











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Smokefree laws protect nonsmokers from secondhand smoke and reduce tobacco-induced diseases.1 The 2005 World Health Organization Framework Convention on Tobacco Control’s2 (FCTC) Article 8 commits parties to implementing smokefree laws.3
The experience of high income countries4,5,6,7,8,9,10 shows that successful implementation requires active education and enforcement,9,11 appropriate enforcement agencies,5 and support from nongovernmental organizations (NGOs).4 Tobacco companies encourage noncompliance directly and through third parties,4,11 lobbying,6,9,10,12 litigating,7 and thwarting the implementation of rules.8,13
Smoke-free implementation for low and middle-income countries (LMICs) is challenging because tobacco companies often have more resources than the health authorities,14 and tobacco industry activities are less controlled,12 making implementation weak or uneven.15,16,17
Colombia, with an adult smoking prevalence of 12.8% in 2007,18 low for Latin America, adopted national smokefree policies before many LMICs.19 In May 2008, the Health Ministry issued Resolución 1956 de 2008 (Ministerial Resolution No. 1956), mandating smokefree indoor public areas. In July 2009, Ley 1335 de 2009, a comprehensive tobacco control law, expanded smokefree coverage to all hospitality venues,20 making Colombia the country with lowest gross domestic product per capita with such a national smokefree law.21
Successful implementation of Colombia’s 2008 resolution and 2009 law involved national and local health department efforts, with technical and financial help from domestic and international health NGOs.
Materials and methods
From July 2014 to July 2015, we reviewed Colombian government ministries’ resolutions, administrative orders, government agency webpages, and public documents related to Colombia’s 2008 smokefree resolution and 2009 tobacco control law, articles of daily newspapers with national reach dated between January 2008 and July 2015, and related legislation, court rulings, and local government resolutions, using standard snowball methods.
We conducted interviews with 14 in-country tobacco control advocates, national and local health authorities, and policymakers between October 2014 and December 2014 following protocol IRB #10-01262 approved by the University of California, San Francisco Committee on Human Research (table I.)22 Informed consent was obtained in accordance with ethical principles of medical research involving human subjects of the Helsinki Declaration.
Table I Key Actors Influencing Implementation and Interviewed Actors. Colombia, 2008-2016
* Agency reached as part of key informant interviews
‡ Calderón L. Interview of Lorena Calderón, tobacco program manager at the Ministerio de Salud y Protección Social, by Randy Uang, Bogotá, Colombia. 2014
§ Hernández B. Interview of Blanca Hernández, former tobacco program manager at Ministerio de la Protección Social no longer working on tobacco, by Randy Uang, Bogotá, Colombia. 2014
# Ronderos M. Interview of Margarita Ronderos, professor at Pontificia Universidad Javeriana, by Randy Uang, Bogotá, Colombia. 2014
& Rivera Rodríguez DE. Interview of Diana Esperanza Rivera Rodríguez, former public policy director, Instituto Nacional de Cancerología, by Randy Uang, Bogotá, Colombia. 2014
Results
Early attempts at smokefree legislation
Colombia’s 2008 smokefree resolution and 2009 law were adopted after decades of failed attempts23,24 that were blocked by tobacco industry interests, tobacco-growing area legislators a and the Ministry of Agriculture,a despite tobacco being less than 0.1% of Colombia’s exports.25 In 2006, Sen. Dilian Francisca Toro, a physician allied with President Álvaro Uribe (2002-2010),26 became Senate President and pushed for Colombia to join the FCTC,27 which it did in April 2008. Health advocates then argued for legislation to comply with the FCTC.a
Colombia’s 2008 smokefree resolution and 2009 law
Resolución 1956 de 2008, issued in May 2008 by the Health Ministry28 (then called the Ministry of Social Protection), mandated smokefree indoor public areas nationwide.
Ley 1335 de 2009 (“Law 1335 of 2009”), sponsored by Sen. Toro, passed in July 2009 to implement FCTC Articles 8 and 10-16 including smokefree areas, prohibiting tobacco advertising, promotion and sponsorship, and prohibiting individual cigarette sales.a The law went beyond Resolución 1956 de 2008 (table II),29 by requiring smokefree grounds of educational institutions, cultural institutions such as museums, and health facilities. The Instituto Nacional de Cancerología (National Cancer Institute, part of the Health Ministry), Liga Colombiana Contra el Cáncer (Colombian League Against Cancer), the Colombia-based Latin America branch of Corporate Accountability International, and Sociedad Colombiana de Cardiología (Colombian Society of Cardiology) supported its passage;23,30,31 representatives friendly to the tobacco industry opposed it.23 Philip Morris, British American Tobacco, and local tobacco company Protabaco tried unsuccessfully to permit designated smoking areas.23
Implementation of the smokefree provisions did not face the concerted tobacco industry opposition common elsewhere,4,6,9,10,11,12,13,16,32 likely because the companies seem to have focused on countering the prohibitions on tobacco advertising, promotion and sponsorship.
Processes and results in implementation
The Health Ministry, local health authorities, local police, NGOs, the national barowners’ association (Asobares), and individual establishments, including universities, contributed to implementation. Implementation, with generally good compliance and enforcement, varied regionally. As in high income countries,33,34,35 implementation included guidance from the Health Ministry to local health departments, education by health departments and advocates, and enforcement by local health authorities and police, especially in major cities. In 2015, a survey in large cities found that 92% of nonsmokers and 91% of smokers supported the 2009 law.36
National-local dynamics
Colombia’s low state capacity37 meant limited national agency efforts. Health policy implementation was decentralized across local health agencies for Colombia’s major cities, 32 departamentos (departments), and capital district. The Health Ministry provided guidance, but local agencies had autonomya in educational efforts, and worked with local police on enforcement.
National government activities
To implement the 2008 resolution, in December 2008 the Health Ministry distributed a “circular”,38 i.e. a memo to local health departments, detailing that it expected local public education and enforcement activities, without requiring specific activities.
For the 2009 law, the Health Ministry shared surveillance, education, and enforcement practices among local health departments.b Bogotá included smokefree surveillance in routine health inspections,b resulting in 162,000 inspections in 2009 and 197 000 by 2011,39 with compliance in a low-income Bogotá neighborhood estimated at 91%.40 The Instituto Nacional de Cancerología provided technical assistance to the Health Ministry, including monitoring.c Limited Health Ministry resources for tobacco control,d however, meant the absence of a strong national smokefree education campaign.41
The Procuraduría General de la Nación (National Inspector General), constitutionally responsible for ensuring compliance with laws by government agencies, did not focus on compelling local smokefree education and enforcement because it was focused on Colombia’s internal armed conflict and conflict-related human rights.42 The Health Ministry asked the Procuraduría to focus more on local health agency smokefree education and enforcement, and the Procuraduría issued a “circular” memo43 requesting local health departments to implement the law, but did little follow-up, which resulted in variations in activity.
Local government bodies’ activities: Regional variation
Implementation was strongest in big cities and in cities with supportive political leadership: Bogotá (population 8 million), Medellín (2.4 million), Cali (2.3 million), Colombia’s most influential cities, and two southwestern cities, Popayán (250 000) and Pasto (480 000), with personally committed mayors. Local health departments distributed materials to business owners and the public before and after implementation.
Implementation was weakest in rural areas and the Atlantic coast, with less interest from agencies in these arease. Health advocates had focused on large cities,e and the Colombian state had more presence in departmental capitals. Rural and small-city health agencies often knew little of the lawe or claimed having limited resources and personnel.44
Supportive political leadership in Popayán and Pasto resulted in the reiteration of the local health departments’ implementation responsibilitiesf,g and in crafting educational efforts annuallyf,g for restaurant, bar, and nightclub owners,e,g by the mayors’ offices. Popayán also conducted smokefree education at schools.e,g
Local police: Attention to public security
Consistent with FCTC guidelines,3 the 2009 law authorized enforcement by local police and health authorities. Given Colombia’s armed conflict, many police departments did not prioritize smokefree enforcement; however, Bogotá, Medellín, and Pasto’s health departments convinced local police to carry out enforcement.b
Signage requirements
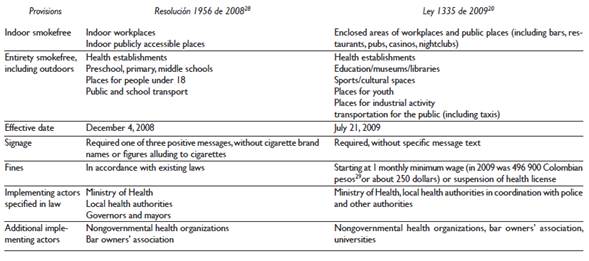
The 2008 resolution required establishments to post signs with specified smokefree messages (“For the good of your health, this space is free of cigarette or tobacco smoke,” “Breathe easy, this space is free of tobacco smoke,” “Welcome, this establishment is free of tobacco smoke”). The resolution prohibited cigarette brand logos and images “alluding to cigarettes” so the signs did not carry the international “no smoking” symbol. Establishments could post signs referring to smokefree environments (a positive message) without any “no smoking” symbol (a negative message), then optionally could post additional signs carrying the symbol. The 2009 law required signage about smokefree environments, but without a predefined list, allowing for more expansive text (figure 1). Since “no smoking” signs may prime smoking tendencies,45 Colombia’s positive smokefree messaging may have improved compliance.
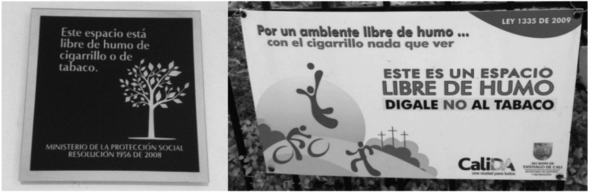
Figure 1 Examples of smokefree signs posted following the 2008 smokefree resolution, with a specific message mandated by the resolution (on left, “This space is free of cigarette or tobacco smoke”) and a smokefree sign citing the 2009 tobacco control law, with more expansive text (on right, “This is a smokefree space; say no to tobacco”)
Outside funders: Supporting NGO activities
Organizations outside Colombia funded Colombian NGOs to create educational materials and train local health department staff. As elsewhere in Latin America, the US-based Bloomberg Foundation’s Initiative to Reduce Tobacco Use funded Colombian NGOs for smokefree education, training, and monitoring, totaling 501 563 dollars through October 2015.46 Corporate Accountability International’s Colombia-based staff highlighted noncompliance starting in 2008 and provided technical assistance to defend the 2009 law against potential industry litigation.e The Bogotá-based Universidad Sergio Arboleda improved community involvement in 2010-2012, the Liga Colombiana Contra el Cáncer (Colombian League Against Cancer) conducted smokefree education in 2012,h and the health and civic group Fundación FES trained local health departments in 2014.i
In particular, the Liga Colombiana Contra el Cáncer and Corporate Accountability International joined Senator Toro in 2011 to highlight noncompliance to the Ministry of Health and news media.42 Since health advocates in the 2000s had sensitized journalists to tobacco control,j coverage often called for national and local efforts.
Advocates also worked with the Bogotá-based Universidad Sergio Arboleda to create “Opción No Fumar” (the Non-smoking Option) campaign, distributing flyers, postcards, and pamphlets about the law.h By July 2013, “Opción No Fumar” had distributed 29 350 pamphlets.47
Controversy about terraces: The merchants’ federation Fenalco and NGO vigilance
The Federación Nacional de Comerciantes (Colombian Merchants’ Federation, Fenalco) interpreted the 2009 law’s smokefree provisions as not applying to terrace areas of restaurants and bars. Fenalco had cooperated in the past with tobacco industry “youth smoking prevention” programs48 designed to displace government action.49
In 2010 and 2011 Fenalco distributed flyers to business owners and employees claiming smoking in terraces was allowed44,50 because they were not under roofs 51 and claimed that health advocates were maligning Fenalco for its interpretation.51 Despite the support of the Health Ministry and NGOs,44,50 whether implementation included terraces depended on local health authorities. Medellín only enforced covered terraces,52 while in 2011 Bogotá’s health department declared it would enforce all terraces.53
Strong support from the Bar Owners’ Association (Asobares)
The Asociación de Bares de Colombia (Asobares, Association of Bars of Colombia) supported implementation strongly but initially had opposed the 2008 resolution,k reflecting the efforts of the tobacco industry to turn hospitality groups against smokefree laws.4,6 Some of Asobares’ executive committee were personally affected by secondhand smoke, so Asobares surveyed its members and found that a majority supported the resolution, so shifted to supporting it.k The tobacco industry did not appear to interfere with this change.
Asobares conducted intensive education for bar owners for six months before the 2008 resolution’s December 4 effective date,k including brochures, and bar coasters co-sponsored by the Health Department of Bogotá, Bogotá Mayor’s Office, and World Heart Federation, reading: “Si va a fumar, hágalo afuera” (“If you are going to smoke, do it outside”).k Asobares provided candy to people who stepped outside to smoke, had models come to bars to give prizes to such people, and worked with the Bogotá government on a protocol for the emergency services number (123), which would summon police to eject patrons who insisted on smoking indoors.k These activities set a tone of compliance from the start.
University activities: Smokefree outdoors
Universities developed educational campaigns to implement smokefree educational institutions. In Bogotá, 21 universities cooperated to develop similar campaigns, and in Cali, 13 universities joined a local health department network to share information on campaigns.54,55 The Pontificia Universidad Javeriana in Bogotá and Cali, with personal interest from the Bogotá campus rector,l had the Bogotá campus establish signs at campus entrances and major outdoor locations, including a life-size sign of a student announcing a smokefree campus. The Cali campus put signs throughout, including person-high signs saying, “En la universidad no se fuma” (“At the university, there is no smoking”).56
Discussion
Like high income countries,4,11,57Colombia’s successful smokefree implementation required sustained engagement by national and local health authorities, NGO, external funders, the national bar owners’ association, and universities. Different from high income countries, in Colombia there were few government resources, weak state capacity, and enforcement agencies focused on public security.
Like many Latin American countries, Colombia lacked a strong national smokefree education campaign,16 but had many vigorous local campaigns.45 Colombia benefited from national and local agencies and support from legislative champions, and notably has a successful history of public health policies.58,59
Three factors in Colombia especially contributed to strong implementation. First, noncompliance vigilantly exposed by NGOs, including for terraces, as in the case of local implementation in Mexico and the US.4,13 The merchants’ federation argued against applying the law to terraces, creating an ambiguity about patio-like areas that also occurred in the US.6,9,10,11,60
Second, support by the Bar Owners’ Association set a tone of compliance similar to that of California in the US,61 showing how organizations within the society, not just government agencies, are essential to compliance. Since 2008, Asobares, with the help from the Campaign for Tobacco-Free Kids, visited hospitality associations throughout Latin America to encourage national smokefree laws.k
Third, international organizations aided implementation, supporting NGOs to provide education and technical assistance.62 Sustained resources are necessities for long term compliance,63 and external funding often does not last, so international organizations’ support provides a crucial opportunity to help LMIC smokefree implementation.
These factors contributed to robust implementation despite Colombia’s health policy decentralization, weak state capacity, and public security issues.
Policy implications
Smokefree legislation should clearly cover all workplaces and specify national and local agency responsibilities. Health advocates should cultivate hospitality association support in advance of legislation, when possible. International funders should continue strongly funding LMIC implementation, as moderate resources can make substantial impacts.

