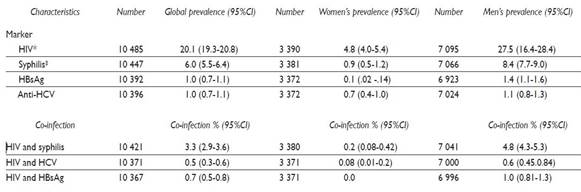
* HIV-Ag/Ab positive
‡ Anti-TP positive and VDRL positive
Table II HIV* seroprevalence and its distribution by age, syphilis,‡ anti-HCV, and HBsAg infections among women and men studied at Condesa Clinic in Mexico City from November 1st, 2011 to September 28th, 2012
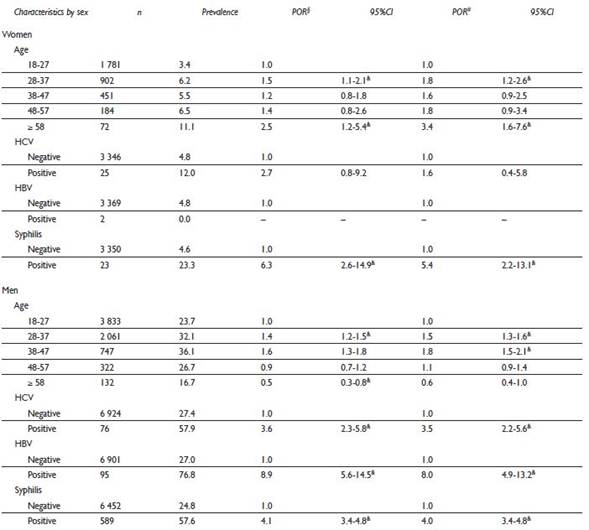
* HIV-Ag/Ab positive
‡ Anti-TP positive and VDRL positive
§ Crude prevalence odds ratios
# Adjusted prevalence odds ratios
& p<0.05
We also analyzed the timeliness of an HIV diagnosis with respect to the studied individuals’ sex and age, and we found a significant association between these variables (table III). Using a CD4 cell count > 350 as the reference category, we found that the risks of belonging to the intermediate category (CD4 cells count between 200 and 350) were higher among the 28 to 37 (1.4, 95%CI, 1.1-1.8) and the 38 to 47 (1.6, 95%CI, 1.2-2.4) year old age groups, respectively. Furthermore, the probability of a late diagnosis (CD4 cell count ≤ 200) was related to the fact of being a woman (1.6, 95%CI, 1.1-2.3) and it increased with age in all categories.

Discussion
The results of the present study show that the global HIV prevalence among the studied individuals was as high as 20.1%. Most importantly, HIV prevalence among women and men in every month of the study fluctuated lightly around the mean values without showing a clear ascending or descending trend along the study period (data no shown). As a result, we are expecting a very high prevalence of HIV cases among consecutive voluntary attendees at CC along the time.
We were able to identify eight acute HIV infection cases. These results suggest that most acute HIV cases are provided by young men who are requesting VCT. The epidemiological importance of this finding is that people with acute HIV infection are highly infectious due to rising levels of virus concentrations in plasma. Special care should be applied among people with acute HIV infection as prevention counseling and antiretroviral therapy to reduce infectiousness to others.12
It is important to point out that among men the prevalence of HIV infection was 5.7 times higher than among women. The prevalence of HIV infection among men in our study was also higher than many of those reported in other studies on MSM in different countries around the world.14 The UNAIDS 2012 report estimated a prevalence of HIV infection of 17% among MSM in Mexico.15 However, a HIV prevalence of 30% and even 40% among MSM in Mexico City has been reported after 1988.16 More recently, a study that reported HIV prevalence among MSM in 24 cities across Mexico found a global frequency of 16.9% with fluctuations according to the distribution of the cities in five regions: the Central-East region had the highest HIV frequency (20.4%) and the Central-West region had the lowest (9.9%).3 Even so, HIV prevalence among men was 27.5% in this study, which represents one of the highest reported in Mexico.
As expected, HIV prevalence among men was related to age and STI markers. The risks of HIV infection were associated to relatively young groups of age (28 to 47 years). This figure is consistent with the distribution of cumulative cases of HIV/AIDS in Mexico among men since the beginning of the HIV epidemic and up to 2012.17 The high odds ratios of STIs among HIV-infected individuals suggest high-risk sexual practices among the studied men. This is the case of the hepatitis B marker that were statistically correlated to the HIV infection (OR: 8, 95%CI, 4.9-13.2) as had been reported in a previous study of men seeking HIV testing in Mexico City,18 as well as of the syphilis antibody (OR: 4, 95%CI, 3.4-4.8) as reported in a systematic review paper on MSM.19 Although the odds ratio of the HCV infection among HIV infected men was high (3.5, 95%CI, 2.2-5.6), the results presented in this study showed a low HCV infection seroprevalence (1%) and an HIV plus HCV co-infection of 0.6%. These results suggest that the HCV infection is incipient among HIV-infected persons diagnosed at CC. This contrasts with MSM who practiced intravenous drug use in Mexico and whose HIV and HCV seroprevalence was 1 and 99%, respectively.20
Although women displayed a much lower HIV infection frequency than men, it is still high compared to the HIV prevalence at the population level. The National Survey on Health and Nutrition carried out in 2012 reported a global prevalence of HIV infection of 0.15% at population level in Mexico.21 Thus, in our study women’s HIV infection prevalence was 32 times higher than the general population’s. This result suggests that women who seek care at CC are at a high risk of being HIV infected. A study carried out among women who requested an HIV test at a Conasida Clinic in Mexico City found that 4% prevalence of HIV infection was related to a history of blood transfusions and to having an HIV-infected partner, but it was not associated to the women’s own sexual behavior.22 In the present study, seroprevalence of STIs were low and the frequencies of HIV and STI markers co-infection were very low among the studied women. On the other hand, the only marker associated to the HIV infection was syphilis. Therefore, the high prevalence of HIV found among women suggests that women could have been exposed to the HIV infection through their own sexual behavior but also through contact with an infected male partner.
We found that almost one third of the studied subjects (31.8%) had a late HIV diagnosis according to the CD4 cell marker. This figure is lower than the ones previously reported in Mexico: 43.2 and 61%.23,24 Our results differed from the ones in these two reports because we used a different definition of late HIV diagnosis and because the results of these two studies were obtained at secondary and tertiary levels of medical care in Mexico. On the contrary, CC is a facility that belongs to the first level of medical care where timely diagnosis of HIV is essential to establish early treatment if necessary.
Finally, the prevalence of late HIV diagnosis displayed variations of around 30% throughout the study period, which points to the fact that many of the people who requested HIV testing had a late contact with CC. The characteristics associated to these subjects were age and sex. The multinomial analysis showed no difference regarding sex among the people with an untimely HIV diagnosis, taking the timely HIV diagnosis category as reference. However, the risks of untimely HIV diagnosis appeared among the 28 to 37 and 38 to 47 year old age groups, taking the youngest age group as reference. Most importantly, the risk of a late HIV diagnosis was higher among women than among men. This result contrasts with the conclusions from other studies performed in Mexico in which men displayed a higher prevalence of late diagnosis compared to women.23,24 Therefore, the studied women could have cultural and social disadvantages that hinder their seeking care at CC care and getting an early HIV diagnosis.25 There was also a trend of an increasing risk of late HIV diagnosis associated to older age groups. Factors related to the delay in seeking HIV testing in this population could include stigma and discrimination, as well as a lack of worry about the HIV infection.26
In conclusion, this study carried out an evolving laboratory approach of people who sought care at CC. This provided elements to develop an integral program to deal with a population with a high HIV and STIs prevalence and high frequency of late HIV diagnosis. However, this study has limitations as the own cross-sectional design implies. The main disadvantage of this study was the lack of information about different characteristics of the studied individuals like socioeconomic level, use of illicit drugs or sexual practices. Thus, we could not control during the analysis, the associations between the magnitude of HIV and STI and important characteristics of the population studied. These limitations indicate that the conclusions of this study must be interpreted with caution.

