











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkComplications and premature mortality can be minimised by interventions to keep glycaemic control under target levels as stipulated in clinical guidelines.1,2 The management of type 2 diabetes is broad and complex, including diet, exercise, education, oral antidiabetic medications, and insulin.3-6 Good diabetes management and good glycaemic control requires that patients both receive high quality clinical care and achieve effective self-management. 7
Previous studies have focused on specific aspects of self-management, such as diet and exercise,8 medication adherence,9,10 or specific aspects of quality of care, such as continuity of care.8 Very few observational studies have measured both self-management and quality of care at the same time,8,9 and most randomised controlled trials focusing on diabetes have not assessed the relative importance of these components.11-13
The objective of this study is to examine the individual contribution and relative importance of selfmanagement and quality of care in the prediction of glycaemic control at six-month follow-up in patients with type 2 diabetes.
Materials and methods
Participants were recruited from the Mexican Institute for Social Security (Instituto Mexicano del Seguro Social IMSS) in the city of Aguascalientes, Mexico (December 2009 to April 2010). Eligible participants were adults (≥40 years old), diagnosed with type 2 diabetes for at least 1 year and under consecutive IMSS care with a monthly prescription of oral glucose-lowering medications but no insulin prescription. This study was based on a model (Figure 1) including multiple measures of both quality of care and self-management related to glycaemic control.
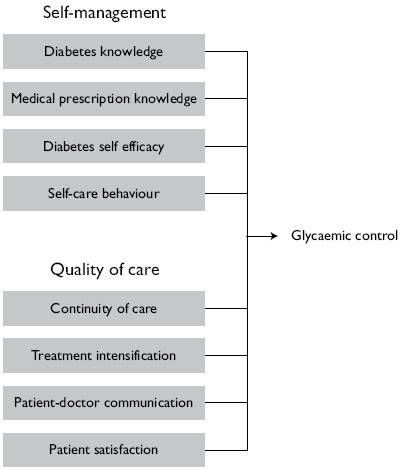
Source: reference 14
Figure 1 Model of predictors of glycaemic control in patients with type 2 diabetes. Aguascalientes, Mexico, December 2009 - April 2010
Data was collected prospectively. Self-management (SM), quality of care (QoC), clinical and demographic variables were measured at baseline.14 SM measures: Diabetes Knowledge Questionnaire (DKQ-24),15 Medical Prescription Knowledge Questionnaire (MPKQ),16 Diabetes Self-Efficacy (DSE) scale,17 and Summary of Diabetes Self-Care Activities (SDSCA).18 SDSCA was transformed to a total score using four items: healthy eating plan, physical activity, foot care, and taking medications ('good' diabetes self-management: ≥3 behaviours ≥4 days per week). QoC measures: Continuity item from the General Practice Assessment Questionnaire (GPAQ),19 Treatment intensification,9 Patient-Doctor Communication Scale,20 and Patient Satisfaction with Diabetes Care.21 Treatment intensification was evaluated from medical records using the availbale blood glucose measure (fasting blood glucose [FBG] or glycated hemoglobin [HbA1c]) given prioprity to HbA1c. Appropriate treatment intensification was assumed when general practitioners (GP) intensified treatment if necessary (patient had FBG >130 mg/dl [7.2 mmol/l] or HbA1c >7.0%) or didn't intensify treatment if it was not necessary (patient had FBG ≤130 mg/dl [7.2 mmol/l] or HbA1c ≤7.0%).
Age, gender, marital status, level of education, occupation, comorbidities, complications, duration of diabetes in years, and depression22 were collected from interviews. HbA1c was measured in all participants at baseline and follow-up as part of this study. Body mass index (BMI) and current medical prescription (oral glucose-lowering medications) were extracted from medical records.
This study complies with the principles of the Helsinki Declaration. Written informed consent was obtained at recruitment with approval of the Ethics Committee of Research on Human Beings at the University of Manchester (ref 09121) and from the IMSS Local Health Research Committee N° 101 (R-2009-101-12).
Sample size and selection
Assuming a correlation between SM and QoC of 0.1, an intra-cluster correlation of 0.1 [recognising that outcomes of patients at the same practice may not be independent, given that they consult the same GP(s)] and 20% loss to follow-up at six months, a sample of 405 patients would enable a difference as small as 0.2 (e.g. 0.25 vs. 0.05) to be detected between the correlations of HbA1c/SM and HbA1c/QoC with approximately 75% power at the 5% level of significance.23,24
Given the time and financial constraints of the study, it was decided that 80% of patients would be selected using a consecutive sample (all eligible patients attending an appointment would be approached). For the remaining 20% of the sample, a random sample of patients was also taken to evaluate selection bias. It was ensured that at least one patient per GP was selected. Any differences between the two samples were controlled for in the analyses.
Statistical analysis
Baseline data was summarised using descriptive statistics. First, univariate linear regressions were examined to evaluate the individual contribution of SM and QoC to glycaemic control (HbA1c at follow-up). Second, a multivariate model was then fitted to determine their relative importance. The analysis was repeated controlling for HbA1c at baseline, practice, sampling method, demographic and clinical characteristics. Third, HbA1c at baseline was removed from the model because it was strongly associated with HbA1c at follow-up. We assumed that this strong association could have covered weaker but clinically relevant associations. Continuous variables were centred at their mean value in order to minimise multicollinearity in the presence of interactions.25 Given that independent variables can be measured in different units, the estimated coefficients (β) were standardised to identify which independent variables have a greater effect on the dependent variable HbA1c at followup. By comparing the coefficients associated with SM and QoC from univariate and multivariate regressions, it was possible to examine their individual contribution to HbA1c, as well as their relative importance.
HbA1c had a skewed distribution. Therefore, bootstrapping, free from parametric assumptions, was used to derive estimates of error variance for tests of statistical significance, using 10 000 bootstrap samples of data from the original dataset.26 An β-level of 0.05 was selected for significance for all statistical tests.
Results
Recruitment
Figure 2 shows a CONSORT diagram outlining recruitment. Two hundred and seventy patients agreed to participate in the study, attended the laboratory, and completed interviews. There were 45 exclusions (mainly incomplete data from medical records to evaluate treatment intensification). Twenty two participants were lost at follow-up (10%). The final sample analysed was 204 patients.
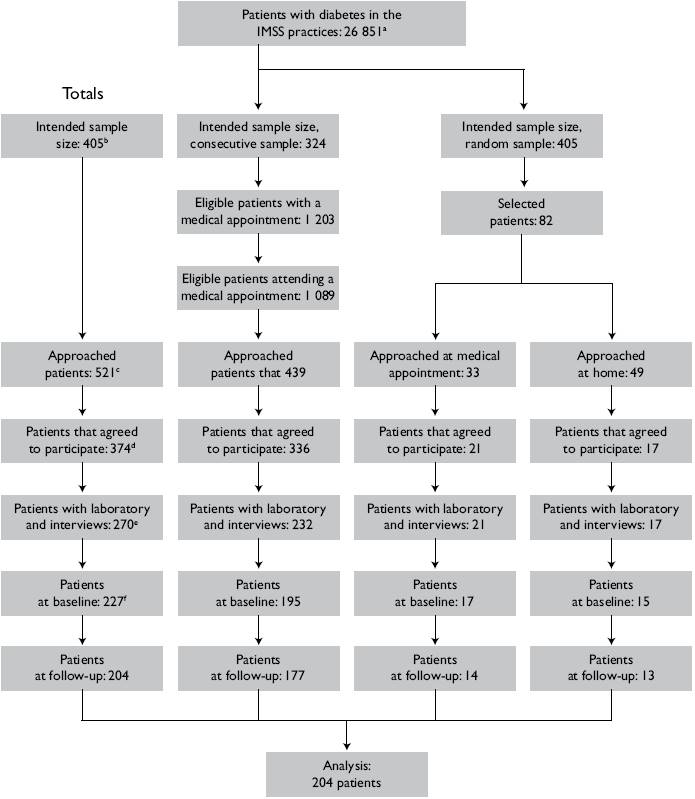
Sample size for the analysis was 204 patients. This sample represents: (a) 0.8% of patients with diabetes; b) 51% of the intended sample; (c) 39% of approached patients;(d) 55% of patients who agreed to participate; (e) 76% of patients with laboratory and interview data; (f) and 90% of patients at baseline
Source: Reference 27
Figure 2 CONSORT diagram. Glycaemic control in type 2 diabetes. Aguascalientes, Mexico (December 2009 - April 2010)
Demographic and clinical characteristics
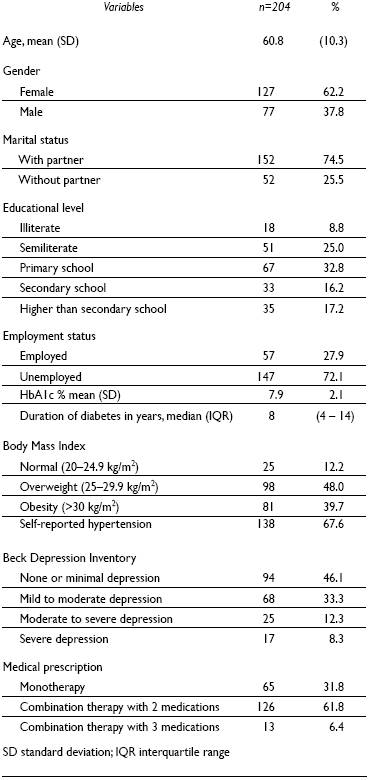
Mean age was 60.8 years; 62% were female, 75% had a partner, 67% had at best primary school and 72% were not in paid employment (Table I). Median duration of diabetes was eight years, 48% were overweight, 40% were obese, 68% self-reported hypertension, 54% had depression, and 68% were prescribed more than one oral glucose lowering medication. Mean HbA1c at baseline was 7.9% and 8.3% at follow-up (SD 2.0).
Self-management
Mean score of DKQ-24 was 15.8 (SD 3.6); 25% of patients answered ≥80% of the questions correctly. Thirty one percent of patients were classified as having 'strong' knowledge of their medical prescription. The mean score of DSE was 7.0 (SD 1.7) and 55% of patients scored ≥7 on this scale. Over half of the participants (57%) reported good diabetes self-management behaviours.
Quality of care
GP appropriately intensified treatment in just over half of the sample (58%). Eighty-six percent of patients selfreported being seen by their usual GP 'a lot of the time', 'almost always' or 'always'. One hundred and forty one patients (69%) reported good communication with their GPs (scoring ≥4 in the Patient-Doctor Communication Scale), but only 34 patients (17%) were satisfied with their diabetes care (scoring ≥4 in the Patient Satisfaction with Diabetes Care).
Statistical modelling - multivariate including HbA1c at baseline
The multivariate linear regression model, that included all variables, explained 41% of the variation in HbA1c at follow-up (Table II). A 1% increase in HbA1c at baseline (e.g. from 7% to 8%) was significantly associated with a 0.59% increase in HbA1c at follow-up (95% CI 0.46 to 0.72, P <0.01). The 10-year increase in diabetes duration was significantly associated with 0.3% increase of HbA1c (95% CI 0.02 to 0.7, P <0.05). Combination therapy was still significantly associated with HbA1c at follow-up(0.63%,95%CI0.09to1.17,P<0.05);however, in the univariate analysis, this association was stronger (1.4% increase of HbA1c, 95% CI 0.88 to 2.01 P <0.01).

Statistical modelling - multivariate without HbA1c at baseline
When HbA1c at baseline was removed from the model, appropriate treatment intensification was a significant predictor (Table II). This model explained 14% of thevariation in HbA1c at follow-up. HbA1c levels were significantly lower (0.65% reduction of HbA1c) in patients receiving appropriate treatment intensification (95% CI −1.23 to −0.07, P <0.05).
A significant interaction was found between SM behaviours and treatment intensification and it is shown in Figure 3 (β = 0.21, P <0.05). Controlling for HbA1c at baseline, this interaction suggests that if treatment is not intensified appropriately, effective SM can result in reduced HbA1c. Whereas when treatment is appropriately intensified, SM behaviour appears to make little, if any, difference to HbA1c.
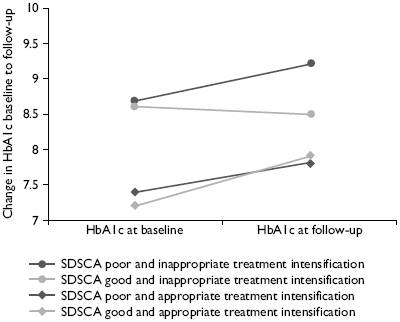
SDSCA poor = 0 to 2 self-management behaviours ≥4 days/week; SDSCA good = 3 or 4 self-management behaviours ≥4 days/week; inappropriate treatment intensification = GP didn't intensify treatment when necessary (patient had fasting blood glucose >130 or HbA1c >7.0) or GP intensified treatment when not necessary (patient had fasting blood glucose ≤130 or HbA1c ≤7.0); appropriate treatment intensification = GP intensified treatment when necessary (patient had fasting blood glucose >130 or HbA1c >7.0) or GP didn't intensify treatment when not necessary (patient had fasting blood glucose ≤130 or HbA1c ≤7.0)
Figure 3 Interaction between self-management behaviours (SDSCA) and treatment intensification in their association with change in HbAIc from baseline to follow-up. Aguascalientes, Mexico (December 2009 - April 2010)
Discussion
This study suggests that QoC (treatment intensification) was more important than SM as a predictor of glycaemic control at six months follow-up, at least in the context of Mexican primary care. Treatment intensification was significant only if HbA1c at baseline was not controlled for.
The effect of treatment intensification has been reported previously.9,28-31 Treatment intensification was extracted from medical records in this study. We acknowledge that medical records might have not been fully completed by GPs. This measure is also limited because it deals only with increases in dosage or the addition of more medications but does not take into account the trade-offs between risks and benefits of intensifying medications. The aim of treatment intensification in diabetes is to achieve recommended HbA1c levels, with a target level of <7% in Mexico.4 The American Diabetes Association suggests the same target except in the presence of a history of severe hypoglycaemia, limited life expectancy, advanced diabetes complications, and multiple comorbidities (recommending to achieve 'less-stringent' HbA1c <8%).3 Medical records lack the necessary information to identify patients who are not appropriate candidates (e.g. history of severe hypoglycaemia) or refuse treatment intensification. Previous studies have encountered the same limitation.9,29,32,33
The analyses for this study were undertaken on the assumption that treatment intensification in the context of raised HbA1c was generally an appropriate measure of QoC. However, it is possible that treatment intensification could be associated with reductions in quality of life among patients if it leads to additional burden or anxiety. We did not measure quality of life and were therefore unable to assess any impact on it. Other measures could have confounded the results like changes in body weight and adherence to treatment but these were not measured either.
Treatment intensification had an effect on HbA1c at follow-up when HbA1c at baseline was not included in the analysis but duration of diabetes and combination therapy remained significant. It has been suggested that glycaemic control deteriorates overtime due to pancreatic β-cell dysfunction34,35 and therefore multiple therapies are required.36 This might be why patients with longer duration of diabetes had higher HbA1c levels and were under combination therapy. Twelve of the participants were under combination therapy with three medications and above treatment targets (HbA1c >7.0%). They were potential candidates for insulin treatment.
The findings of this study showed that none of the SM predictors were associated with HbA1c at follow-up. Systematic reviews and meta-analysis of RCTs have reported variable results: significant effects of SM interventions on SM behaviours as well as on glycaemic control, effects on SM but no consequent effect on glycaemic control, and effects of SM interventions on glycaemic control without demonstrating any effects on SM.13,37-39 For our study, it might be possible that the lack of power concealed an association between SM and glycaemic control. Furthermore, social desirability might have affected participants' report of SM behaviours. Participants might have reported behaviours that they did not actually do. The National Health Survey in Mexico found that less than 30% of adults with diabetes reported having a diet or doing exercise40 which is lower than the percentage of SM behaviours reported in our study.
Secondary analyses did suggest an interaction between SM behaviours and treatment intensification. In patients who did not receive treatment intensification when indicated, greater numbers of SM behaviours predicted significantly lower HbA1c at follow-up. This interaction has not been reported previously which suggests a hypothesis to test in future research.
There are limitations in the study. Half of the participants were not included in the analysis because they did not agree to participate, did not attend blood test, or were lost to follow-up. It is possible that nonparticipants might have had different SM and QoC characteristics, but lacking data on non-respondents, we could not analyse their characteristics. Some nonparticipants reported that they did not have time to attend blood tests and interviews, and these patients may be less keen on performing SM and attending medical appointments. There were some differences between consecutive and random samples which were controlled in the multivariate model along other variables. The intended sample size was 405 participants, 270 attended laboratory and interviews but had incomplete data in their medical records; the total analysis sample was 204 patients. This sample size was still sufficient to provide 70% power to detect the required difference in correlations, assuming a correlation of 0.3 between SM and QoC. The average follow-up time was 5.8 months. It is likely that a more noticeable change would be observed with a longer follow-up period.
The approach taken in this longitudinal cohort study has significant strengths. The study measured various aspects of both SM and QoC, a comprehensive approach which has not been reported in the literature up to now. The analysis allowed statistical control for relevant covariates (demographic and clinical), and the follow-up rate of 90% was higher than the recommended acceptable rate of 80% meaning that the risk of bias due to attrition was small.41,42
Conclusion
Treatment intensification was the main predictor of lower HbA1c levels at follow-up, when HbA1c at baseline was not controlled for, suggesting that QoC was more important than SM as a predictor of glycaemic control. Although none of the SM predictors was significantly related to HbA1c, an exploratory interaction showed that patients who did not receive treatment intensification when they needed it and performed more SM behaviours had lower HbA1c levels at follow-up.

