











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkThe global demographic transition has resulted in a greater number of adults and elderly population than in previous decades.1 Currently, chronic diseases are one of the leading causes of death among adults all around the world. According to Global Burden of Diseases (GBD), injuries, and risk factors enterprise, the GBD has continued to shift away from communicable to non-communicable diseases and from premature death to years living with disability.2 In terms of the number of years of life lost due to premature death in Mexico, ischemic heart disease, diabetes mellitus, and chronic kidney diseases were the highest ranking causes in 2010, with high body mass index (BMI), high fasting plasma glucose, and bad dietary habits as the leading risk factors responsible for most of the disease burden.2,3
Evidence from nationally representative surveys show that overweight and obesity trends have increased over time. According to the National Health and Nutrition Survey 2012, 71% of the Mexican population is either overweight or obese and this combined prevalence is growing an average of 0.7 percentage points per year.4,5 This increase will have a tremendous impact on public health in Mexico, since obesity is strongly associated with several chronic diseases, such as diabetes mellitus and cardiovascular diseases.6-8
Certain factors have been linked to the growing BMI around the world, which include trends towards less healthy lifestyles, more calorie dense diets, decreasing levels of physical activity, and more sedentary behaviors. The nutritional transition occurring in Mexico is characterized by: 1) the increased availability of low-cost processed foods that contain high amounts of fat, sugar, and salt; 2) an increase in fast food consumption; 3) less available time for food preparation; 4) a significant increase in exposure to food and beverage advertising; and 5) behaviors that result in decreased levels of physical activity.7,9
Given the public health importance in terms of magnitude and costs generated by chronic diseases, in addition to the complexity of the aforementioned risk factors, we need longitudinal studies that can identify the prevalence and trends of non-communicable diseases. Cohort studies can also help explain how specific lifestyle factors (e.g. dietary patterns, physical activity, smoking and alcohol consumption) can influence the development of chronic diseases among the Mexican population. The Health Workers Cohort Study (HWCS) is an ongoing prospective cohort study conducted in Central Mexico with the objective to examine the association between certain lifestyle and genetic factors and different health outcomes. Therefore, our aim is to provide evidence that can be translated into effective programs and policies that will help to reduce the occurrence of chronic diseases in the Mexican population.
Materials and methods
Cohort population
The HWCS participants are medical, administrative, and academic employees (and their families) from three different institutions: the Mexican Social Security Institute (IMSS, by its acronyms in Spanish) and National Institute of Public Health (INSP, by its acronyms in Spanish), both located in Cuernavaca, Morelos, and workers from the Autonomous University of Mexico State (UAEM, by its acronyms in Spanish) located in Toluca, Mexico. Initially, each institution delivered announcements and invitation letters to workers who were also asked to invite their relatives to take part in the study. During the baseline assessment conducted from March 2004 to April 2006, approximately 11 000 female and male participants were voluntary enrolled in the HWCS, after providing informed consent. For the baseline assessment, all participants were asked to complete an extensive self-administered questionnaire at home. After completing the questionnaire the participants visited the Research Centers for numerous physical examinations and a fasting blood sample collection.
The second assessment of the cohort took place six years after the initiation of the study (2010 to 2013), this served as a follow-up for the original participants and provided baseline information for new subjects who were enrolled in the HWCS. During the follow-up phase, a subset of approximately 2 500 participants of the HWCS among IMSS employees in Cuernavaca who were initially enrolled were invited to participate, and 1 855 (74%) took part in the second evaluation. Additionally, 1 206 new participants were enrolled in the second examination of the HWCS (Figure 1).

Measurements in the HWCS
During the baseline and follow-up assessments the participants completed a self-administered questionnaire10 and provided detailed information about their demographic characteristics (e.g. birth date, education, marital status, employment status); medical family history, past medical history, current medication use, lifestyle information (e.g. diet, physical activity, smoking status, alcohol consumption, etc.); body type (e.g. weight change, self-reported anthropometric measures, self-perception of body weight); psychosocial factors (e.g. life stressors, stress and social networks, perceived stress); social support and quality of life (e.g. depression symptoms, sleep quantity); extensive reproductive history (for females); partner violence; and cognitive assessment. The 20162017 follow up will also include sun exposure assessment.
Dietary measurements
As reported in prior publications,11,12 a semi-quantitative food frequency questionnaire (FFQ)13 that has been validated in a Mexican population,13 was used to assess diet. To test the FFQ's reproducibility, it was administered twice, at a 1-year interval, to 134 women residing in Mexico City and the validity results were then compared with those from the set of four diet recall tests given at 3-months intervals. For the first FFQ, the de-attenuated coefficients varied from 0.65 for saturated fatty acids to 0.12 for polyunsaturated fatty acids. Whereas, for the second FFQ, the coefficients ranged from 0.63 for total fat to 0.21 for polyunsaturated fatty acids.13
Briefly, this questionnaire obtained data regarding the consumption frequency of 116 food items during the previous year. For each food, a commonly used portion size was specified and the participants were asked how frequently they consumed the food during the previous year. With a comprehensive database of food content, we computed the energy and nutrient intake by multiplying the frequency of consumption of each food by the nutrient content.14
Physical activity measurements
Physical activity (PA) was assessed using a questionnaire that has been validated in Spanish15 and adapted for the HWCS population in Mexico as follows: 1) adding some leisure-time activities that are common among the Mexican population such as football and fronton, as well eliminating weightlifting and sailing, which are less common, and 2) adding more specific choices to the workplace domain such as carrying moderate or heavy loads, pushing objects, climbing the stairs and using tools.16,17
Participants were asked to report the amount of time they spent engaged in specific activities during their leisure-time and work place contexts. The PA section on leisure-time activity included 16 items on the amounts of weekly time spent performing exercises like walking, running, cycling, etc. The PA questionnaire collected information about the frequency (days/week),the amount of time (hours/week), and intensity (light, moderate and vigorous) of activities carried out during a typical week in the last year. The questionnaire also measured the time engaged in sedentary activities such as watching TV and playing video games.10
Psychosocial measurements
We used a self-administered version the Center for Epidemiologic Studies-Depression Scale (CES-D),18 which was designed to measure current levels of depressive symptoms in the general population and also is a worth tool for epidemiological studies.
The CES-D has high internal consistency and adequate test-retest repeatability. In addition the CES-D scale has showed consistence in the reliability, validity and factor structure across a wide variety of demographic characteristics among the general population.18 The design of this scale allows its application to study the relationships between depression and other variables also in subgroups of the population; due its properties the CES-D has been widely used in different cultures and languages, among them in Spanish-speaking population; the Spanish version has been validated in Mexican population as well.19 A 20-item version was used to determine which participants were free of depressive symptoms and to evaluate depressive symptoms at baseline and follow-up.20
The main components of the CES-D related with depressive symptomatology included in the 20 items of the scale were depressed mood, feelings of guilt and worthless-ness, feelings of helplessness and hopelessness, psychomotor retardation, loss of appetite and sleep disturbance; the response categories of each item scores from zero to three according to the frequency of occurrence of the symptom.10,18
Anthropometric and clinical measurements
Body weight was measured with a calibrated electronic scale (model BC-533; Tanita) with participants wearing minimum clothing and no shoes. Height was measured using a conventional stadiometer (Seca), with barefoot participants standing with their shoulders in a normal position. Measurements were taken with the tape in a horizontal plane perpendicular to the vertical scale, touching the top of the head at the moment of inspiration. Waist circumference was measured at the highest point of the iliac crest to the nearest 0.1 cm.21,22
Subjects' blood pressure was measured twice during each study visit by a trained nurse using an automatic monitor. The first measurement was taken after 5 min of rest, while participants were sitting with the dominant arm supported at heart level. The second measurement was taken in the same way, five minutes after the first.23
Nurses trained who used standardized procedures performed all measurements. Reproducibility was evaluated, resulting in concordance coefficients between 0.83 and 0.90 for anthropometric and clinical measurements.
In addition a Lunar DPX NT instrument was used to measure body composition and body bone mineral density, bone mineral content, lean body mass, appendicular lean body mass, and fat mass.24,25 Well-trained technicians obtained all the measurements following standardized procedures. Daily quality assurance scans were conducted using the phantom provided by the manufacturer, and technicians ensured that the daily variation coefficient (VC) was within normal operational standards and in vivo VC was lower than 1.0-1.5%.
Also a Sunlight Omnisense bone sonometer (Sunlight Omnisense 8000P; BeamMed Ltd, Tel Aviv, Israel) was used to evaluate the rate of bone mass gain and loss. A sonometry of two peripheral bones was performed at the distal radius and mid tibiae, following the standardized procedures outlined in the operator manual. The coefficient of variation of this instrument ranged from 0.5 to 1.0% in vivo.
Biological measurements
In the baseline assessment, a fasting venous blood sample (fasting time ≥ 8 hours) was collected for each participant. Approximately 20 ml were obtained for clinical laboratory measurements and for biorepository purposes. Routine hematology tests (e.g. hemoglobin, hematocrit, etc.) and chemistry tests (e.g. aminotransferase, triglycerides, glucose, total cholesterol, high-density lipoproteins, low-density lipoproteins, uric acid, creatinine, etc.) were performed. All biomedical assays were processed using a Selectra XL instrument (Randox), in concordance with the guidelines of the International Federation of Clinical Chemistry and Laboratory Medicine.26 Assessment of serum vitamin D levels on subjects from the second and third phase.
During the second assessment, in a particular group of samples, in order to respond to particular questions we followed approaches such as genotyping of candidate genes using the Golden Gate assay. In this initial phase of the study, a total of 288 SNPs in genes involved in the Bone Metabolism, Obesity and non-alcoholic fatty liver disease (NAFLD), were selected.27,28 These SNPs were selected using the following criteria: minor allele frequency (MAF) >5 % in Caucasians, and polymorphisms previously associated in candidate gene association studies, genome wide association studies (GWAS) and meta-analyses. Finally, 96 ancestry informative markers (AIMs) were included in the design to be used to detect and adjust for population stratification and estimate the ancestry of the sample. These AIMs distinguish mainly Amerindian and European ancestry (δ>0.44) and have been validated in other study of the Mexican population.29 Genotyping was performed on Illumina BeadStation. Duplicate control samples were genotyped on each array, which also served as internal controls. The primary analysis of the genotyping data with the Illumina GenomeStudio software was followed by visual inspection and assessment of data quality and clustering. Genotyping accuracy was also assessed by genotype clustering using the Illumina GeneTrain score, which is a measure of the clustering confidence of individual SNP alleles.
We are also extending our research to genomewide association studies (GWAS) and from genome to epigenome. We are performing genome-wide profiling at proteomic, transcriptomic and micro-RNA level by microarrays, for hypothesis related to bone metabolism and some other related to liver disease.
Ethics
The study protocol, questionnaires, procedures, and informed consent forms were approved by the corresponding IRBs of all participating institutions: the Mexican Social Security Institute (12CEI 09 006 14), the National Institute of Public Health (13CEI 17 007 36), and the Autonomous University of the Mexico State (1233008X0236). Signed written informed consent was obtained from all participants prior to enrollment.
Baseline characteristics of study participants
A total of 10 729 subjects were enrolled in the baseline HWCS, with an age range of 6 to 94 years. Most of the participants were adults over the age of 20 years (86.4%), while 13.6% were younger than 20 years. Among adults, the mean age was 43.8 ± 14.2 years. The percentage of current smokers was slightly higher in males (28.0%) than in females (20.1%), and more than half of the participants had an education level beyond high school (53.4% among females and 59.9% in males), and a greater proportion were married (57.4 and 80.2% for females and males, respectively).
Among the children and adolescents, slightly more girls (56.1%) were enrolled than boys (43.9%). Most of the initial HWCS participants in this age group were non-smokers (82.6 and 81.0% for girls and boys, respectively). Additionally, the percentage of low physical activity was marginally higher among girls (15.5%) than in boys (14.3%) (Table I).
Table I Baseline demographic characteristics of participants in the Health Workers Cohort Study
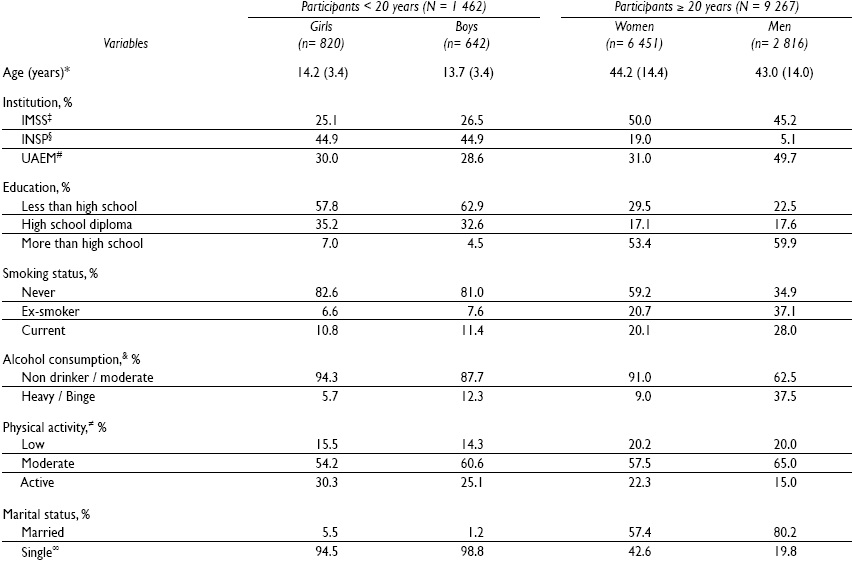
* Mean (SD)
‡ IMSS: Social Security Mexican Institute
§ INSP: National Institute of Public Health
# UAEM: Autonomous University of the Mexico State
& Alcohol consumption: Heavy (3 or 4 drinks/per day for males and 2 to 4 drinks/per day for females); Binge (5 or more drinks/per day for males and females).
≠ Low <90 min/week, moderate ≥ 90 to < 150 min/week, active ≥ 150 min/week
∞ Unmarried, divorced, widowed
Among adults, mean BMI was 26.8 ± 4.8 kg/m2, while in children and adolescents the average BMI was 21.4 ± 4.4 kg/m2. The prevalence of overweight or obesity among adults was 70.2% for males and 61.3% for females. In subjects under the age of 20 years, the combined prevalence of overweight and obesity was 23.7% (23.3% for girls and 24.3% for boys). Among the adult participants, 43.4% had plasma triglycerides > 150 mg/dL, 17.7% had an elevated fasting glucose, and 77.5% had low HDL-c concentrations. The estimated prevalence of metabolic syndrome at baseline was 28.6% (30.0% for females and 25.4% for males) (Table II).
Table II Baseline clinical and anthropometric characteristics of participants in the Health Workers Cohort Study
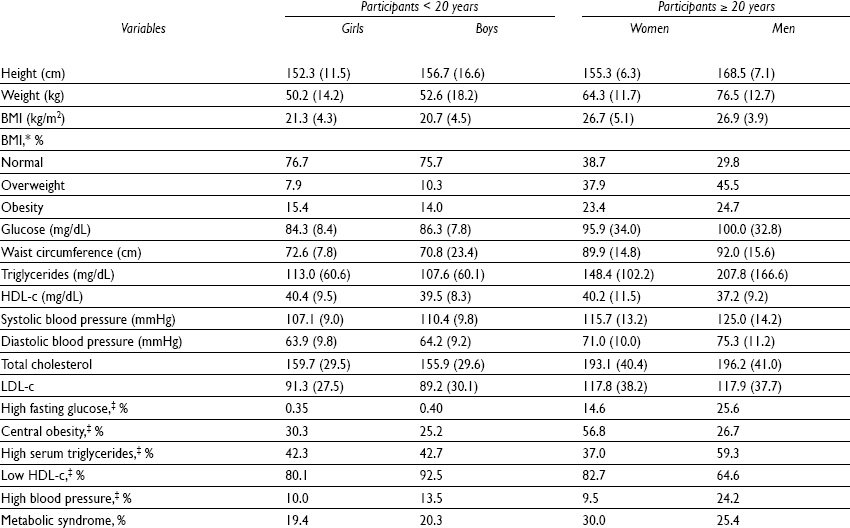
* For participants <18 years: Normal, <1.0 Z-scores; overweight, ≥ 1.0 Z-scores to <2.0 Z-scores; and obesity ≥ 2.0 Z-scores. For participants ≥ 18 years: Normal, < 25.0 kg/m2; overweight ≥ 25.0 to < 30.0 kg/m2; and obesity, ≥ 30.0 kg/m2
‡ For participants < 18 years: High fasting glucose (≥100 mg/dL and < 126 mg/dL), high serum triglycerides (≥100 mg/dL), low serum HDL-c (<50 mg/dL except in boys aged 15 to 19 was 45 mg/dL), central obesity (> 75th percentile for age and gender), high blood pressure (<90th percentile for age gender, and height).
For participants ≥ 18 years: High fasting glucose (≥100 mg/dL and <126 mg/dL), high serum triglycerides (≥150 mg/dL), low serum HDL-c (≤50 mg/dL for women and ≤ 40 mg/dL for men), central obesity (waist circumference ≥ 88 cm for women, and ≥ 102 cm for men), high blood pressure (≥130/85 mm Hg)
First reports and key findings
The baseline and longitudinal results from the HWCS have been reported in some publications. These papers report the effects of different lifestyle factors (e.g. dietary patterns and physical activity) on different health outcomes (e.g. metabolic syndrome, osteoporosis, cardiovascular disease risk, liver disease, depression, etc.).30-36 The longitudinal results regarding the association between specific environmental and genetic factors and risk of developing osteoporosis or non-alcoholic fatty liver disease, have also been published.37-39
Some of the analysis have addressed our population's diet using the dietary pattern approach and studied associations with some outcomes like metabolic syndrome,40 obesity,11 low bone mineral density,25 and insulin resistance.41 In general, to derive dietary patterns energy consumed from each food was converted into a proportion of the total consumption of energy per day, and subsequently standardized using Z-scores. The foods and beverages on the questionnaire were categorized into 22 to 28 food groups,42,43 which were used as the basis for the dietary pattern derivation. Dietary patterns were derived with principal components analysis of the food groups. The resulting factors were orthogonally rotated (varimax rotation) to improve their interpretation. We estimate the factor scores for each dietary pattern by adding the consumption of the food groups weighted by their factor loading, and each participant received a score for each of the identified patterns. When we evaluated the association between Mexican adults' dietary patterns and 10-year predicted cardiovascular disease,42 we found that the multivariate relative risks across quintiles (Figure 2) of the prudent dietary pattern were 1.0, 0.84, and 0.40 (P-trend = 0.006). On the other hand, participants in the highest quintile of the refined-foods dietary pattern were more likely to develop elevated 10-year predicted CVD than were those in the lowest quintile (RR: 2.98; 95%CI: 1.46, 6.10; P-trend = 0.020). Finally, the meat/fish dietary pattern was not significantly related with 10-year cardiovascular disease.
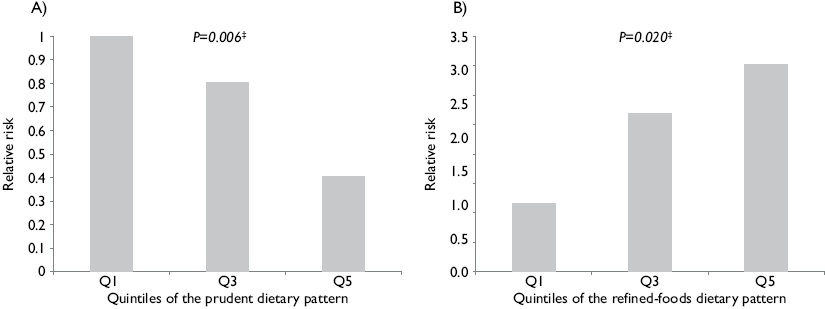
* Adjusted for: Age (<30, 30-39, 40-49, 50-59, 60-69 ≥70 years), sex, time period (four two year periods); smoking status (never, past and current smoking), alcohol consumption (nondrinker, moderate and heavy), multivitamin use (yes or no), parental history of myocardial infarction (yes or no), history of hypertension (yes or no), physical activity (min/day), and postmenopausal hormone ujse (yes or no); body mass index (<25 kg/m2 or ≥25 kg/m2); energy intake (quintiles)
‡ To assess the overal trend, we computed the Mantel-Haenszel extension chi-quare test
Figure 2 Relative risk of 10-year predicted cardiovascular disease42 according to quintiles of the a) prudent dietary pattern and b) refined-foods dietary patterns*
Limitations and strengths
The HWCS has several limitations. The main weakness is that our cohort study only includes people living in Central Mexico, so the results may not be generalizable to the rest of the population. However, we consider that the HWCS population could be representative of adults living in urban areas in Central Mexico. Another important challenge is the relatively small size of the cohort (n= 1 855), since not all of the participants were followed up in the second assessment. Additionally, as reported in a previous cohort study,44 the assessment of main exposures and other risk factor information is based on self-reported data that may be subject to error. Therefore, an analysis of the data in terms of validity is recommended.
Some of the main strengths of the HWCS include having both male and female participants, a wide range of ages (6 to 94 years), the use of standardized methods to evaluate body composition, the use of previously validated instruments to measure different exposures (e.g. diet, physical activity, and depression). Another important strength of our cohort study is that we have bio-specimens that can be used to evaluate the role of genes and their interaction with environmental variables to establish the causality of multiple chronic diseases.
To the best of our knowledge, the HWCS is the first prospective study to evaluate the association between specific lifestyle and genetic factors and different health outcomes, including diabetes mellitus, cardiovascular disease, osteoporosis, and liver disease among others. Another objective of the HWCS is to identify biomarkers, polymorphisms, and other disease modifying effects, as well as the life course processes that correlate to health and disease in Mexico. Our results to date provide evidence from a low-middle income country, where the environmental, socioeconomic, and lifestyle conditions may differ from those of high-income countries. Compared with the general population of Mexico, the HWCS participants had a slightly lower but similar prevalence of overweight and obesity, and metabolic syndrome than those subjects studied in the 2012 National Health and Nutrition Survey.4
Future plans
The HWCS is a longitudinal study can provide new insights into disease mechanisms and prevention through the analysis of genetic, environmental, and lifestyle risk factor information in a large sample of Mexicans. In the short term, we will conduct the third follow-up assessment of the HWCS during 2016-2017. During this phase we will apply a similar self-administered questionnaire that will collect information on demographic characteristics, medical family history, past medical history, current medication use, lifestyle information, psychosocial factors,45 etc. Some of the objectives for this third phase of the HWCS are to identify factors associated with healthy ageing, to identify biomarkers (e.g. microRNAs), disease modifying effects, and to analyze the role of the gut microbiome and metabolite profiles in health and disease; we are building a database that will be used in the genetic dissection of human complex diseases. The blood samples will be collected for extraction of DNA, RNA and proteins and biobanking. We will use approaches of genomic tools, statistical and bioinformatical methods. These approaches involve candidate gene and genome-wide association studies (GWAS). The candidate gene approach focuses on association between SNPs with selected genes of interest and phenotypes or disease status. In contrast GWAS, scan the entire genome for common genetic variation (e.g. SNPs). We will also use genome-wide transcriptome analyses and proteome protein expression profiling, to find new biomarkers involved in the diseases.

