











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkDietary assessment represents a continuing challenge, principally in large-scale studies. The development of valid, efficient, and cost-effective instruments for measuring dietary intakes for specific populations is still a key research prioritiy.1,2 Different dietary methods, such as food records (FRs), 24-hour dietary recalls (24DRs),1 and food frequency questionnaires (FFQ), can be used for assessing habitual dietary intake. Although FRs and 24DRs have been successfully employed and shown to be accurate methods; the time, respondents' motivation, participant's literacy, and economic constraints of these dietary instruments make them unsuitable for most studies.3 On the other hand, among the various instruments planned to assess nutrient and food intake, the FFQ are used to estimate individual perception of standard food intake over a reference period of time such as months or years. In contrast with other dietary assessment methods, the FFQ are easier to administer. They are relatively less expensive, less difficult to achieve, and they also offer a rapid estimate of usual food intake;1,4 making them more feasible for epidemiological studies. The FFQ have been commonly used as a practical and efficient method to assess habitual diet over periods of time in dietary surveys.1 They have also provided reasonable measurements of energy, macronutrients, and micronutrients in different countries.5-8 However, all FFQ should be adapted to the target population due to the great differences in food supply, as well as the broad range of dietary habits from one population to another.1 In addition, it is well acknowledged that nutritional values reported from FFQ data can be subject to random and systematic measurement errors, which can profoundly influence the design, analysis, and interpretation of nutritional epidemiological studies.9,10 Therefore, to correctly interpret the results of epidemiological studies that use FFQ, there is a need to know the relationship between reported intakes from the FFQ and true usual intakes.11 Until now, different methods have been employed for the validation of dietary intakes. However, limitations like cost and degree of invasiveness of the biomarkers,12 and others related to the FR like reduction of the response rate, and even a change in subjects' diet, are important factors limiting their use in validation studies.13 For that reason, collection of multiple 24DRs has been suggested as another comparison standard method for the validation of dietary intakes. Actually, approximately 75% of the validation studies of the FFQ are validated against multiple 24DRs, which have been found to be suitable for comparison with questionnaires to establish validity.4
Since 2006, as part of the Mexican National Health and Nutrition Survey 2012 (Ensanut 2012, by its Spanish acronym), a semi-quantitative food frequency questionnaire (SFFQ) was used for assessing the dietary intake of Mexican population. However, the created SFFQ has not yet been properly validated. Therefore, the main objective of the present study was to evaluate whether this SFFQ is valid in Mexican adolescent and adult populations by comparison with the average of two 24DRs.
Materials and methods
The present analysis was done with data from the Ensanut 2012, that is a probabilistic population-based survey with multi-stage stratified sampling, designed to be representative of the nation, its three main regions (North, Central and Mexico City, and South), and rural and urban areas. The survey design and sampling procedures have been previously described in detail.14 Briefly, the Ensanut 2012 aims to monitor health and nutrition conditions, health program coverage, and access to health services. The survey obtained information from 50 528 households, with a response rate of 87%; 46 303 interviews with adolescents and adults were conducted.
Design and study population
For the present study, data was collected in three phases. First, identification of selected housing field; second, application of household and individual questionnaires; and third, the application of the dietary questionnaires, and anthropometric measurements. The SFFQ and the first 24DR were electronically collected after the first and second phase. Finally, the second 24DR was collected 2 or 3 days apart from the first 24DR.
Using a simple random sampling, a subsample of 186 adolescents and 278 adults (≥ 20 years) were included for a validity study. Among them, for the present analysis, 178 adolescents and 230 adults, who had complete information of one SFFQ and two 24DRs, and with no outlier energy (values between 600 and 6 000 kcal) and nutrients intake values,15 were included.
This study was conducted according to the Declaration of Helsinki guidelines, and written informed consent was obtained from either the participants or their parents (for participants below 18 years old) before they were enrolled in the study. Research Ethics Committee at the National Institute of Public Health (INSP, for its acronym in Spanish) revised and approved the informed consent forms and the study protocol.
Dietary assessment
The semi-quantitative food frequency questionnaire
The electronic SFFQ used in the Ensanut 2012 is an adapted version of the questionnaire employed in the Ensanut 2006.16 Briefly, the food list (101 food items) included in the questionnaire used in the Ensanut 2006, as well as the portion size, and mean weight of portion for each population group were estimated by a group of INSP researchers from the analysis of the most-consumed-foods data obtained from the National Nutrition Survey 1999. The new version of the final SFFQ (used in the Ensanut 2012) includes consumption of 140 foods during seven days prior to the date of the interview. Frequency of food items could be characterized by set categories ranging from never to six times a day. Participants also designated the portion size of the ingested food items, using predefined categories. These data were first converted to times per day, and then portion size per day was computed. To calculate the consumption of energy (kcal/day) and daily nutrients intakes, the daily frequency of consumption (portions/day) of each food was multiplied by the amount of energy and nutrients in a standard serving or portion size of that food (using the food composition tables compiled by the INSP), and the contributions of all foods were totaled using Microsoft Visual FoxPro 7.0. The SFFQ was collected by personnel trained in standardized data collection and entry procedures.
24-hour dietary recall
Participants completed two electronic 24DRs distributed over all days of the week; the first 24DR was obtained at the same time of the SFFQ. Personnel trained in standardized methods collected all the required information through face-to-face interviews, using 24DR automated multiple pass method (24DR-AMPM software version 1.0) developed and adapted to the Mexican population by a group of INSP researchers.* For each 24DR, participants were asked in detail about their food consumption during the previous day. In brief, at the beginning of the interview, participants listed the food items they had consumed during the previous day (since the moment they woke up until they went to sleep), with no prompts from the interviewer about different possible eating occasions. A list of foods that are often forgotten was also used to elicit recall, in this case the interviewer got back to the beginning of the preliminary food list and helped the interviewer remember foods frequently omitted. Subsequently, the food list obtained in the previous steps was organized according to the time each food was consumed and the context each meal was done (place and activities). Then, detailed information on each food item was collected, for example: 1) the food was single, dish or recipe; 2) the amount of single food consumed or ingredients used in a recipe (in household measures or food weight); 3) the type of food weight (net or gross); 4) the food preparation method (raw, cooked, steamed or oven); 5) the total amount of the food served; 6) the amount of food that was not consumed; 7) how processed foods were consumed (frozen and/or packaging). Lastly, a review of the final food list was made in order to obtain additional information or to correct any specific data that had been improperly recorded. We calculated the daily mean intakes of energy, macro and micronutrients, estimated by the two 24DRs. The average 24DRs data were used as the standard to measure the relative validity of the SFFQ.
Other participant characteristics
Sociodemographic characteristics (age, sex and socioeconomic status) were obtained with predefined questionnaires. Localities with less than 2 500 residents were considered rural, and areas with 2 500 or more residents were considered urban. A household wealth index (HWI) was created using principal components analysis with household characteristics and family assets. This index was divided into tertiles, with 1 being the lowest category.
Statistical analysis
We performed descriptive analysis of the main characteristics of interest; means were computed for continuous variables; and frequencies and percentages were calculated for categorical variables.
Means and medians were computed for energy and nutrient intakes assessed by the SFFQ and the 24DRs. For the purpose of this study, the following nutrient intakes were compared: energy (kcal), protein (g), total fat (g), saturated fat (g), monounsaturated fat (g), polyunsaturated fat (g), cholesterol (mg), carbohydrates (g), dietary fiber (g), calcium (mg), magnesium (g), iron (g), zinc (g), vitamin A (ER), vitamin D (mcg), vitamin B12 (mcg), vitamin C (mg), and folate (mcg). We log-transformed the dietary data to improve the normal distribution and reduce skewness. The residual method was employed to eliminate the possibility of variation due to energy intake.5,17
Pearson correlation coefficients (PCC) were computed to evaluate the relationship between the energy and nutrients from the SFFQ, log-transformed and energy adjusted, and the average of two 24DRs. We also calculated deattenuated correlation coefficients, using the approach described by Rosner, to take into account within-person variations caused by day-to-day fluctuations.18 Additionally, to assess the validity of nutrient values, derived from the SFFQ, we also used regression analysis and compared them with the mean of the two 24DRs.
Kappa statistic19,20 was used to evaluate how well the SFFQ could categorize individuals into quartiles of the nutrient distributions when compared with the average 24DRs categorization. For the present analysis, subjects were classified into quartiles based on the energy-adjusted nutrient intakes. The degree of misclassification was calculated by examining the proportion of subjects classified by the reference method that fell into the same, adjacent, or extreme quartile when classified by the SFFQ.
Furthermore, Bland and Altman21 plots were used to graphically examine the agreement for energy, carbohydrate, fat, and protein intake between the two methods.
All statistical analyses were performed with STATA statistical software version 13.0. A value of p<0.05 was considered to be statistically significant.
Results
Overall, 186 adolescents and 278 adults (≥20 y) participated in the validation study. Of these, six adolescents and 28 adults were removed from the present analysis as their estimated daily energy intake was less than 600 kcal/day or >6 000 kcal/day. Additionally, participants who left 10 percent or more food items blank on the questionnaire were also excluded (two adolescents and 20 adults). For the present analysis, a total of 178 adolescents and 230 adults who completed two 24DRs and the SFFQ were included.
Among the adolescents who participated in this study, 50% were females; and the average age was 15.5 ± 2.3 y. Of the adult participants eligible for this analysis, 58.3% were females and 41.7% were males; the mean age was 41.4 ± 12.2 y; and 62.6% were from urban areas (Table I).
Table I Characteristics of participants in the validation study from the Mexican National Health and Nutrition Survey 2012. México, Ensanut 2012

* Mean and standard deviation
In adults, values for energy and nutrients estimated by the SFFQ were slightly higher than those obtained with the 24DRs, except for protein, polyunsaturated fatty acids, fiber, and magnesium. In this age group, the SFFQ overestimated by 265 kcal the energy intake, and overestimated nutrient were particularly high for carbohydrate, calcium, vitamin A, and folate. In adolescents, all the mean values of the 24DRs were lower than those of the SFFQ, except cholesterol, vitamin D, and vitamin B12. The analysis of nutrient intakes showed significant differences in energy, saturated fat, carbohydrates, calcium, zinc, vitamin C, and folate between SFFQ and 24 DRs (Table II).
Table II Mean and median daily nutrient intake estimated by the average of two 24DRs and one SFFQ. Mexico, Ensanut 2012

* P-value <0.001
‡ P-value <0.01
§ P-value <0.05
# Not significant, when we compared the average of 24DRs vs SFFQ
Overall, in adults, PCC of crude unadjusted data varied from 0.25 (iron) to 0.49 (saturated fat). Whereas in adolescents' coefficients for energy and crude nutrient intakes ranged from 0.21 for vitamin D to 0.51 for carbohydrates. In subjects older than 20 y, correlation coefficients (CC) above 0.40 or higher were voted for total energy intake, total fat, saturated fat, monounsaturated fat, cholesterol, carbohydrates, and calcium. In both age groups, the adjustment of total energy slightly improves the PCC in some nutrients (e.g. saturated fat, vitamin C), but decreases the values in others (e.g. polyunsaturated fat, protein). Except for that of zinc and polyunsaturated fat in adolescents, all correlations were statistically significant with p<0.05. Adjustment for within-person variability (deattenuated coefficients) increased all values of the CC, ranging from 0.30 for folate to 0.61 for saturated fat in adults and 0.19 to 0.61 for zinc and calcium in adolescents, respectively (Table III).
Table III Validity Pearson correlation coefficients between daily nutrient intakes estimated by the 24DRs* and SFFQ. Mexico, Ensanut 2012

* 24DRs; the average of two 24 hour dietary recalls
‡ All nutrients were log-transformed
§ The energy-adjusted correlations between dietary methods use the residuals from regressing each nutrient on the total calories (residual method)
# The deattenuated correlation coefficient was calculated using the ratio of the within-to between-person variance measured from the 24DRs. The formula used to calculate the corrected correlation was:
& P-value <0.001
≠ P-value <0.01
∞ P-value <0.05
∅ Not significant
In the cross-classified analysis (Table IV), a subject would be correctly classified if their energy or nutrient intakes were ranked into the same or an adjacent quartile. In adults, for most of the nutrients, the proportion of subjects classified into the exact same quartile varied from 30.0% (vitamin D) to 44.8% (monounsaturated fat), whereas, the percentage of misclassification (extreme or opposite quartile) ranged from 10.8 for total fat to 19.1 for vitamin A. On the other hand, for adolescents, classification of subjects into one quartile (in the same or adjacent categories) ranged from 55.6% for polyun-saturated fat to 69.3% for carbohydrates. For this age group, extreme misclassification into opposite quartile was weak with values between 8.7% (carbohydrates) and 17.6% (folate).
Table IV Regression analysis between de semi-quantitative food frequency Questionnaire (SFFQ) and the average of the two 24-hour dietary recalls (24DRs). Mexico, Ensanut 2012

* 24DRs; the average of two 24 hour dietary recalls.
‡ All nutrients were log-transformed and energy adjusted
According to Bland and Altman plot analysis, we found that for energy and all macronutrients, both methods showed good level of concordance. For example, for energy, approximately five adolescents and ten adults fell outside the limit of agreements. Similar results were observed for proteins, carbohydrates and lipids (Figures 1 and 2).
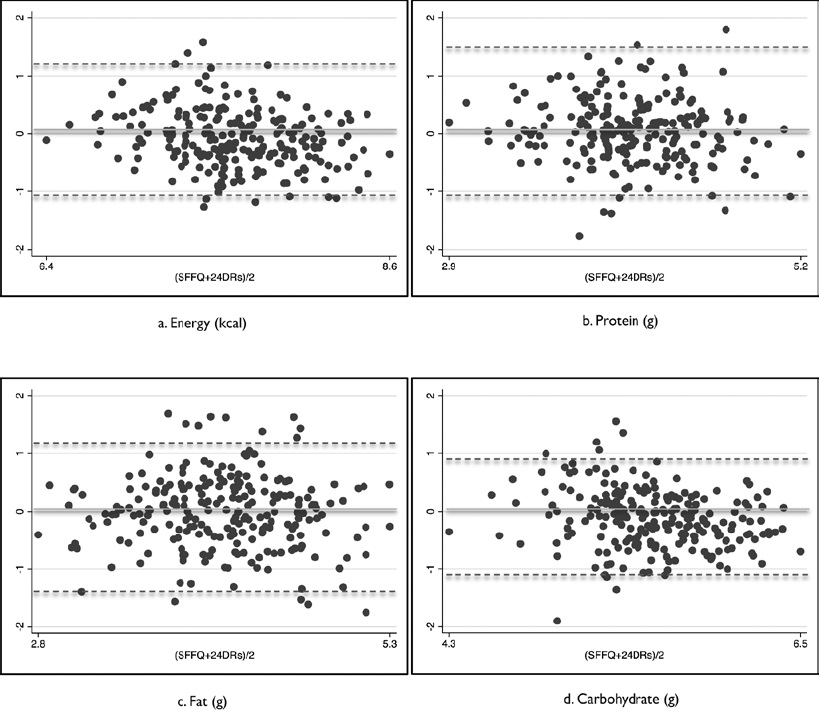
Figure 1 Bland and Altman plots for energy and macronutrients with the mean difference and limits of agreements in adults. Bland and Altman plots for a. energy, b. protein, c. fat, and d. carbohydrate, with the mean difference (solid line) and 95% limits of agreements (dashed lines) in adults

Figure 2 Bland and Altman plots for energy and macronutrients with the mean difference and limits of agreements in adolescents. Bland and Altman plots for a. energy, b. protein, C. fat, and d. carbohydrate, with the mean difference (solid line) and 95% limits of agreements (dashed lines) in adolescents
Discussion
The present study evaluated the relative validity of a 140-item SFFQ in a Mexican adolescent and adult population. Comparing daily nutrient intake, obtained from the SFFQ, with those derived from the average of two 24hour dietary recalls, our results indicated that the SFFQ had moderate to good relative validity (varied from 0.30 to 0.61 in adults and from 0.19 to 0.61 in adolescents) for most macroand micronutrients. Additionally, we observed a good agreement between the two methods when exploring interquartile categorization, as more than 63% adults and 62% adolescents were correctly classified into the same or adjacent quartiles for energy and most macro and micronutrients.
The absolute estimated energy, macroand micronutrient intakes derived from the SFFQ were in general higher than those derived from the reference method (24DRs), which is very often reported in previous validation studies.20,22-28 This possibly results when people are asked to recall the frequency of a large number of foods consumed in an FFQ and thus, they might tend to overestimate their actual intake. Also, difficulty in conceptualizing the assigned portion sizes and difficulties in reporting the frequencies of usual intake could be related.1 For example, in a study conducted by Kristal and colleagues29 that evaluated bias of FFQ when measuring fruit and vegetable consumption, they found that estimated intakes were lower when comparing a brief questionnaire (FFQ with only seven items) with dietary recalls; whereas, when they compared an FFQ with thirty or more items with a dietary recall or food records higher intakes were observed.
Usually, the association between FFQ and reference method have been assessed by correlation coefficients,1 and due to the numerous measurement errors for each dietary assessment instrument, the observed correlation coefficients are measures of relative validity.25,30 In general, the CC computed for each nutrient in the present study were similar or slightly lower than the ones reported in other validation studies carried out among adolescent26-28 and adult population.22-25,30 In our study, the average PCC, between SFFQ and two 24DRs, for absolute nutrient intake was 0.365 for adults and 0.374 for adolescents.
For both adults and adolescents, corrections by energy adjustment increased the observed CC for some nutrients, but decreased the CC for the majority. This may indicate, according to Willet and Stampfer,19 that energy adjustment increases CC when the variability of nutrient consumption is related to energy intake, but decreases CC when the variability depends on systematic errors of overestimation and underestimation. In our study, the lower correlations' values found in some nutrients may indicate that the SFFQ, to some extent, systematically over/underestimated intake of those nutrients. However, error in over/underestimation is expected in the SFFQ. Similarly, Liu and colleagues,24 Dehghan and colleagues,30 Deschamps and colleagues,26 Slater and colleagues,31 and Xia and colleagues28 found that energy adjustment did not improve the crude correlations in their studies.
Regardless of the differences between 24DR and SFFQ in the present study, due to the correction for day-to-day variation intakes, deattenuated correlations coefficients were usually higher than crude correlations. Our results, in both adults and adolescents, showed that for more than 60% of nutrient, deattenuation increased the correlations and they were ≥ 0.40, which is considered as valid. Our results are lower than some reported by previous validation studies,11,32 but comparable to others.24,30,31,33 For example, with respect to energy, lower coefficients have been informed in the Willet FFQ (approximately 0.17 when both genders were combined), and the Block FFQ (0.39 when both genders were combined)34 as compared with 0.53 (both genders) derived from adult population in our study. In terms of macronutrients, it was particularly evident that our correlations for protein were lower than the coefficients observed in other macronutrients (0.33 for adults and 0.34 for adolescents). However, our findings were similar to those obtained in previous validation studies7,26 conducted in Mexico in adult women (0.29 to 0.32) and other study carried out on French adolescents (0.33). Additionally, we observed low correlations for polyunsaturated fat (0.36 for adults and 0.21 for adolescents), which are similar to the coefficients observed in other studies.22-28 This result could be a consequence of the SFFQ development, which mainly focused on food items that substantially contributed to energy intake. In this respect, the assessment of nutrients that contribute little to the energy intake such as polyunsaturated fat, could be difficult. Certainly, polyunsaturated fat consumption comes mainly from intake of fatty fish, nuts, and some oils; in our SFFQ questions on fish intake were based on preparation (canned fish in oil, water or tomato; dried or salted fish; fresh fish) which influences energy intake rather than on the kind of fish, which would be important for a more accurate estimation of polyunsaturated fat intake. Despite our deattenuated CC for some micronutrients, specially zinc (0.31 and 0.19) and folate (0.30 and 0.30) in both adults and adolescents, respectively, were low, they were significant with p values <0.05, suggesting reasonable agreement between the two dietary methods. Other studies have also reported poor correlation for micronutrients.11,24,26
Table V Cross-Classification of adjusted daily mean intakes of nutrients into Quartiles estimated from the SFFQ and the 24DRs*. Mexico, Ensanut 2012
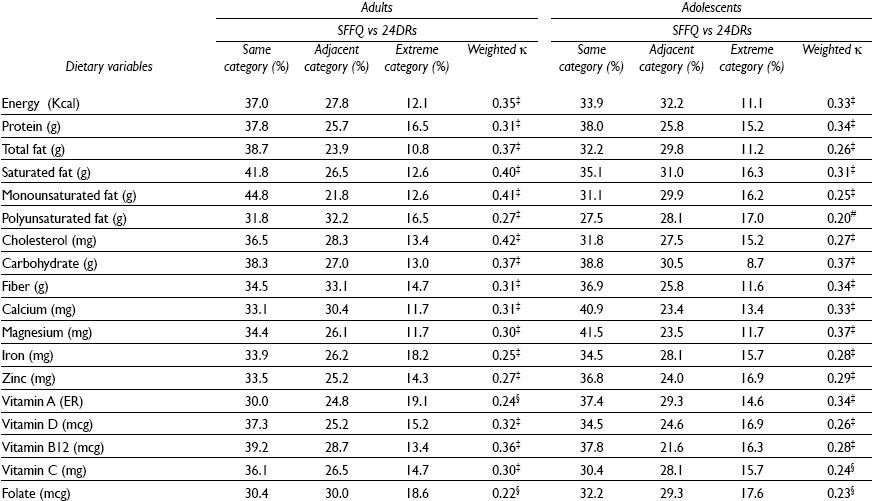
* 24DRs; the average of two 24 hour dietary recalls
‡ P-value <0.001
§ P-value <0.01
#P-value <0.05
The CC is usually accepted for measuring the strength of association between new methods against the comparison of the "gold standard" method. However, the use of correlation analysis for assessing validity has frequently been questioned on the basis that it does not measure agreement between the two methods. Generally, FFQ are used for ranking individuals according to food or nutrient intake rather than for estimating absolute levels of intake. In this respect, we used cross-classification into quartiles of intake and weighted kappa to assess the agreement and showed that the two dietary instruments were comparable. Despite some differences in the estimation of nutrients, for the majority of nutrients, approximately more than 60% of adults and adolescents were classified in the same or an adjacent category, which is consistent with other studies.23-31 This result demonstrated reasonable good agreement between methods and may reflect good sensitivity for our SFFQ. Finally, an acceptable agreement (kappa 0.20 to 0.45) was obtained for energy and most nutrients for both adolescents and adults.
In the present study there are some limitations that must be considered. Biomarkers have often been suggested as the "gold standard" for energy and some nutrients, but due to the viability and financial limitations, like most validation studies,4 we selected the 24-hour dietary recall as the reference method. Despite other dietary methods, like diet records, have been suggested as a reference method, in a review on the validations of FFQs, Cade and collegues4 found that 75% of the studies validated FFQs against repeated 24DRs. Even though we extensively trained interviewers, we recognize that both 24DR and SFFQ have some error sources, such as the reliance on memory and the perception of portion size.1 However, the SFFQ stresses usually long-term memory, whereas 24DR relies on short-term memory. Additionally, the 24DR instrument was interviewer-based using open-ended questions, while the SFFQ was administered with close-ended questions. Such differences let us assume that errors between methods are sufficiently independent and that the 24DR is a satisfactory method for this target instrument.24,35 To estimate long-term usual intake, collection of three-to-four days of recalls in each season of the year has been considered as ideal.1 In our study, two 24-hour dietary recalls were used as comparison method; therefore, the estimate of intake may have been closer to true intake if we had collected more days of food consumption. Regarding micronutrients, it has been proposed that the number of days which must be examined to allow a true estimation of average daily intake is greater for micronutrients than for macronutrients and surpasses the two days evaluated in this study.36 However, other studies enhanced the possibility of using only a small number of replicate measures for the reference method combined with a statistical adjustment to remove the effects of within-person variation.28 In this respect, some authors have suggested that the greatest statistical efficiency is obtained with only two, and at the most five, duplicates per subject.10,20 In this context, to validate our SFFQ against two 24DRs seems to be adequate. Another limitation of our study is that we did not administer the SFFQ twice, thus we cannot evaluate the reproducibility of the instrument. For this reason, future effort needs to be done to assess the reproducibility of this SFFQ.
There is no single perfect way of developing an SFFQ or measuring its validity. However, in general, the methods implemented in the present study, including sample size; selection of population; SFFQ structure, like number of food items; and statistical methods, were consistent with commonly accepted practices.
In conclusion, the SFFQ used in the Ensanut 2012 was found to be a suitable tool for the assessment of energy and dietary intake of nutrients by Mexican adolescents and adults, especially for ranking them according to their nutrient intake. The present SFFQ might be a useful instrument in large epidemiological studies with a focus on diet as a risk factor for various health outcomes. Finally, further efforts should be made to evaluate the reproducibility of the SFFQ.

